
Rationale and Objectives
The start of call is a stressful time for radiology residents. Traditional teaching methods are not ideal for call preparation because they are radically different than the task performed on call. The purpose of this study is to determine if a computer-based radiology simulator would have an effect on resident confidence level or diagnostic abilities.
Materials and Methods
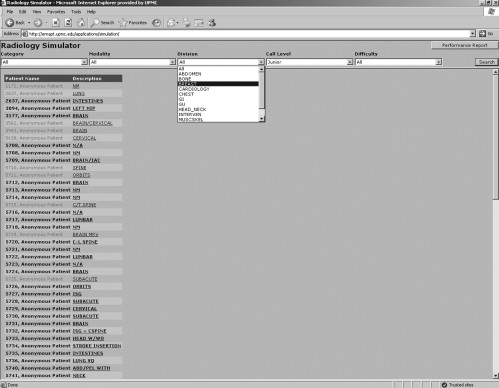
A simulator was created to mimic the picture archive and communication system (PACS) at our hospital. Typical call-level cases were selected, anonymized, and entered into the database. The first-year residents were randomly split into a control group and a study group that used the simulator. Each resident took a survey 1 month before and after beginning call to measure his or her subjective feeling of preparedness and nervousness. Objective measures were also obtained through the use of discordance levels from on-call cases.
Results
Seventy-one cases were entered into the simulator. Of the 12 residents in the first-year class, 7 were placed in the study group and 5 in the control group. The residents in both groups claimed they felt more prepared and less nervous 1 month after starting call. The differences at survey were not significant, but the residents in the study group trended toward feeling more prepared and less nervous. There was no statistical difference in the discordance rates for on-call cases between the two groups.
Conclusions
Although statistical significance was not reached between the users of the radiology simulator and the control group, there was a subjective feeling that the simulator was useful for call preparation and as an interactive learning tool. A larger sample study group size may show statistical significance.
The onset of call is a scary milestone for most new radiologists. Residency programs use a variety of methods to help prepare their residents for this task, including lectures, specific core rotations, mini-call, case conferences, and reviews of teaching files. While each method helps prepare the resident for specific topics that may arise on call, none simulates the actual activity of call: reading cases independently. To address this deficiency, an on-call simulator was created.
Simulators have a long history of use in both medicine and aviation for education and training purposes; however, most simulators teach a particular skill or skill set. Medical simulators have been used most extensively in surgery and anesthesiology, but they are also used in other fields such as ophthalmology and gastroenterology ( ). Simulators in radiology have recently been developed for perfecting ultrasound and vascular interventional technique ( ). Previously, other simulator programs have been described, but on a limited scale ( ). Because much of modern radiology is performed digitally, radiology is uniquely situated within medicine for the seamless integration of simulators.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Simulator
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case Manager
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Case Selection
Get Radiology Tree app to read full this article<
Table 1
A List of Cases and Their Attributes Entered in the Simulator
Patient Number Pertinent Information Modality Primary Finding(s) 1 Liver transplant, shortness of breath, evaluate for pulmonary embolism Chest CT Hydropneumothorax, no pulmonary embolism 2 Abdominal pain A/P CT Acute cholecystitis 3 Small bowel and liver transplant, history of fungal infection, shortness of breath Chest CT Pericardial effusion with pericardial tamponade 4 Not breathing well Chest CR Large pneumothorax 5 Trauma–motor vehicle accident with rollover C/A/P CT Diaphragmatic rupture, pelvic fractures with active arterial extravesation, splenic laceration, pneumothorax, lung contusion 6 Head Trauma Head CT Axonal shear injury 7 Hit by car Head CT Subdural hemorrhage with midline shift and uncal herniation, subarachnoid hemorrhage, intraparenchymal hemorrhage, and multiple fractures 8 Left upper lobe mass, fever, HIV positive Chest CT Cavitary lung lesion with associated mediastinal and hilar lymphadenopathy 9 Left flank pain, history of left ureteral surgery A/P CT Midureteral obstructing stone causing hydronephrosis and hydroureter 10 Status post liver transplant. Evaluate for biliary obstruction Liver US Pneumobilia, low hepatic arterial resistive indices 11 Status post liver transplant. Check vessel patency Liver US Hepatic arterial stenosis and biliary necrosis 12 Abdominal pain A/P CT Epiploic appendagitis 13 Assaulted Orbital CT Blowout fracture of orbit with herniation of fat and the inferior rectus muscle through the fracture defect 14 Right lower extremity swelling. Evaluate for deep vein thrombosis. Lower extremity US Deep vein thrombosis in right lower extremity 15 Partial small bowel obstruction A/P CT Ischemic colitis with pneumatosis intestinalis and portal venous gas 16 Headache Head CT Subarachnoid hemorrhage 17 Fall, evaluate for bleed Head CT fracture of the anterior ring of C1 18 Weakness, evaluate for stroke Head CT Acute right middle cerebral artery infarct with dense MCA sign, loss of gray/white differentiation, and occlusion of the artery on CTA. 19 All-terrain vehicle accident/trauma A/P CT Splenic laceration with active extravesation, large pneumothorax, ruptured renal cyst 20 Stroke Head CT Large left middle cerebral artery infarct causing significant edema and uncal herniation 21 Scrotal pain × 2–3 days Scrotal US Chronic testicular torsion 22 Hit by bus Head CT Epidural hematoma 23 Patient wrestling around and hit abdomen into sink, hematuria A/P CT Renal laceration with extravesation of urine on the delayed images 24 Liver transplant, assess vessel patency Liver US Portal vein thrombosis 25 Chest pain C/A/P CT Type A aortic dissection involving the great vessels, aortic bifurcation, celiac axis, superior mesenteric artery, and the left renal artery; lack of perfusion of the left kidney 26 Fell 25 feet from a barn A/P CT Liver laceration, adrenal hematoma, rib fractures 27 Hit by car Chest CR Widened mediastinum 28 Hit by car Chest CT Aortic transection with mediastinal hematoma, scapular fracture 29 Abdominal pain, vomiting, β-HCG positive Pelvic US Viable intrauterine pregnancy 30 Evaluate for bleed. Patient with hypoxia. Decreased blood pressure. Head CT Small acute subdural hematoma 31 Rule out ischemic bowel A/P CT Pancolitis with bowel hemorrhage 32 Abdominal pain in a patient with a liver transplant and a previous history of endovascular repair of an abdominal aortic aneurysm A/P CT Sigmoid diverticulitis 33 Trauma, motor vehicle accident Pelvic CR Extraperitoneal bladder rupture, pelvic hematoma 34 Trauma, motor vehicle accident A/P CT Liver laceration, renal laceration, sternal fracture, trace pneumothoraces. 35 Right flank pain A/P CT Acute appendicitis 36 Waterskiing accident A/P CT Diastasis of pubic symphysis 37 Trauma Pelvis CR Intertrochanteric fracture 38 Nausea / vomiting / abdominal pain A/P CT Mucinous ovarian tumor 39 Shortness of breath Chest CT Pulmonary embolism 40 Trauma, pregnancy Pelvic US Viable intrauterine pregnancy 41 Sudden onset of abdominal pain. Pregnancy test negative. Pelvic US Ruptured ovarian cyst with hemoperitoneum 42 Stroke Head CT Basilar artery occlusion with hyperdense basilar tip 43 PICC line placement Chest CR PICC in left axilla 44 Feeding tube placement Chest CR Feeding tube in right lower lobe bronchus 45 Status post recent vascular surgery (femoral popliteal bypass and carotid endarterectomy). Now with falling hematocrit and suspected bleed. C/A/P CT Retroperitoneal hemorrhage related to anticoagulation, pneumatosis intestinalis, pneumothorax 46 Left lower quadrant pain, fever A/P CT Pyelonephritis, adrenal adenoma 47 Shortness of breath Chest CR Westemark’s sign of pulmonary embolism 48 Abdominal pain, vomiting A/P CT Pancreatic pseudocyst with splenic artery pseudoaneurysm, thrombosed splenic vein, thrombosed superior mesenteric vein, thrombosed portal vein, liver hemangioma, liver focal nodular hyperplasia 49 Mental status change Head CT Early stroke with loss of differentiation of caudate and internal capsule 50 2–3 day history of right neck swelling without fever or elevated white blood cell count Neck CT Airway compromise due to soft tissue swelling of hypopharynx, cervical adenopathy 51 Intubation Chest CR Right upper lobe collapse due to intubation obstructing a tracheal bronchus 52 Fall 4 days prior, seizure 1 day prior Head CT Intraparenchymal hemorrhage 53 Infiltrate Chest CR Hilar mass with associated collapse of right lower lobe 54 Falling hematocrit and hemoglobin levels A/P CT Iliopsoas hematoma 55 Fall, neck pain Cervical CT Dens fracture with associated epidural hematoma 56 Right upper quadrant pain, positive sonographic Murphy’s sign RUQ US Acute cholecystitis 57 Evaluate for aspiration pneumonia Chest CT Pulmonary embolism with infarcts 58 Abdominal pain, nausea, vomiting A/P CT Crohn disease 59 Cough Chest CR Lingular pneumonia 60 Stab to the chest Chest CR Tension pneumothorax 61 Trauma Cervical CR C2 fracture 62 Ethanol abuse. Elevated amylase and lipase A/P CT Acute on chronic pancreatitis with pancreatic necrosis 63 Trauma Chest CR Right main-stem bronchus intubation with atelectasis of left lung 64 Fall from tree down hillside Pelvic CR Prostatic urethral rupture, diastasis of pubic symphysis 65 Acute cervical motion tenderness A/P CT Tuboovarian abscess, Fitzhugh-Curtis syndrome 66 Trauma, motor vehicle accident Cervical CR Perched facet of C4–5 67 Trauma, motor vehicle accident Cervical CT Hangman’s fracture, pneumomediastinum 68 Rule out leak status post esophageal dilatation Chest CR Esophageal leak after surgery 69 Motor vehicle accident trauma after striking deer Orbital CT Tripod fracture of orbit 70 Trauma Chest CT Pulmonary laceration, flail chest, pneumothorax, mediastinal hematoma, multiple fractures 71 Trauma, motor vehicle accident C/A/P CT Shock bowel, aspiration pneumonitis
A/P: abdomen and pelvis; β-HCG: human chorionic gonadotropin beta; C/A/P: chest, abdomen, and pelvis; CR: computed radiography; CT: computed tomography; CTA: CT angiogram; MCA: middle cerebral artery; PICC: peripherally inserted central catheter; RUQ: right upper quadrant; US: ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Using the Simulator
Get Radiology Tree app to read full this article<
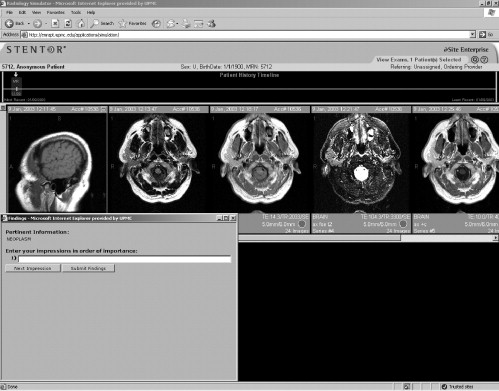
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Resident Participation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
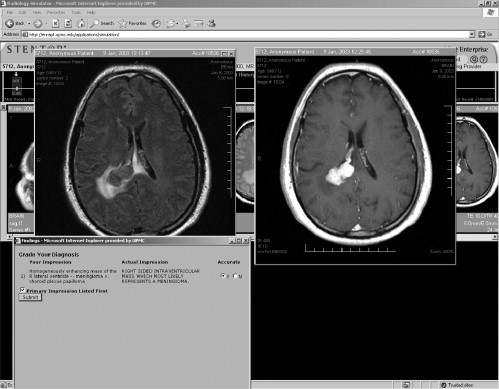
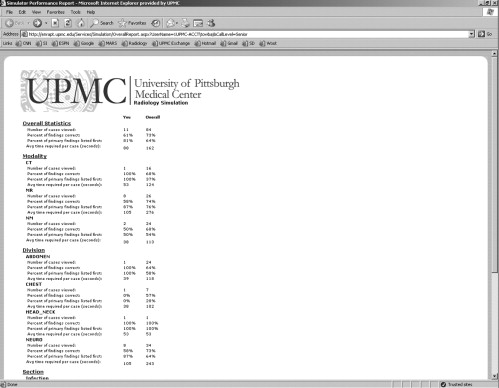
Resident Performance
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Residents’ Subjective Feelings Regarding Call Both Before and After Beginning Call
1 Month Before Beginning Call 1 Month After Beginning Call Difference Question 1: How prepared do you feel for taking call? 1 = not at all prepared, 5 = very well prepared Study group 3.4 3.9 0.5 Control group 3.2 3.4 0.2
1 Month Before Beginning Call 1 Month After Beginning Call Difference Question 2: How nervous are you to begin call? 1 = not at all nervous, 5 = very nervous Study group 3.7 3.6 0.1 Control group 4.4 4.2 0.2
1 Month Before Beginning Call 1 Month After Beginning Call Difference Question 3: How well has the residency program prepared you for taking call? 1 = not at all, 5 = very well Study group 3.0 3.4 0.4 Control group 3.0 3.2 0.2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Resident Performance On Call During the First 3 Months
Study Group Resident Total Number of Cases Viewed Total Number of Cases Faculty Agreed with Resident Total Number of Cases Faculty Gave Resident a Mild Discordance Total Number of Cases Faculty Gave Resident a Significant Discordance Total Number of Cases Judged % of Cases the Faculty Agreed with the Resident % of Cases the Resident Received a Mild Discordance % of Cases the Resident Received a Significant Discordance 1 143 104 4 2 110 94.5 2.8 1.4 2 169 122 15 3 140 87.1 8.9 1.8 3 126 80 13 0 93 86.0 10.3 0 4 280 189 25 4 218 86.7 8.9 1.4 5 258 207 12 4 223 92.8 4.7 1.6 6 79 62 9 0 71 87.3 11.4 0 7 313 234 12 6 252 92.9 3.8 1.9 Overall 1368 998 90 19 1107 90.1 6.6 1.4
Control Group Resident Number Total Number of Cases Viewed Total Number of Cases Faculty Agreed with Resident Total Number of Cases Faculty Gave Resident a Mild Discordance Total Number of Cases Faculty Gave Resident a Significant Discordance Total Number of Cases Judged % of Cases the Faculty Agreed with the Resident % of Cases the Resident Received a Mild Discordance % of Cases the Resident Received a Significant Discordance 8 216 156 11 5 172 90.7 5.1 2.3 9 285 215 18 2 235 91.5 6.3 0.7 10 401 324 25 2 351 92.3 6.2 0.4 11 305 233 12 1 246 94.7 3.9 0.3 12 352 255 24 4 283 90.1 6.8 1.1 Overall 1559 1183 90 14 1287 91.9 5.8 0.8
Please note that the faculty does not need to judge each case. The percent of cases in which the faculty agreed with the resident is determined by dividing the total number of cases the faculty agreed with the resident by the total number of cases judged. The percent of cases the resident received a mild or significant discordance was determined by dividing the total number of cases that the resident received a specific type of discordance by the total number of cases viewed. Because the denominator is different, the percentages do not add up to 100%.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Resident Performance On the First Night of Call
Study Group Resident Number Total Number of Cases Viewed Total Number of Cases Faculty Agreed with Resident Total Number of Cases Faculty Gave Resident a Mild Discordance Total Number of Cases Faculty Gave Resident a Significant Discordance Total Number of Cases Judged % of Cases the Faculty Agreed with the Resident % of Cases the Resident Received a Mild Discordance % of Cases the Resident Received a Significant Discordance 1 42 27 1 0 28 96.4 2.4 0 2 27 17 2 1 20 85.0 7.4 3.7 3 13 10 1 0 11 90.9 7.7 0 4 24 15 1 1 17 88.2 4.2 4.2 5 42 32 6 0 38 84.2 14.3 0 6 43 29 4 1 34 85.3 9.3 2.3 7 34 29 2 2 33 87.9 5.9 5.9 Overall 225 159 17 5 181 87.8 7.6 2.2
Control Group Resident Number Total Number of Cases Viewed Total Number of Cases Faculty Agreed with Resident Total Number of Cases Faculty Gave Resident a Mild Discordance Total Number of Cases Faculty Gave Resident a Significant Discordance Total Number of Cases Judged % of Cases the Faculty Agreed with the Resident % of Cases the Resident Received a Mild Discordance % of Cases the Resident Received a Significant Discordance 8 31 20 1 1 22 90.9 3.2 3.2 9 42 38 2 0 40 95 4.8 0 10 24 19 1 0 20 95 4.2 0 11 37 29 3 0 32 90.6 8.1 0 12 32 23 2 1 26 88.5 6.3 3.2 Overall 166 129 9 2 140 92.1 5.4 1.2
Please note that the faculty does not need to judge each case. The percent of cases in which the faculty agreed with the resident is determined by dividing the total number of cases the faculty agreed with the resident by the total number of cases judged. The percent of cases the resident received a mild or significant discordance was determined by dividing the total number of cases that the resident received a specific type of discordance by the total number of cases viewed. Because the denominator is different, the percentages do not add up to 100%.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Khalifa Y.M., Bogorad D., Gibson V., et. al.: Virtual reality in ophthalmology training. Surv Ophthalmol 2006; 51: pp. 259-273.
2. Kneebone R., Nestel D., Wetzel C., et. al.: The human face of simulation: patient-focused simulation training. Acad Med 2006; 81: pp. 919-924.
3. Ahlberg G., Hultcrantz R., Jaramillo E., et. al.: Virtual reality colonoscopy simulation: a compulsory practice for the future colonoscopist?. Endoscopy 2005; 37: pp. 1198-1204.
4. Wiet G.J., Stredney D., Sessanna D., et. al.: Virtual temporal bone dissection: an interactive surgical simulator. Otolaryngol Head Neck Surg 2002; 127: pp. 79-83.
5. Schaefer J.J.: Simulators and difficult airway management skills. Paediatr Anaesth 2004; 14: pp. 28-37.
6. Wong A.K.: Full scale computer simulators in anesthesia training and evaluation. Can J Anaesth 2004; 51: pp. 455-464.
7. Monsky W.L., Levine D., Mehta T.S., et. al.: Using a sonographic simulator to assess residents before overnight call. AJR Am J Roentgenol 2002; 178: pp. 35-39.
8. Chaer R.A., Derubertis B.G., Lin S.C., et. al.: Simulation improves resident performance in catheter-based intervention: results of a randomized, controlled study. Ann Surg 2006; 244: pp. 343-352.
9. Berry M., Lystig T., Reznick R., et. al.: Assessment of a virtual interventional simulator trainer. J Endovasc Ther 2006; 13: pp. 237-243.
10. Ganguli S., Pedrosa I., Yam C.S., et. al.: Part I: preparing first-year radiology residents and assessing their readiness for on-call responsibilities. Acad Radiol 2006; 13: pp. 764-769.
11. Yam C.S., Kruskal J., Pedrosa I., et. al.: Part II: preparing and assessing first-year radiology resident on-call readiness technical implementation. Acad Radiol 2006; 13: pp. 770-773.
12. LoRusso A.P., Bassignani M.J., Harvey J.A.: Enhanced teaching of screening mammography using an electronic format. Acad Radiol 2006; 13: pp. 782-788.
13. Toms A.P., Kasmai B., Williams S., et. al.: Building an anonymized catalogued radiology museum in PACS: a feasibility study. Br J Radiol 2006; 79: pp. 666-671.
14. Novelline RA. Core curriculum in emergency radiology. American Society of Emergency Radiology, 2006. Available at: http://www.erad.org/download/ASERCoreCurriculum06a.pdf . Accessed December 25, 2006.
15. Towbin AJ, Paterson B, Chang PJ. A computer-based simulator of radiology: an educational tool. Accepted for publication in Radiographics.
16. Fanti V., Marzeddu R., Massazza G., et. al.: A simulator for x-ray images. Radiat Prot Dosimetry 2005; 114: pp. 350-354.
17. Winslow M., Xu X.G., Yazici B.: Development of a simulator for radiographic image optimization. Comput Methods Programs Biomed 2005; 78: pp. 179-190.
18. Branstetter B.F., Morgan M.B., Nesbit C.E., et. al.: Preliminary reports in the emergency department: is a subspecialist radiologist more accurate than a radiology resident?. Acad Radiol 2007; 14: pp. 201-206.
19. Ojutiku O., Haramati L.B., Rakoff S., et. al.: Radiology residents’ on-call interpretation of chest radiographs for pneumonia. Acad Radiol 2005; 12: pp. 658-664.
20. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
21. Ginsberg M.S., King V., Panicek D.M.: Comparison of interpretations of CT angiograms in the evaluation of suspected pulmonary embolism by on-call radiology fellows and subsequently by radiology faculty. AJR Am J Roentgenol 2004; 182: pp. 61-66.
22. Lal N.R., Murray U.M., Eldevik O.P., et. al.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. AJNR Am J Neuroradiol 2000; 2: pp. 124-129.
23. Wysoki M.G., Nassar C.J., Koenigsberg R.A., et. al.: Head trauma: CT scan interpretation by radiology residents versus staff radiologists. Radiology 1998; 208: pp. 125-128.
24. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.