
Rationale and Objectives
The purpose was to verify whether myocardial viability can be detected by a delayed enhancement magnetic resonance imaging (MRI) approach using a rapid three-dimensional inversion-recovery fast low-angle shot (3D IR-FLASH) sequence in a preclinical and clinical setting.
Materials and Methods
Nonreperfused myocardial infarctions were induced in eight minipigs. Both the pigs and 15 patients with suspected myocardial infarction underwent MRI using a rapid 3D IR-FLASH sequence and a two-dimensional IR-FLASH sequence as the reference standard.
Results
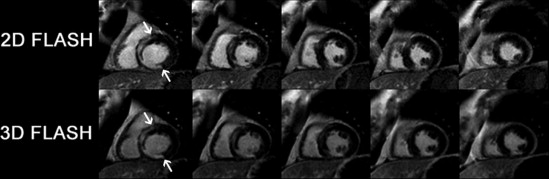
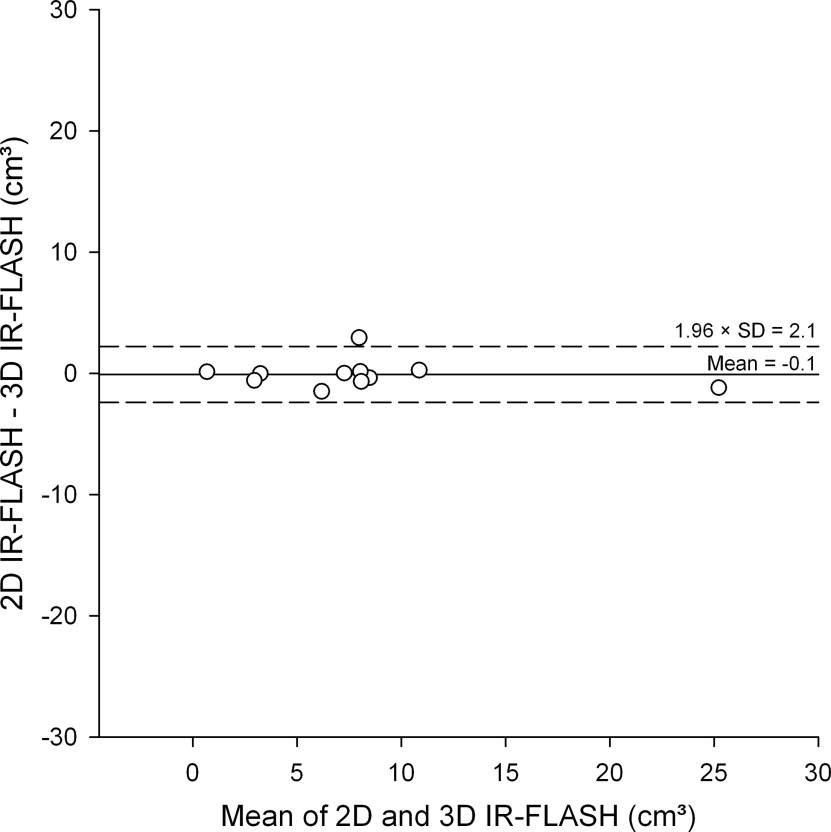
In the pigs, a total of 52 segments with myocardial infarction were identified with both sequences and there was good agreement in transmurality of 99.5%. The infarction volume determined with the 3D IR-FLASH in the animal study (2.4 ± 1.5 cm 3 ) showed a good correlation with the histomorphometrically determined volume using triphenyltetrazolium chloride (2.3 ± 1.2 cm 3 , r = 0.98, P < .001) and the two-dimensional IR-FLASH sequence (2.3 ± 1.4 cm 3 , r = 0.99, P < .001). Eleven of 15 patients were found to have myocardial infarction in 37 myocardial segments with both sequences and there was a good agreement in transmurality of 98.8%. There was also a good correlation in the clinical study between the 3D and 2D sequences (6.9 ± 6.7 cm 3 vs. 6.8 ± 6.5 cm 3 , r = 0.98, P < .001). In Bland-Altman analysis there was no significant under- or overestimation of the myocardial infarction volume using the 3D IR-FLASH sequence in comparison to the two-dimensional reference standard in both the preclinical and clinical study. The contrast-to-noise ratios were not significantly different between 3D and 2D sequences in the animal (34.7 ± 1.5 vs. 33.8 ± 2.6; P = .51) and clinical study (31.4 ± 12.5 vs. 36.7 ± 11.5; P = .31). The breathhold time for the 3D IR-FLASH sequence in the clinical study (20.4 ± 2.2 s) was significantly shorter than that of the 2D IR-FLASH sequence (190.1 ± 20.8 s, P < .001).
Conclusions
The rapid 3D IR-FLASH sequence detects myocardial infarction with high accuracy and allows a relevant reduction in acquisition time.
The demonstration of myocardial viability is important for the diagnosis, therapeutic decision, and evaluation of the outcome of medical and surgical treatment. In the last few years, magnetic resonance imaging (MRI) has become more important in analyzing left ventricular myocardial viability ( ). An accurate assessment of the transmurality of myocardial infarction is only possible with the high spatial resolution of delayed-enhancement MRI ( ). The transmurality of myocardial infarction is crucial for the prognosis and the reconstitution of contractile function of the left ventricle ( ). The reference standard for delayed-enhancement MRI is a two-dimensional (2D) inversion-recovery fast low-angle shot sequence (IR-FLASH) ( ). The main drawback of this technique is the long acquisition time of 10–14 heartbeats for one single slice ( ). As a consequence, 10–16 breathholds each lasting at least 10 heartbeats are necessary to cover the entire left ventricle on short-axis orientation using this 2D approach. Therefore the purpose of our study to evaluate the correlation and accuracy of a rapid three-dimensional (3D) IR-FLASH sequence in comparison to the reference standard sequence (2D IR-FLASH) for noninvasive assessment of myocardial viability in pigs (with histopathologic correlation) and patients.
Materials and methods
Experimental Study and Instrumentation
In eight minipigs (weighing 22.6 ± 3.1 kg), anesthesia was induced using 15 mg/kg ketamine hydrochloride IM (Ketamine 500 mg, Curamed Pharma GmbH, Karlsruhe, Germany), 0.2 mg/kg droperidol IM (Dehydrobenzperidol, Janssen-Cilag GmbH, Neuss, Germany), and 0.2 mg/kg midazolam hydrochloride IM (Dormicum, Hoffmann-La Roche AG, Grenzach-Whylen, Germany) followed by 5–7 mg/kg/h propofol IV (Disoprivan 1%, AstraZeneca, Wedel, Germany) and maintained by ventilation for the entire instrumentation period (approximately 60 min) with 2–5% isoflurane (Forene, Abbott GmbH, Wiesbaden, Germany). Nonreperfused myocardial infarction was induced with a closed-chest model ( ): with a multipurpose catheter (Multipurpose, 6F, XBR 2, Vistabrite Tip, 80 cm, Miami, FL) tungsten spirals with a length of 4–6 cm (Spirale n detachable en tungstene, Balt Extrusion, Montmorency, France) were flushed with saline into the left circumflex coronary artery to induce nonreperfused myocardial infarction. Immediately after MRI, the animals were euthanized under deep anesthesia with intravenous injection of 5 mL of a commercially available mixture of tetracaine hydrochloride (5 mg/mL), mebezonium iodide (50 mg/mL), and embutramide (200 mg/mL) (T61; Intervet Deutschland, Unterschleissheim, Germany). Subsequently, the hearts were removed and stiffened by repetitive immersion in 95% ethanol precooled to −80°C and sliced from base to apex into 5-mm thick sections. These sections were incubated in 2% triphenyltetrazolium chloride (TTC) for 20 minutes at 37°C to define the infarcted areas (= regions that failed to stain brick-red). These slices were scanned with a flat bed scanner. An observer measured infarction sizes (in cm 3 ) in the TTC-stained slices. The care and treatment of animals was according to legal requirements and all experiments performed were approved by the responsible state authority.
Clinical Study
Get Radiology Tree app to read full this article<
MRI Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Experimental Study
Get Radiology Tree app to read full this article<
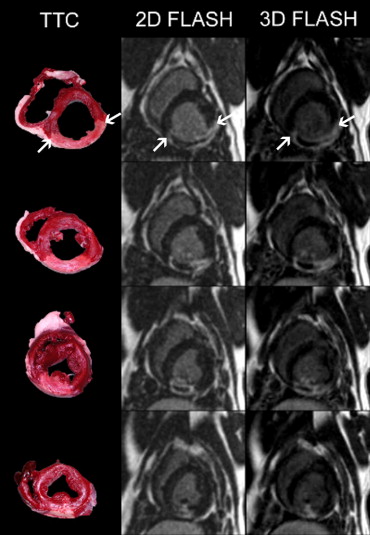
Table 1
Comparison of Contrast-to-Noise Ratios using the Two Sequences
Contrast-to-Noise Ratios 2D IR-FLASH 3D IR-FLASH_P_ Experimental study 33.8 ± 2.6 34.7 ± 1.5 .51 Clinical study 36.7 ± 11.5 31.4 ± 12.5 .31
2D: two-dimensional; 3D: three-dimensional; IR-FLASH: inversion-recovery fast low-angle shot.
Get Radiology Tree app to read full this article<
Clinical Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Elliott M.D., Kim R.J.: Late gadolinium cardiovascular magnetic resonance in the assessment of myocardial viability. Coron Artery Dis 2005; 16: pp. 365-372.
2. Wagner A., Mahrholdt H., Holly T.A., et. al.: Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet 2003; 361: pp. 374-379.
3. Kim R.J., Wu E., Rafael A., et. al.: The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med 2000; 343: pp. 1445-1453.
4. Simonetti O.P., Kim R.J., Fieno D.S., et. al.: An improved MR imaging technique for the visualization of myocardial infarction. Radiology 2001; 218: pp. 215-223.
5. Dewey M., Kaufels M., Laule M., et. al.: Magnetic resonance imaging of myocardial perfusion and viability using a blood pool contrast agent. Invest Radiol 2004; 39: pp. 498-505.
6. Barkhausen J., Ebert W., Debatin J.F., Weinmann H.J.: Imaging of myocardial infarction: comparison of Magnevist and gadophrin-3 in rabbits. J Am Coll Cardiol 2002; 39: pp. 1392-1398.
7. Cerqueira M.D., Weissman N.J., Dilsizian V., et. al.: Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Circulation 2002; 105: pp. 539-542.
8. Fox C.S., Evans J.C., Larson M.G., et. al.: Temporal trends in coronary heart disease mortality and sudden cardiac death from 1950 to 1999: the Framingham Heart Study. Circulation 2004; 110: pp. 522-527.
9. Kühl H.P., Papavasiliu T.S., Beek A.M., et. al.: Myocardial viability: rapid assessment with delayed contrast-enhanced MR imaging with three-dimensional inversion-recovery prepared pulse sequence. Radiology 2004; 230: pp. 576-582.
10. Foo T.K., Stanley D.W., Castillo E., et. al.: Myocardial viability: breath-hold 3D MR imaging of delayed hyperenhancement with variable sampling in time. Radiology 2004; 230: pp. 845-851.
11. Tatli S., Zou K.H., Fruitman M., et. al.: Three-dimensional magnetic resonance imaging technique for myocardial-delayed hyperenhancement: a comparison with the two-dimensional technique. J Magn Reson Imaging 2004; 20: pp. 378-382.
12. Carr J., Pereles F., McCarthy R., et. al.: Delayed contrast-enhanced imaging of left ventricular myocardial scarring using single-shot inversion recovery (IR) true-FISP [abstract]. Proc Intl Soc Mag Reson Med 2003; 11: pp. 1612.
13. Dewey M., Laule M., Taupitz M., et. al.: Myocardial viability: assessment with three-dimensional MR imaging in pigs and patients. Radiology 2006; 239: pp. 703-709.
14. Kellman P., Arai A.E., McVeigh E.R., et. al.: Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med 2002; 47: pp. 372-383.
15. Kellman P., Larson A.C., Hsu L.Y., et. al.: Motion-corrected free-breathing delayed enhancement imaging of myocardial infarction. Magn Reson Med 2005; 53: pp. 194-200.
16. Balci N.C., Inan N., Anik Y., et. al.: Low-dose gadobenate dimeglumine versus standard-dose gadopentate dimeglumine for delayed contrast-enhanced cardiac magnetic resonance imaging. Acad Radiol 2006; 13: pp. 833-839.
17. Huber A., Schoenberg S.O., Spannagl B., et. al.: Single-shot inversion recovery TrueFISP for assessment of myocardial infarction. AJR Am J Roentgenol 2006; 186: pp. 627-633.
18. Wintersperger B.J., Nikolaou K., Dietrich O., et. al.: Single breath-hold real-time cine MR imaging: improved temporal resolution using generalized autocalibrating partially parallel acquisition (GRAPPA) algorithm. Eur Radiol 2003; 13: pp. 1931-1936.
19. Schuijf J.D., Kaandorp T.A., Lamb H.J., et. al.: Quantification of myocardial infarct size and transmurality by contrast-enhanced magnetic resonance imaging in men. Am J Cardiol 2004; 94: pp. 284-288.
20. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.