
Rationale and Objectives
To evaluate the ex vivo ablation zones created in hepatic tissue using monopolar and bipolar gas- and water-cooled radiofrequency (RF) applicators.
Materials and Methods
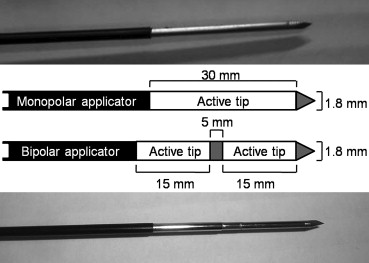
RF ablations were performed on ex vivo bovine liver tissue using closed circuit water-cooled and closed circuit cryogenically cooled (via CO 2 enthalpy) 15-ga linear-needle applicators. Both monopolar and bipolar electrode applicators were used, with the electric current administered ranging in 50-mA increments from 1100 to 1300 mA for the monopolar case, and from 500 to 700 mA for the bipolar case. Total ablation time was 15 minutes. Six tissue samples were ablated per setting. The ablated volumes were assumed to have a three-dimensional ellipsoid shape, with one long major axis and two smaller minor axes. Gross histology was used to measure the dimensions of the ablated regions to quantify the ablated volume, the dimensions of the axis, and the ratio between the long axis and the smallest minor axis, which was termed the ellipticity index.
Results
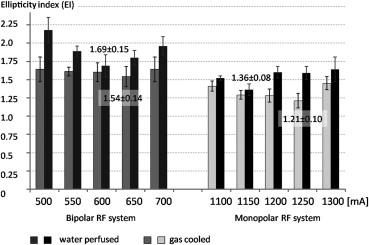
The gas-cooled monopolar applicator achieved the largest short-axis ablation diameter (4.05 ± 0.4 cm), followed by the water-cooled monopolar applicator (3.18 ± 0.29 cm). With the bipolar applicator, the gas-cooled applicators also achieved larger short-axis ablation diameters (3.02 ± 0.15 cm) than the water-cooled applicators (2.72 ± 0.29 cm). The gas-cooled monopolar applicator also provided the largest ablation volume (42.7 ± 10.7 mL) and the most spherically shaped lesions (ellipticity index: 1.21 ± 0.10). Lesion size increased with injected current up to a threshold current of 1200/1250 mA (monopolar water-/gas-cooled) and 600/650 mA (bipolar water-/gas-cooled), but dropped at greater values.
Conclusions
Gas-cooled monopolar applicators were superior to the other tested applicators in terms of both volume and sphericity of the ablation zone.
Because the goal of achieving large and reliable ablation of lesions has not been completely achieved, new ablation methods continue to be developed. We can assume that a typical lesion created by a linear ablation probe can be modeled as a three-dimensional spheroid, which has one major and two minor axes, with the major axis lying parallel to the probe shaft. Currently, the extent of the lesion’s long axis can be controlled by choosing between different lengths of electrodes, but controlling the short axis remains an issue that limits the success of ablation therapy, especially in the case of larger lesions. Indeed, studies have shown that local tumor recurrence is more frequently observed in lesions >3 cm which have been ablated . In radiofrequency (RF) ablation, an increase in the ablation volume can be accomplished through several methods: by increasing the electrode surface, which is achieved by increasing the probe gauge , by using several applicators in a cluster , by using a multiprobe array , or by using expandable applicators . Increasing the power output can also increase the ablated volume; this can be combined with strategies for reducing probe heating, such as pulsing the energy application . Another method is to influence the energy application at the interface between the applicator and the tissue by preventing tissue dehydration and carbonization using actively cooled applicators that use closed circuit water cooling , perfusion , or cryogenic cooling .
RF ablation can be delivered using monopolar or bipolar applicators. In a monopolar setting, part of the applied energy is lost between the electrodes and may lead to heating of metallic materials, such as pacemaker electrodes and surgical clips . In addition, skin burns may appear if the grounding pads are partially detached . Bipolar applicators do not require grounding pads and have been reported to be more energy efficient .
Get Radiology Tree app to read full this article<
Materials and methods
RF System
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Experimental Setup and Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ablation Assessment
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<

Table 1
Ablation Zone Characteristics
Cooling (mA) Water-perfused Gas-cooled Short Axis (mm) Long Axis (mm) Ellipticity Index Ablation Duration (seconds) Regularity Index (TDmin/TDmax) Short Axis (mm) Long Axis (mm) Ellipticity Index Ablation Duration (seconds) Regularity Index (TDmin/TDmax) Bipolar radiofrequency system 500 19 ± 1 42 ± 1 2.18 900 ± 0 0.88 ± 0.07 17 ± 1 28 ± 2 1.64 900 ± 0 0.88 ± 0.05 550 21 ± 1 40 ± 1 1.89 880 ± 49 0.94 ± 0.04 22 ± 2 35 ± 3 1.61 883 ± 41 0.96 ± 0.05 600 27 ± 3 46 ± 2 1.69 872 ± 35 0.94 ± 0.13 27 ± 3 43 ± 2 1.60 847 ± 87 0.93 ± 0.06 650 25 ± 1 44 ± 1 1.80 795 ± 120 0.96 ± 0.33 30 ± 2 43 ± 1 1.54 825 ± 63 0.94 ± 0.04 700 22 ± 1 42 ± 2 1.96 540 ± 187 0.89 ± 0.08 28 ± 3 46 ± 2 1.64 655 ± 194 0.99 ± 0.11 Monopolar radiofrequency system 1100 29 ± 1 44 ± 1 1.52 692 ± 163 0.93 ± 0.03 30 ± 2 43 ± 2 1.41 757 ± 196 0.91 ± 0.04 1150 31 ± 3 41 ± 2 1.36 482 ± 61 0.94 ± 0.04 34 ± 1 44 ± 2 1.29 900 ± 0 0.92 ± 0.06 1200 32 ± 3 51 ± 4 1.60 610 ± 148 0.95 ± 0.04 39 ± 5 49 ± 4 1.28 745 ± 180 0.93 ± 0.06 1250 27 ± 2 43 ± 3 1.59 425 ± 142 0.95 ± 0.03 41 ± 5 49 ± 2 1.21 900 ± 0 0.93 ± 0.03 1300 27 ± 2 43 ± 3 1.64 375 ± 92 0.95 ± 0.04 33 ± 5 47 ± 5 1.45 522 ± 276 0.93 ± 0.04
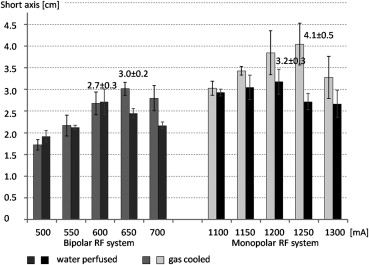
Table 2
Mann–Whitney U Test: Levels of Significance
Short-axis Diameters ( P Value) Ellipticity Index ( P Value) Volume ( P Value) Monopolar gas-cooled versus monopolar water-cooled.002.015.030 Monopolar gas-cooled versus bipolar gas-cooled.002.002.002 Monopolar gas-cooled versus bipolar water-perfused.002.002.002 Monopolar water-perfused versus bipolar water-perfused.026.009.041 Monopolar water-perfused versus bipolar gas-cooled .345.041 .064 Bipolar gas-cooled versus bipolar water-perfused.034 .132 .064
P-Level < .05 in bold.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Solbiati L., Livraghi T., Goldberg S.N., et. al.: Percutaneous radio-frequency ablation of hepatic metastases from colorectal cancer: long-term results in 117 patients. Radiology 2001; 221: pp. 159-166.
2. van Duijnhoven F.H., Jansen M.C., Junggeburt J.M., et. al.: Factors influencing the local failure rate of radiofrequency ablation of colorectal liver metastases. Ann Surg Oncol 2006; 13: pp. 651-658.
3. Berber E., Siperstein A.: Local recurrence after laparoscopic radiofrequency ablation of liver tumors: an analysis of 1032 tumors. Ann Surg Oncol 2008; 15: pp. 2757-2764.
4. Goldberg S.N., Gazelle G.S., Dawson S.L., et. al.: Tissue ablation with radiofrequency: effect of probe size, gauge, duration, and temperature on lesion volume. Acad Radiol 1995; 2: pp. 399-404.
5. Goldberg S.N., Solbiati L., Hahn P.F., et. al.: Large-volume tissue ablation with radio frequency by using a clustered, internally cooled electrode technique: laboratory and clinical experience in liver metastases. Radiology 1998; 209: pp. 371-379.
6. Goldberg S.N., Gazelle G.S., Dawson S.L., et. al.: Tissue ablation with radiofrequency using multiprobe arrays. Acad Radiol 1995; 2: pp. 670-674.
7. de Baere T., Denys A., Wood B.J., et. al.: Radiofrequency liver ablation: experimental comparative study of water-cooled versus expandable systems. AJR Am J Roentgenol 2001; 176: pp. 187-192.
8. Goldberg S.N., Stein M.C., Gazelle G.S., et. al.: Percutaneous radiofrequency tissue ablation: optimization of pulsed-radiofrequency technique to increase coagulation necrosis. J Vasc Interv Radiol 1999; 10: pp. 907-916.
9. Solazzo S.A., Ahmed M., Liu Z., et. al.: High-power generator for radiofrequency ablation: larger electrodes and pulsing algorithms in bovine ex vivo and porcine in vivo settings. Radiology 2007; 242: pp. 743-750.
10. Lorentzen T.: A cooled needle electrode for radiofrequency tissue ablation: thermodynamic aspects of improved performance compared with conventional needle design. Acad Radiol 1996; 3: pp. 556-563.
11. Mulier S., Ni Y., Frich L., et. al.: Experimental and clinical radiofrequency ablation: proposal for standardized description of coagulation size and geometry. Ann Surg Oncol 2007; 14: pp. 1381-1396.
12. Pereira P.L., Trubenbach J., Schenk M., et. al.: Radiofrequency ablation: in vivo comparison of four commercially available devices in pig livers. Radiology 2004; 232: pp. 482-490.
13. Hines-Peralta A., Hollander C.Y., Solazzo S., et. al.: Hybrid radiofrequency and cryoablation device: preliminary results in an animal model. J Vasc Interv Radiol 2004; 15: pp. 1111-1120.
14. Rempp H., Voigtlander M., Clasen S., et. al.: Increased ablation zones using a cryo-based internally cooled bipolar RF applicator in ex vivo bovine liver. Invest Radiol 2009; 44: pp. 763-768.
15. Carrara S., Arcidiacono P.G., Albarello L., et. al.: Endoscopic ultrasound-guided application of a new internally gas-cooled radiofrequency ablation probe in the liver and spleen of an animal model: a preliminary study. Endoscopy 2008; 40: pp. 759-763.
16. Tong N.Y., Ru H.J., Ling H.Y., et. al.: Extracardiac radiofrequency ablation interferes with pacemaker function but does not damage the device. Anaesthesiology 2004; 100: pp. 1041.
17. Goldberg S.N., Solbiati L., Halpern E.F., et. al.: Variables affecting proper system grounding for radiofrequency ablation in an animal model. J Vasc Interv Radiol 2000; 11: pp. 1069-1075.
18. McGahan J.P., Gu W.Z., Brock J.M., et. al.: Hepatic ablation using bipolar radiofrequency electrocautery. Acad Radiol 1996; 3: pp. 418-422.
19. Lee J.M., Han J.K., Kim S.H., et. al.: A comparative experimental study of the in-vitro efficiency of hypertonic saline-enhanced hepatic bipolar and monopolar radiofrequency ablation. Korean J Radiol 2003; 3: pp. 163-169.
20. Haemmerich D., Staelin S.T., Tungjitkusolmun S., et. al.: Hepatic bipolar radio-frequency ablation between separated multiprong electrodes. IEEE Trans Biomed Eng 2001; 48: pp. 1145-1152.
21. Goldberg S.N., Grassi C.J., Cardella J.F., et. al.: Image-guided tumor ablation: standardization of terminology and reporting criteria. J Vasc Interv Radiol 2009; 20: pp. S377-S390.
22. Lee J.M., Han J.K., Kim S.H., et. al.: Bipolar radiofrequency ablation using wet-cooled electrodes: an in vitro experimental study in bovine liver. AJR Am J Roentgenol 2005; 184: pp. 391-397.
23. Rempp H., Scharpf M., Voigtlander M., et. al.: Sustained growth of the ex vivo ablation zones’ critical short axis using gas-cooled radiofrequency applicators. Cardiovasc Intervent Radiol 2011; 34: pp. 149-155.
24. Lee J.M., Han J.K., Kim S.H., et. al.: Saline-enhanced hepatic radiofrequency ablation using a perfused-cooled electrode: comparison of dual probe bipolar mode with monopolar and single probe bipolar modes. Korean J Radiol 2004; 5: pp. 121-127.
25. Lee J.M., Han J.K., Kim S.H., et. al.: An ex-vivo experimental study on optimization of bipolar radiofrequency liver ablation using perfusion-cooled electrodes. Acta Radiol 2005; 46: pp. 443-451.
26. Lee J.M., Han J.K., Kim S.H., et. al.: Hepatic bipolar radiofrequency ablation using perfused-cooled electrodes: a comparative study in the ex vivo bovine liver. Br J Radiol 2004; 77: pp. 944-949.
27. Lee J.M., Kim S.H., Han J.K., et. al.: Ex vivo experiment of saline-enhanced hepatic bipolar radiofrequency ablation with a perfused needle electrode: comparison with conventional monopolar and simultaneous monopolar modes. Cardiovasc Intervent Radiol 2005; 28: pp. 338-345.
28. Clasen S., Schmidt D., Dietz K., et. al.: Bipolar radiofrequency ablation using internally cooled electrodes in ex vivo bovine liver: prediction of coagulation volume from applied energy. Invest Radiol 2007; 42: pp. 29-36.
29. Goldberg S.N., Hahn P.F., Tanabe K.K., et. al.: Percutaneous radiofrequency tissue ablation: does perfusion-mediated tissue cooling limit coagulation necrosis?. J Vasc Interv Radiol 1998; 9: pp. 101-111.
30. Bitsch R.G., Dux M., Helmberger T., et. al.: Effects of vascular perfusion on coagulation size in radiofrequency ablation of ex vivo perfused bovine livers. Invest Radiol 2006; 41: pp. 422-427.
31. Yu J., Liang P., Yu X., et. al.: A comparison of microwave ablation and bipolar radiofrequency ablation both with an internally cooled probe: results in ex vivo and in vivo porcine livers. Eur J Radiol 2011; 79: pp. 124-130.