
Rationale and Objectives
To evaluate the diagnostic accuracy of a 3-T magnetic resonance imaging (MRI) system with a phased-array coil (3T MRI) in the local staging of prostatic cancer.
Materials and Methods
Between July 2004 and September 2007, 59 patients (mean age 66 years) with a histologic diagnosis of prostatic cancer underwent 3-T MRI with a phased-array coil. A total of 42/59 patients underwent a radical prostatectomy within 3 weeks of the MRI examination. Two radiologists with differing experience in the interpretation of prostatic imaging used a 1–5 scale score to assess extracapsular spread, seminal vesicle and neurovascular bundle infiltration, and prostatic apex involvement. The anatomopathologic examination conducted on histologic macrosections was the reference test used to evaluate the results of 3-T MRI. Interobserver reliability was assessed using the k value.
Results
The sensitivity, specificity, and accuracy values obtained by the expert radiologist were 68%, 92%, and 83%, respectively, compared to 50%, 85%, and 71% for the identification of extracapsular spread and 81%, 62%, and 84% compared to 63%, 50%, and 55% for apex involvement. Interobserver reliability was good (k = 0.71). Seminal vesicle infiltration was correctly identified in four of five cases and neurovascular bundle infiltration was identified in four of four cases.
Conclusions
Despite presenting diagnostic accuracy values lower than those reported in literature using 1.5-T endorectal coil MRI, the use of 3-T MRI with a phased-array coil could constitute a valid alternative to MRI techniques using endorectal coils in selected patients. Direct comparative studies between the two methods on large caseloads are required to confirm this hypothesis.
Although its use has yet to be univocally accepted in the urology sector and it presents artifact-related, technical, and methodologic problems, endorectal coil magnetic resonance imaging (erMRI) using 1.5-T magnets is still considered the most accurate imaging technique in the local staging of prostate cancer ( ). In recent years, MRI appliances with field intensities of 3 T (3-T MRI) or higher that guarantee an outstanding signal-to-noise ratio, on account of the significant increase in the signal that can be obtained compared to 1.5-T appliances, have become commonplace. A number of recently published works have assessed the results that can be obtained using 3-T MRI, both with a phased-array coil and an endorectal coil, in terms of image quality and diagnostic accuracy in evaluating prostate cancer ( ). The results of these evaluations are contrasting; some authors ( ) confirm that erMRI remains the technique of election for prostate cancer staging, whereas others ( ) argue that the performance of 3-T MRI with phased-array coils is comparable to that of erMRI, without the drawbacks, costs, and artifacts connected to the endorectal coil technique.
The aim of our study is to evaluate the diagnostic accuracy of 3-T MRI with phased-array coils in the local staging of prostatic cancer.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
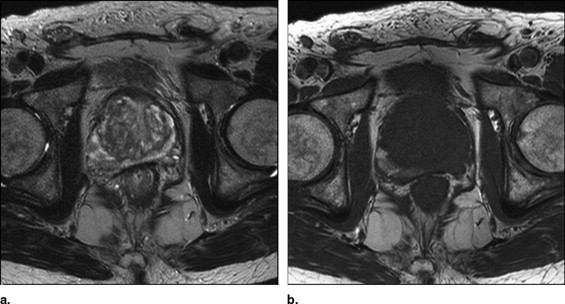
Extracapsular Extension
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Comparative Evaluation of Extraprostatic Spread and Matched Values of Diagnostic Accuracy
Capsule Expert Radiologist Less Expert Radiologist Involved Spared Involved Spared Pathology Involved 11 5 8 8 Spared 2 24 4 22 Sensitivity (%) 68 50 Specificity (%) 92 85 PPV (%) 85 67 NPV (%) 83 73 Accuracy (%) 83 71 K 0.70
NPV: negative predictive value; PPV: positive predictive value.
Get Radiology Tree app to read full this article<
Seminal Vesicle Infiltration
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Neurovascular Bundle Infiltration
Get Radiology Tree app to read full this article<
Prostatic Apex Involvement
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparative Evaluation of Involvement of Glandular Apex and Matched Values of Diagnostic Accuracy
Apex Expert Radiologist Less Expert Radiologist Involved Spared Involved Spared Pathology Involved 13 3 10 6 Spared 10 16 13 13 Sensitivity (%) 81 63 Specificity (%) 62 50 PPV (%) 57 44 NPV (%) 84 68 Accuracy (%) 69 55 K .71
NPV: negative predictive value; PPV: positive predictive value.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Schnall M.D., Imai Y., Tomaszewski J., et. al.: Prostate cancer: local staging with endorectal surface coil MR imaging. Radiology 1991; 178: pp. 797-802.
2. Futterer J.J., Engelbrecht M.R., Hiusman H.J., et. al.: Staging prostate cancer with dynamic contrast-enhanced endorectal MR imaging prior to radical prostatectomy: experienced versus less experienced readers. Radiology 2005; 237: pp. 541-549.
3. Mullerad M., Hricak H., Wang L., et. al.: Prostate cancer: detection of extracapsular extension by genitourinary and general body radiologists at MR imaging. Radiology 2004; 232: pp. 140-146.
4. Quinn S.F., Branzini D.A., Demlow T.A., et. al.: MR imaging of prostate cancer with an endorectal coil technique: correlation with whole-mount specimens. Radiology 1994; 190: pp. 323-327.
5. Werner-Wasik M., Whittington R., Malkowicz S.B., et. al.: Prostate imaging may not be necessary in nonpalpable carcinoma of the prostate. Urology 1997; 50: pp. 385-389.
6. Jager G.J., Severens J.L., Thornbury J.R., et. al.: Prostate cancer staging: should MR imaging be used? —A decision analytic approach. Radiology 2000; 215: pp. 445-451.
7. Presti J.C., Hricack H., Narayan P.A., et. al.: Local staging of prostatic carcinoma comparison of transrectal sonography and endorectal MR imaging. AJR Am J Roentgenol 1996; 166: pp. 103-108.
8. Tempany C.M., Zhon X., Zerhouni E.A., et. al.: Staging of prostate cancer: results of radiology diagnostic oncology group project comparison of three MR imaging techniques. Radiology 1994; 192: pp. 47-54.
9. Hirose M., Bharatha A., Hata N., et. al.: Quantitative MR imaging assessment of prostate gland deformity before and during MR imaging guided brachytherapy. Acad Radiol 2002; 9: pp. 906-912.
10. Maio A., Rifkin M.D.: Magnetic resonance imaging of prostate cancer: Update. Top Magn Reson Imaging 1995; 7: pp. 54-68.
11. Rouviere O., Hartman R.P., Lyonnet D.: Prostate MR imaging at high-field strenght: evolution or revolution?. Eur Radiol 2006; 16: pp. 276-284.
12. Uematsu H., Takahashi M., Dougherty L., et. al.: High field body MR imaging preliminary experiences. J Clin Imaging 2004; 28: pp. 159-162.
13. Futterer J.J., Scheenen T.W.J., Huisman H.J., et. al.: Initial experience of 3T endorectal coil MR imaging and 1H-spectroscopic imaging of the prostate. Invest Radiol 2004; 39: pp. 671-680.
14. Schick F.: Whole body MRI at high field: technical limits and clinical potential. Eur Radiol 2005; 15: pp. 946-959.
15. Ocak I., Bernardo M., Metzger L., et. al.: Dynamic contrast-enhanced MRI of prostate cancer at 3T: a study of pharmacokinetic parameters. AJR Am J Roentgend 2007; 189: pp. 849-851.
16. Bloch B.N., Rofsky N.M., Baroni R.H., et. al.: 3 Tesla magnetic resonance imaging of the prostate with combined pelvic phased-array and endorectal coils: initial experience. Acad Radiol 2003; 11: pp. 863-867.
17. Bartha R., Drost D.J., Menon R.S., et. al.: Comparison of the quantification precision of human short echo time H spectroscopy at 1.5 and 4.0 Tesla. Magn Reson Med 2000; 44: pp. 185-192.
18. De Bazelaire C.M.J., Duhamel G.D., Rofsky N.M., et. al.: MR imaging relaxation times of abdominal and pelvic tissues measured in vivo at 3.0T: preliminary results. Radiology 2004; 230: pp. 652-659.
19. Takahashi M., Uematsu H., Hatabu H.: MR imaging at high magnetic fields. Eur J Radiol 2003; 46: pp. 45-52.
20. Beyersdorff D., Taymoorian K., Knosel T., et. al.: MRI of prostate cancer at 1.5 and 3.0 T: comparison of image quality in tumor detection and staging. AJR Am J Roentgenol 2005; 185: pp. 1214-1220.
21. Sosna J., Pedrosa I., Dewolf W.C., et. al.: MR imaging of the prostate at 3 Tesla: comparison of an external phased-array coil to imaging with an endorectal coil at 1.5 Tesla. Acad Radiol 2004; 11: pp. 857-862.
22. Torricelli P., Cinquantini F., Ligabue G., et. al.: Comparative evaluation between external phased array coil at 3 T and endorectal coil at 1.5 T. J Comput Assist Tomogr 2006; 30: pp. 355-361.
23. D’Amico A., Whittington R., Schnall M., et. al.: The impact of the inclusion of endorectal coil magnetic resonance imaging in a multivariate analysis to predict clinically unsuspected extraprostatic cancer. Cancer 1995; 75: pp. 2368-2372.
24. Landis J.R., Koch G.C.: The measurement of observer agreement for categorical data. Biometrics 1977; 33: pp. 159-174.
25. Coakley F., Qayyum A., Kurhanewicz J.: Magnetic resonance imaging and spectroscopic imaging of prostate cancer. J Urol 2003; 170: pp. 69-75.
26. Sala E., Akin O., Moskowitz C.S., et. al.: Endorectal MR imaging in the evaluation of seminal vesicle invasion: diagnostic accuracy and multivariate feature analysis. Radiology 2006; 238: pp. 929-937.
27. Cornud F., Flam T., Chauveinc L., et. al.: Extraprostatic spread of clinically localized prostate cancer: factors predictive of pT3 tumor and of positive endorectal MR imaging examination results. Radiology 2002; 224: pp. 203-210.
28. Manzone T., Malkowicz S.B., Tomaszewski J.E., et. al.: The use of endorectal MR imaging to predict prostate carcinoma recurrence after radical prostatectomy. Radiology 1998; 209: pp. 537-542.
29. Futterer J.J., Heijmink S.W.T.P.J., Scheenen T.W.J., et. al.: Prostate cancer: local staging at 3-T endorectal MR imaging-Early experience. Radiology 2006; 238: pp. 184-191.
30. Stamey T.A., Villers A.A., McNeal J.E., et. al.: Positive surgical margins at radical prostatectomy: importance of the apical dissection. J Urol 1990; 143: pp. 1183-1187.
31. Kim C.K., Park B.K., Kim B.: Localization of prostate cancer using 3T MRI. J Comput Assist Tomogr 2006; 30: pp. 7-11.
32. D’Amico A., Whittington R., Malkowicz , et. al.: Role of percent positive biopsies and endorectal coil MRI in predicting prognosis in intermediate-risk prostate cancer patients. Cancer J Sci Am 1996; 2: pp. 343-350.
33. Wang L., Mullerad M., Chen H.N., et. al.: Prostate cancer: incremental value of endorectal MR imaging findings for prediction of extracapsular extension. Radiology 2004; 232: pp. 133-139.
34. Sonnad S.S., Langlotz C.P., Schwartz J.S.: Accuracy of MR imaging for staging prostate cancer: a meta-analysis to examine the effect of technologic change. Acad Radiol 2001; 8: pp. 149-157.
35. Wang L., Hricak H., Kattan M.W., et. al.: Prediction of organ-confined prostate cancer: incremental value of MR imaging and MR spectroscopic imaging to staging nomograms. Radiology 2006; 238: pp. 597-603.
36. Yu K.K., Scheidler J., Hricak H., et. al.: Prostate cancer: prediction of extracapsular extension with endorectal HR imaging and three-dimensional proton MR spectroscopic imaging. Radiology 1999; 213: pp. 481-488.