
Rationale and Objectives
The aim of this study was to evaluate the accuracy of measurements of lung volumes reconstructed using three-dimensional computed tomographic (CT) imaging from thin-section multidetector-row CT images compared to standard pulmonary function testing.
Materials and Methods
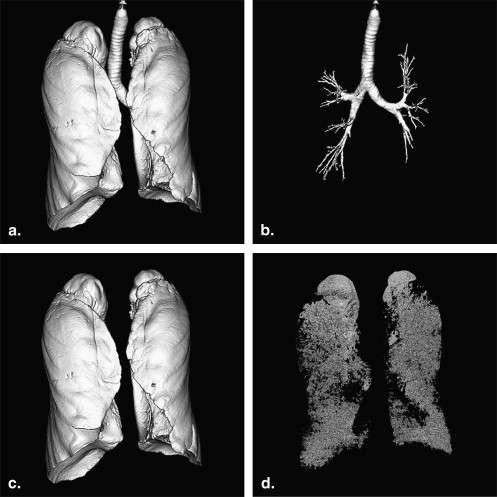
Preoperative three-dimensional CT images and pulmonary function test results of 64 patients with solitary pulmonary nodules who were considered candidates for lung resection were reviewed. On the three-dimensional CT images, total lung capacity (TLC CTV ), emphysematous lung capacity (ELC CTV ), and normal lung capacity (NLC CTV ) were calculated. Total lung capacity (TLC), vital capacity, and forced expiratory volume in 1 second were measured using spirometry.
Results
There was a strong positive correlation between estimated TLC CTV and measured TLC values ( r = 0.87, P < .001). Estimated ELC CTV at the threshold value of −900 Hounsfield units was negatively correlated with forced expiratory volume in 1 second ( r = −0.56, P < .001). NLC CTV values were more strongly correlated with vital capacity values than TLC CTV values ( r = 0.74, P < .001).
Conclusions
Lung volume calculated using three-dimensional CT volumetry was well correlated with lung volume measured using spirometry. Three-dimensional CT volumetry can be used to evaluate pulmonary function.
The incidence and mortality rate of lung cancer have been increasing worldwide. The prognosis is poor, and the most effective treatment is surgical resection, especially for early-stage non–small-cell lung cancer. However, patients with lung cancer often have other respiratory complications, such as chronic obstructive pulmonary disease (COPD) due to smoking, that increase the risks of surgery . Therefore, it is essential to evaluate preoperative respiratory function and to predict postoperative function to exclude patients who will not be able to safely undergo lobectomy or pneumonectomy.
Preoperative pulmonary function has usually been evaluated using spirometry, although several alternative approaches to evaluating pulmonary function using quantitative computed tomographic (CT) imaging have been reported recently . Ueda et al reported that using quantitative CT imaging at a slice thickness of 10 mm in combination with spirometry improved risk prediction in patients undergoing lung lobectomy for cancer. With the recent advances in multidetector-row CT (MDCT) technology, thinner volumetric data can easily be acquired more quickly and used for the evaluation of three-dimensional lung volumes.
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics
Characteristic Value Age (y) 67 (42–85) Sex Male 39 Female 25 Size of nodule (mm) 20.6 (8–30) TLC (L) 5.34 ± 1.23 (3.05–8.02) VC (L) 3.24 ± 0.84 (1.75–5.20) %VC 111.0 ± 18.6 (74.8–156.2) FEV 1.0 (L) 2.18 ± 0.56 (1.12–3.50) FEV 1.0 % 70.2 ± 11.2 (30.6–92.1)
FEV 1.0 , forced expiratory volume in 1 second; TLC, total lung capacity; VC, vital capacity.
Data are expressed as mean ± standard deviation (range).
Get Radiology Tree app to read full this article<
CT Examination
Get Radiology Tree app to read full this article<
Three-dimensional CT Volume Measurement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Function Testing
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Results of Three-dimensional CT Volumetry
Threshold Value (HU) Mean ± SD Range TLC CTV (L) 4.45 ± 1.23 2.29–8.07 ELC CTV (L) −900 0.29 ± 0.50 0.00–2.16 −950 0.08 ± 0.27 0.00–1.94 NLC CTV (L) −900 4.16 ± 0.97 2.29–6.58 −950 4.37 ± 1.16 2.29–7.24
CT, computed tomographic; ELC CTV , emphysematous lung capacity on three-dimensional CT volumetry; HU = Hounsfield units; NLC CTV , normal lung capacity on three-dimensional CT volumetry; SD, standard deviation; TLC CTV , total lung capacity on three-dimensional CT volumetry.
Get Radiology Tree app to read full this article<
TLC CTV Versus TLC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ELC CTV Versus RV
Get Radiology Tree app to read full this article<
TLC CTV and NLC CTV Versus VC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ELC CTV Versus FEV 1.0 %
Get Radiology Tree app to read full this article<
Normal Pulmonary Function Versus Obstructive Pulmonary Function
Get Radiology Tree app to read full this article<
Table 3
Comparisons Between Normal and Obstructive Pulmonary Functions
Characteristic Normal ( n = 35) Obstructive ( n = 29) Age (y) 66 (42–85) 69 (43–81) Sex Male 14 25 Female 21 4 Size of nodule (mm) 19.9 (8–30) 21.3 (11–30) TLC (L) 4.74 ± 1.08 (3.05–7.17) 6.06 ± 1.00 (4.09–8.02) VC (L) 2.92 ± 0.78 (1.75–4.89) 3.63 ± 0.75 (2.47–5.20) %VC 108.1 ± 15.8 (84.5–141.7) 114.5 ± 21.3 (74.8–156.2) FEV 1.0 (L) 2.21 ± 0.60 (1.30–3.50) 2.15 ± 0.51 (1.12–3.02) FEV 1.0 % 78.0 ± 6.0 (70.1–92.1) 60.8 ± 8.3 (30.6–69.7)
FEV 1.0 , forced expiratory volume in 1 second; TLC, total lung capacity; VC, vital capacity.
Data are expressed as mean ± standard deviation (range).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kearney D.J., Lee T.H., Reilly J.J., DeCamp M.M., Sugarbaker D.J.: Assessment of operative risk in patients undergoing lung resection. Importance of predicted pulmonary function. Chest 1994; 105: pp. 753-759.
2. Licker M.J., Widikker I., Robert J., et. al.: Operative mortality and respiratory complications after lung resection for cancer: impact of chronic obstructive pulmonary disease and time trends. Ann Thorac Surg 2006; 81: pp. 1830-1837.
3. Nagamatsu Y., Shima I., Hayashi A., Yamana H., Shirouzu K., Ishitake T.: Preoperative spirometry versus expired gas analysis during exercise testing as predictors of cardiopulmonary complications after lung resection. Surg Today 2004; 34: pp. 107-110.
4. Ueda K., Kaneda Y., Sudoh M., et. al.: Role of quantitative CT in predicting hypoxemia and complications after lung lobectomy for cancer, with special reference to area of emphysema. Chest 2005; 128: pp. 3500-3506.
5. Ohno Y., Koyama H., Nogami M., et. al.: Postoperative lung function in lung cancer patients: comparative analysis of predictive capability of MRI, CT, and SPECT. AJR Am J Roentgenol 2007; 189: pp. 400-408.
6. Sverzellati N., Chetta A., Calabrò E., et. al.: Reliability of quantitative computed tomography to predict postoperative lung function in patients with chronic obstructive pulmonary disease having a lobectomy. J Comput Assist Tomogr 2005; 29: pp. 819-824.
7. Wu M.T., Pan H.B., Chiang A.A., et. al.: Prediction of postoperative lung function in patients with lung cancer: comparison of quantitative CT with perfusion scintigraphy. AJR Am J Roentgenol 2002; 178: pp. 667-672.
8. Liu F., Han P., Feng G.S., et. al.: Using quantitative CT to predict postoperative pulmonary function in patients with lung cancer. Chin Med J 2005; 118: pp. 742-746.
9. Kishi K., Gurney J.W., Schroeder D.R., Scanlon P.D., Swensen S.J., Jett J.R.: The correlation of emphysema or airway obstruction with the risk of lung cancer: a matched case-controlled study. Eur Respir J 2002; 19: pp. 1093-1098.
10. Madani A., Zanen J., de Maertelaer V., Gevenois P.A.: Pulmonary emphysema: objective quantification at multi-detector row CT—comparison with macroscopic and microscopic morphometry. Radiology 2006; 238: pp. 1036-1043.
11. Kauczor H.U., Heussel C.P., Fischer B., Klamm R., Mildenberger P., Thelen M.: Assessment of lung volumes using helical CT at inspiration and expiration: comparison with pulmonary function tests. AJR Am J Roentgenol 1998; 171: pp. 1091-1095.
12. Stern E.J., Frank M.S.: CT of the lung in patients with pulmonary emphysema: diagnosis, quantification, and correlation with pathologic and physiologic findings. AJR Am J Roentgenol 1994; 162: pp. 791-798.
13. Arakawa A., Yamashita Y., Nakayama Y., et. al.: Assessment of lung volumes in pulmonary emphysema using multidetector helical CT: comparison with pulmonary function tests. Comput Med Imaging Graph 2001; 25: pp. 399-404.
14. Becker M.D., Berkmen Y.M., Austin J.H., et. al.: Lung volumes before and after lung volume reduction surgery: quantitative CT analysis. Am J Respir Crit Care Med 1998; 157: pp. 1593-1599.
15. Park K.J., Bergin C.J., Clausen J.L.: Quantitation of emphysema with three-dimensional CT densitometry: comparison with two-dimensional analysis, visual emphysema scores, and pulmonary function test results. Radiology 1999; 211: pp. 541-547.
16. Shaker S.B., Dirksen A., Laursen L.C., Skovgaard L.T., Holstein-Rathlou N.H.: Volume adjustment of lung density by computed tomography scans in patients with emphysema. Acta Radiol 2004; 45: pp. 417-423.
17. Madani A., De Maertelaer V., Zanen J., Zanen J., Gevenois P.A.: Pulmonary emphysema: radiation dose and section thickness at multidetector CT quantification—comparison with macroscopic and microscopic morphometry. Radiology 2007; 243: pp. 250-257.
18. Camiciottoli G., Bartolucci M., Maluccio N.M., et. al.: Spirometrically gated high- resolution CT findings in COPD: lung attenuation vs lung function and dyspnea severity. Chest 2006; 129: pp. 558-564.
19. Svanberg L.: Influence of posture on the lung volumes, ventilation and circulation in normals; a spirometric-bronchospirometric investigation. Scand J Clin Lab Invest 1957; 9: pp. 1-195.
20. Bobbio A., Chetta A., Ampollini L., et. al.: Preoperative pulmonary rehabilitation in patients undergoing lung resection for non-small cell lung cancer. Eur J Cardiothorac Surg 2008; 33: pp. 95-98.
21. Matsuoka S., Kurihara Y., Yagihashi K., Hoshino M., Watanabe N., Nakajima Y.: Quantitative assessment of air trapping in chronic obstructive pulmonary disease using inspiratory and expiratory volumetric MDCT. AJR Am J Roentgenol 2008; 190: pp. 762-769.
22. Biederer J., Dinkel J., Bolte H., et. al.: Respiratory-gated helical computed tomography of lung: reproducibility of small volumes in an ex vivo model. Int J Radiat Oncol Biol Phys 2007; 69: pp. 1642-1649.
23. Pelinkovic D., Lörcher U., Chow K.U., Kronenberger H., Buhl R.: Spirometric gated quantitative computed tomography of the lung in healthy smokers and nonsmokers. Invest Radiol 1997; 32: pp. 335-343.