
Rationale and Objectives
To investigate 64 computed tomography (CT) perfusion imaging features of patients with pancreatic cancer and mass-forming chronic pancreatitis.
Materials and Methods
Between January 2003 and April 2010, 234 patients with pancreatic mass underwent 64-CT perfusion imaging. Among them, the histopathological results of 64 patients were proven to be pancreatic adenocarcinoma and 15 patients were proven to be mass-forming chronic pancreatitis. Additionally, CT perfusion imaging was performed in 33 healthy volunteers served as controls. The slice data were processed using CT perfusion software. Perfusion parameters including time density curve, blood flow, blood volume, permeability, peak enhancement, and time to peak were recorded.
Results
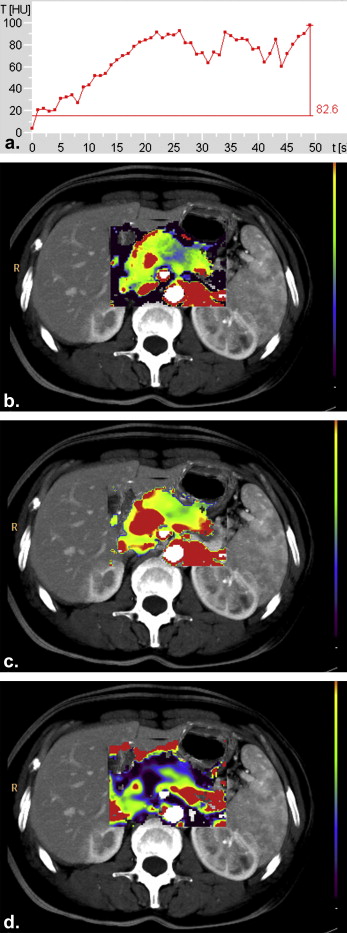
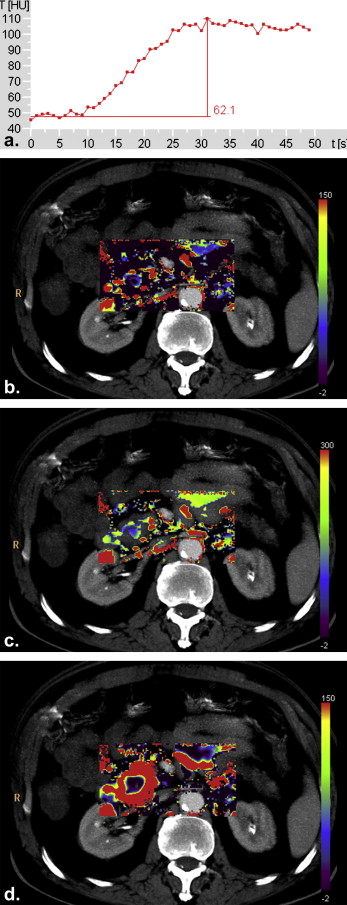
Blood flow was 77% lower in patients with pancreatic adenocarcinoma than in controls, 48% lower in patients with mass-forming chronic pancreatitis than in controls, and 56% lower in patients with pancreatic adenocarcinoma than with mass-forming chronic pancreatitis ( P < .016). Blood volume was 65% lower in pancreatic adenocarcinoma than in controls, 27% lower in mass-forming chronic pancreatitis than in controls, and 53% lower in cancer than mass-forming chronic pancreatitis ( P < .016). Permeability was 559% higher in pancreatic adenocarcinoma than in controls, 821% higher in mass-forming chronic pancreatitis than in controls, and 28% lower in cancer than mass-forming chronic pancreatitis ( P < .016). Peak enhancement was 27% lower and time to peak 23% longer in pancreatic adenocarcinoma than mass-forming chronic pancreatitis ( P < .016). Time-density curve showed the peak of mass-forming chronic pancreatitis is earlier and higher than that of pancreatic adenocarcinoma, and the peak of mass-forming chronic pancreatitis is later and lower than that of controls.
Conclusion
CT perfusion imaging can provide additional quantitative hemodynamic information of pancreatic adenocarcinoma and mass-forming chronic pancreatitis.
Pancreatic cancer, the fourth highest cause of cancer-related death, remains an incurable and rapidly lethal disease, with a 5-year survival rate of less than 3% . Radical surgery is only possible in 20% of patients . The majority of the patients are already in the later stage of disease at the time of diagnosis and half of them do not survive more than 1 year . For those who undergo surgical bypass with unresectable cancer or occult metastasis, surgical mortality rate is 16% with no survival advantage . This poor survival rate and bad prognosis are associated with the diagnosis in advanced stage, which precludes the only potential curative treatment: surgical resection. In this setting, the main objective in the management of pancreatic cancer is to perform an early diagnosis and so new insights into the early diagnosis of this lethal disease are urgently needed . Discrimination between pancreatic adenocarcinoma and mass-forming chronic pancreatitis in the early stage is usually a clinical issue. Data are limited on identification of a role for the perfusion imaging in the differential diagnosis of pancreatic cancer and mass-forming chronic pancreatitis which may hold promise for new diagnostic approaches.
Perfusion computed tomography (CT) is a topic of current interest. CT perfusion imaging allows functional information to be obtained by reflecting the hemodynamic changes of tissues in addition to anatomical detail and has enabled measurement of tissue blood perfusion and capillary permeability of the brain, kidney, heart, liver, spleen, and pancreas . Miles for the first time measured the perfusion parameters of normal pancreas in 1995 . Although small sample exploratory studies about CT perfusion imaging in normal tissue of pancreas, pancreatic cancer, and pancreatic endocrine tumors were conducted after that, its role in discriminating pancreatic cancer from mass-forming chronic pancreatitis has not been well defined . CT perfusion imaging allows noninvasive absolute quantification of pancreatic perfusion and may intensify the precision of the differential diagnosis of pancreatic cancer and mass-forming chronic pancreatitis .
Get Radiology Tree app to read full this article<
Materials and methods
Research Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Perfusion Procedure
Get Radiology Tree app to read full this article<
Data Processing
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Perfusion CT Parameters of Pancreatic Adenocarcinoma
Get Radiology Tree app to read full this article<
Table 1
The Comparisons of Perfusion Parameters in Patients with Pancreatic Adenocarcinoma, Patients with Mass-forming Chronic Pancreatitis and Normal Subjects (Mean ± Standard Deviation)
Pancreatic Adenocarcinoma
( n = 64) Mass-forming Chronic Pancreatitis
( n = 15) Controls
( n = 33) Blood flow (mL/min/mL) 0.365 ± 0.204 ∗ 0.820 ± 0.345 ∗† 1.567 ± 0.379 Blood volume (mL/mL) 0.089 ± 0.042 ∗ 0.191 ± 0.088 ∗† 0.258 ± 0.041 Permeability (mL/mL/min) 0.956 ± 0.556 ∗ 1.336 ± 0.582 ∗† 0.145 ± 0.088 Peak enhancement (HU) 30.858 ± 15.860 ∗ 42.166 ± 23.109 ∗† 57.000 ± 13.382 Time to peak (seconds) 47.047 ± 6.124 ∗ 36.133 ± 7.726 ∗† 24.858 ± 2.881
P < .016 versus normal controls () or versus pancreatic cancer (†).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Perfusion CT Parameters of Mass-forming Chronic Pancreatitis
Get Radiology Tree app to read full this article<
Comparison of Perfusion Parameters between Pancreatic Adenocarcinoma and Mass-forming Chronic Pancreatitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Pancreatic Perfusion CT Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diagnostic Imaging of Pancreatic Carcinoma and Mass-forming Chronic Pancreatitis
Get Radiology Tree app to read full this article<
Perfusion CT Characteristics of Pancreatic Adenocarcinoma and Mass-forming Chronic Pancreatitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Thayer S.P., di Magliano M.P., Heiser P.W., et. al.: Hedgehog is an early and late mediator of pancreatic cancer tumorigenesis. Nature 2003; 425: pp. 851-856.
2. Smith S.L., Rajan P.S.: Imaging of pancreatic adenocarcinoma with emphasis on multidetector CT. Clin Radiol 2004; 59: pp. 26-38.
3. de Castro S.M., Biere S.S., Lagarde S.M., et. al.: Validation of a nomogram for predicting survival after resection for adenocarcinoma of the pancreas. Br J Surg 2009; 96: pp. 417-423.
4. Müller M.W., Friess H., Köninger J., et. al.: Factors influencing survival after bypass procedures in patients with advanced pancreatic adenocarcinomas. Am J Surg 2008; 195: pp. 221-228.
5. Jones S., Zhang X., Parsons D.W., et. al.: Core signaling pathways in human pancreatic cancers revealed by global genomic analyses. Science 2008; 321: pp. 1801-1806.
6. Ovali G.Y., Sakar A., Göktan C., et. al.: Thorax perfusion CT in non-small cell lung cancer. Comput Medi Imag Graph 2007; 31: pp. 686-691.
7. Miles K.A., Hayball M.P., Dixon A.K.: Measurement of human pancreatic perfusion using dynamic computed tomography with perfusion imaging. Br J Radiol 1995; 809: pp. 471-475.
8. Klotz E., König M.: Perfusion measurements of the brain: using dynamic CT for the quantitative assessment of cerebral ischemia in acute stroke. Eur J Radiol 1999; 30: pp. 170-184.
9. van Beek E.J., Hoffman E.A.: Functional imaging: CT and MRI. Clin Chest Med 2008; 29: pp. 195-216.
10. Miles K.A., Hayball M., Dixon A.K.: Colour perfusion imaging a new application of computed tomography. Lancet 1991; 337: pp. 643-645.
11. Badea C.T., Johnston S.M., Subashi E., et. al.: Lung perfusion imaging in small animals using 4D micro-CT at heartbeat temporal resolution. Med Phys 2010; 37: pp. 54-62.
12. Nett B.E., Brauweiler R., Kalender W., et. al.: Perfusion measurements by micro-CT using prior image constrained compressed sensing (PICCS): initial phantom results. Phys Med Biol 2010; 55: pp. 2333-2350.
13. Sahani D.V., Holalkere N.S., Mueller P.R., et. al.: Advanced hepatocellular carcinoma: CT perfusion of liver and tumor tissue-initial experience. Radiology 2007; 243: pp. 736-743.
14. Burns J.D., Jacob J.T., Luetmer P.H., et. al.: CT perfusion evidence of early global cerebral hypoperfusion after aneurysmal subarachnoid hemorrhage with cardiac arrest. Neurocrit Care 2010; 12: pp. 261-264.
15. Gelfand J.M., Wintermark M., Josephson S.A.: Cerebral perfusion-CT patterns following seizure. Eur J Neurol 2010; 17: pp. 594-601.
16. Kambadakone A.R., Sahani D.V.: Body perfusion CT: technique, clinical applications, and advances. Radiol Clin North Am 2009; 47: pp. 161-178.
17. Dawson P.: Functional imaging in CT. Eur J Radiol 2006; 60: pp. 331-333.
18. Rodríguez-Granillo G.A., Rosales M.A., Degrossi E., et. al.: Signal density of left ventricular myocardial segments and impact of beam hardening artifact: implications for myocardial perfusion assessment by multidetector CT coronary angiography. Int J Cardiovasc Imaging 2010; 26: pp. 345-354.
19. Bybee K.A., Lee J., Markiewicz R., et. al.: Diagnostic and clinical benefit of combined coronary calcium and perfusion assessment in patients undergoing PET/CT myocardial perfusion stress imaging. J Nucl Cardiol 2010; 17: pp. 188-196.
20. Celler A., Shcherbinin S., Hughes T.: An investigation of potential sources of artifacts in SPECT-CT myocardial perfusion studies. J Nucl Cardiol 2010; 17: pp. 232-246.
21. Kandel S., Kloeters C., Meyer H., et. al.: Whole-organ perfusion of the pancreas using dynamic volume CT in patients with primary pancreas carcinoma: acquisition technique, post-processing and initial results. Eur Radiol 2009; 19: pp. 2641-2646.
22. Wittkamp G., Buerke B., Dziewas R., et. al.: Whole brain perfused blood volume CT: visualization of infarcted tissue compared to quantitative perfusion CT. Acad Radiol 2010; 17: pp. 427-432.
23. Miles K.A., Hayball M.P., Dixon A.K.: Functional images of changes in human intrarenal perfusion using quantitative dynamic computed tomography. Invest Radiol 1994; 29: pp. 911-914.
24. Miles K.A.: Perfusion CT for the assessment of tumour vascularity: which protocol. Br J Radiol 2003; 76: pp. 36-42.
25. Blomley M.J., McBride A., Mohammedtagi S., et. al.: Functional renal perfusion imaging with colour mapping: is it a useful adjunct to spiral CT of in the assessment of abdominal aortic aneurysm (AAA)?. Eur J Radiol 1999; 30: pp. 214-220.
26. Miles K.A., Charnsangavej C., Lee F.T., et. al.: Application of CT in the investigation of angiogenesis in oncology. Acad Radiol 2000; 7: pp. 840-850.
27. Cuenod C.A., Fournier L., Balvay D., et. al.: Tumor angiogenesis: pathophysiology and implications for contrast-enhanced MRI and CT assessment. Abdom Imaging 2006; 31: pp. 188-193.
28. Yamada T.: Textbook of Gastroenterology.4th ed.2003.Lippincott Williams & Wikins, IncPhiladelphia
29. Bali M.A., Metens T., Denolin V., et. al.: Pancreatic perfusion: noninvasive quantitative assessment with dynamic contrast-enhanced MR imaging without and with secretin stimulation in healthy volunteers — initial results. Radiology 2008; 247: pp. 115-121.
30. Ellika S.K., Jain R., Patel S.C., et. al.: Role of perfusion CT in glioma grading and comparison with conventional MR imaging features. AJNR Am J Neuroradiol 2007; 28: pp. 1981-1987.
31. Kim J.K., Altun E., Elias J., et. al.: Focal pancreatic mass: distinction of pancreatic cancer from chronic pancreatitis using gadolinium-enhanced 3D-gradient-echo MRI. J Magn Reson Imaging 2007; 26: pp. 313-322.
32. Miles K.A., Griffiths M.R.: Perfusion CT: A worthwhile enhancement. Br J Radiol 2003; 76: pp. 220-231.
33. Iglesias García J., Lariño Noia J., Domínguez Muñoz J.E.: Endoscopic ultrasound in the diagnosis and staging of pancreatic cancer. Rev Esp Enferm Dig 2009; 101: pp. 631-638.
34. Al-Haddad M., Eloubeidi M.A.: Interventional EUS for the diagnosis and treatment of locally advanced pancreatic cancer. JOP 2010; 11: pp. 1-7.
35. Olive K.P., Jacobetz M.A., Davidson C.J., et. al.: Inhibition of hedgehog signaling enhances delivery of chemotherapy in a mouse model of pancreatic cancer. Science 2009; 324: pp. 1457-1461.
36. Xu J., Liang Z., Hao S., et. al.: Pancreatic adenocarcinoma: dynamic 64-slice helical CT with perfusion imaging. Abdom Imaging 2009; 34: pp. 759-766.
37. Eastwood J.D., Lev M.H., Provenzale J.M.: Perfusion CT with iodinated contrast material. AJR Am J Roentgenol 2003; 180: pp. 3-12.
38. Cáceres A.V., Zwingenberger A.L., Hardam E., et. al.: Helical computed tomographic angiography of the normal canine pancreas. Vet Radiol Ultrasound 2006; 47: pp. 270-278.
39. Tsuji Y., Yamamoto H., Yazumi S., et. al.: Perfusion computerized tomography can predict pancreatic necrosis in early stages of severe acute pancreatitis. Clin Gastroenterol Hepatol 2007; 5: pp. 1484-1492.
40. Takeda K., Mikami Y., Fukuyama S., et. al.: Pancreatic ischemia associated with vasospasm in the early phase of human acute necrotizing pancreatitis. Pancreas 2005; 30: pp. 40-49.
41. Mirecka J., Libura J., Libura M., et. al.: Morphological parameters of the angiogenic response in pancreatic ductal adenocarcinoma—correlation with histological grading and clinical data. Folia Histochem Cytobiol 2001; 39: pp. 335-340.
42. Bluemke D.A., Cameron J.L., Hruban R.H., et. al.: Potentionally resectable pancreatic adenocarcinoma: spiral CT assessment with surgical and pathologic correlation. Radiology 1995; 197: pp. 381-385.
43. Chang W.I., Kim B.J., Lee J.K., et. al.: The clinical and radiological characteristics of focal mass-forming autoimmune pancreatitis comparison with chronic pancreatitis and pancreatic cancer. Pancreas 2009; 38: pp. 401-408.
44. von Dobschuetz E., Pahernik S., Hoffmann T., et. al.: Dynamic intravital fluorescence microscopy—a novel method for the assessment of microvascular permeability in acute pancreatitis. Microvasc Res 2004; 67: pp. 55-63.
45. Miles K.A.: Tumour angiogenesis and its relation to contrast enhancement on computed tomography: a review. Eur J Radiol 1999; 30: pp. 198-205.
46. Galanski M., Nagel H.D., Stamm G.: Results of a federation inquiry 2005/2006: pediatric CT X-ray practice in Germany. Rofo 2007; 179: pp. 1110-1111.
47. Siegel M.J., Schmidt , Bradley D., et. al.: Radiation dose and image quality in pediatric CT: Effect of technical factors and phantom size and shape. Radiology 2004; 233: pp. 515-522.
48. Kapanen M., Halavaara J., Häkkinen A.M.: Comparison of liver perfusion parameters studied with conventional extravascular and experimental intravascular CT contrast agents. Acad Radiol 2007; 14: pp. 951-958.
49. Kämena A., Streitparth F., Grieser C., et. al.: Dynamic perfusion CT Optimizing the temporal resolution for the calculation of perfusion CT parameters in stroke patients. Eur J Radiol 2007; 64: pp. 111-118.
50. Schramm P., Huang Y., Erb G., et. al.: How does the injection protocol influence the attenuation-time curve in CT perfusion measurements: comparison of measured and simulated data. Med Phys 2009; 36: pp. 3487-3494.
51. Kim S.M., Cho Y.B., Haider M.A., et. al.: Multiphasic contrast injection for improved precision of parameter estimates in functional CT. Med Phys 2008; 35: pp. 5921-5933.
52. Nye J.A., Hamill J., Tudorascu D., et. al.: Comparison of low-pitch and respiratory-averaged CT protocols for attenuation correction of cardiac PET studies. Med Phys 2009; 36: pp. 1618-1623.