
Rationale and Objectives
Complete clinical information improves the diagnostic capacity of medical imaging, and the radiology requisition is the radiologist’s primary means of receiving clinical information. This study aimed to characterize trends in the quality of clinical information in radiology requisitions at an academic medical center between 2011 and 2016.
Materials and Methods
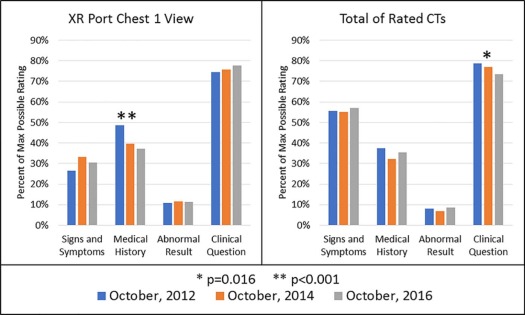
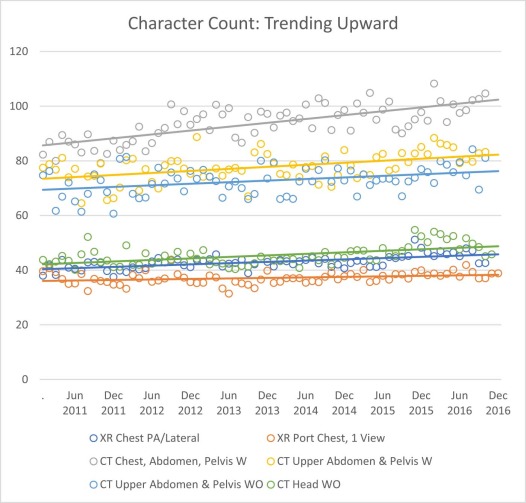
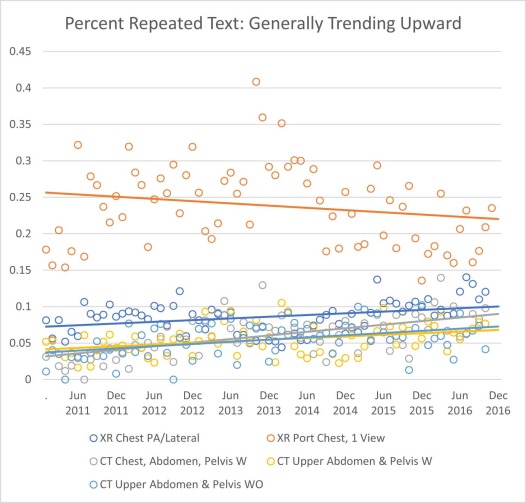
This institution’s requisition form includes two questions: “ Signs and Symptoms: ” and “ Clinical Question to be answered…: ” Requisitions for three studies (CT UPPER ABDOMEN & PELVIS W, CT HEAD WO, and XR PORT CHEST, 1 VIEW) from three selected months were individually rated in four categories of clinical information. Additionally, requisitions for 13 study types were evaluated for character count and for the proportion of requisitions with identical answers to the two questions. A total of 3250 requisitions were individually rated.
Results
There was a decline in the quality of clinical questions in computed tomography requisitions ( P = 0.016) and a decline in the quality of medical history in chest x-ray requisitions ( P < .001). Of the 13 study types, nine had more than 1000 total requisitions (total n = 260,617). Of those nine studies, six showed trends of increasing character length ( P < .001 for each). Four showed an increasing proportion of identical answers to the two questions ( P < .001), and one showed a decreasing proportion of identical answers ( P < .001).
Conclusions
This decline in the quality of clinical information is concerning. Whether it is due to increasing time pressures, a shift in the attitudes of ordering providers, or any other cause, this study demonstrates a declining trend in the quality of communication via the radiology requisition.
Introduction
Radiologists are better able to interpret imaging examinations when they have more complete clinical information. Higher quality clinical information has regularly been shown to increase diagnostic sensitivity, and some trials have shown that it can do so without losing specificity . This effect has not just been demonstrated in experimental settings but has been shown in the context of a radiologist’s regular workflow . Along with clinical information, a specific question can help guide a radiologist’s focus. In patients with acute strokes, requisitions for head computed tomography (CT) scans or magnetic resonance images mentioning a suspicion for a stroke were more likely to result in a correct diagnosis than in those not mentioning a suspicion of stroke . Medical students given a clinical history were more likely to make a correct diagnosis from an image if they suspected the correct diagnosis before viewing that image , suggesting that a requisition that suggests concern for a specific condition would be helpful in diagnosing that condition. Furthermore, most radiologists report desiring more clinical information than is available in the requisitions they receive, and most are discouraged by the difficulty of accessing clinical information through other systems .
Given the clear benefit of clinical information and clinical questions to diagnostic radiology, there has been significant interest in documenting the level of clinical information provided in radiology requisitions, which are the primary means by which a clinician requesting a test communicates with the radiologist who is responsible for the production and interpretation of the examination. Multiple studies have examined how radiology requisitions have been affected by conversion from paper-based ordering systems to electronic ordering systems, with studies generally concluding that the implementation of computerized physician order entry (CPOE) systems improves the quality of clinical information in requisitions . Similarly, multiple studies have documented how radiology requisitions have changed in response to a training or quality improvement effort, with results showing measurable improvement after the quality improvement efforts with variable degrees of regression toward baseline levels within months after the intervention . A study attempted to characterize the completeness of radiology requisitions compared to emergency department provider notes, comparing different shifts, provider levels, and anatomic locations, and it found that attendings and residents tend to give better clinical information than physician extenders and that the quality of clinical information given differs by anatomic location . However, no previous study has examined how the quality of clinical information contained in the radiology requisition may be changing over time independent of any major stimulus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
TABLE 1
Tests Included in Analysis
Name of Test Ordered Name of Test in Analysis CHEST PA/LATERAL—XR XR CHEST PA/LATERAL XR ADULT CHEST PA/LATERAL XR CHEST PA/LATERAL XR PORT CHEST 1V LINE PLCMNT—INITIAL ONLY XR PORT CHEST 1V LINE PLCMNT—INITIAL ONLY XR PORT CHEST 1V LINE PLCMNT—INTL ONLY XR PORT CHEST 1V LINE PLCMNT—NO CHARGE XR PORT CHEST 1V LINE PLCMNT—NO CHARGE XR PORT CHEST, 1 VIEW XR PORT CHEST, 1 VIEW XR PORTABLE CHEST, 1 VIEW XR PORTABLE CHEST, 1VIEW XR PORT CHEST 1V CT CHEST ABDOMEN PELVIS W CT CHEST, ABDOMEN, PELVIS W CT CHEST, ABDOMEN, PELVIS W CT CHEST ABDOMEN PELVIS WO CT CHEST, ABDOMEN, PELVIS WO CT CHEST, ABDOMEN, PELVIS WO CT CHEST, ABDOMEN, PELVIS WWO CT CHEST, ABDOMEN, PELVIS WWO CT CHEST ABDOMEN PELVIS WWO CT CHEST, ABDOMEN, WWO CT CHEST, ABDOMEN, WWO CT UPPER ABD & PELVIS W CT UPPER ABDOMEN & PELVIS W CT UPPER ABD AND PELVIS W CT UPPER ABDOMEN & PELVIS W UPPER ABDOMEN & PELVIS W—CT CT UPPER ABD AND PELVIS WO CT UPPER ABDOMEN & PELVIS WO CT UPPER ABDOMEN & PELVIS WO CT UPPER ABD AND PELVIS WWO CT UPPER ABDOMEN & PELVIS WWO CT UPPER ABDOMEN & PELVIS WWO UPPER ABDOMEN & PELVIS WWO—CT CT UPPER ABDOMEN & PELVIS WWO CONTRAST CT HEAD WO CT HEAD WO CT HEAD WWO CT HEAD WWO
1V, one view; CT, computed tomography; PA, posterior-anterior; PLCMNT, placement; W, with contrast; WO, without contrast; WWO, with and without contrast; XR, x-ray.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 2
Requisitions Identified
Study Type Total RequisitionsXR CHEST PA/LATERAL63,167XR PORT CHEST 1V LINE PLCMNT—INITIAL ONLY4207 XR PORT CHEST 1V LINE PLCMNT—NO CHARGE 628XR PORT CHEST, 1 VIEW110,282CT CHEST, ABDOMEN, PELVIS W10,884CT CHEST, ABDOMEN, PELVIS WO2235 CT CHEST, ABDOMEN, PELVIS WWO 27 CT CHEST, ABDOMEN, WWO 6CT UPPER ABDOMEN & PELVIS W17,263CT UPPER ABDOMEN & PELVIS WO9330CT UPPER ABDOMEN & PELVIS WWO2131CT HEAD WO41,118 CT HEAD WWO 410
1V, one view; PA, posterior-anterior; PLCMNT, placement; W, with contrast; WO, without contrast; WWO, with and without contrast.
Analyzed studies are in bold.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Sample Rated Requisitions
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Trends in Character Count: Green Shading Indicates Increasing Character Count (Color version of table is available online.)
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 5
Trends in Repeated Data: Red Shading Indicates Increasing Repeated Text; Green Shading Indicates Decreasing Repeated Text (Color version of table is available online.)
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Loy C.T., Irwig L.: Accuracy of diagnostic tests read with and without clinical information: a systematic review. JAMA 2004; 292: pp. 1602-1609.
2. Doubilet P., Herman P.G.: Interpretation of radiographs: effect of clinical history. Am J Roentgenol 1981; 137: pp. 1055-1058.
3. Mullins M.E., Lev M.H., Schellingerhout D., et. al.: Influence of availability of clinical history on detection of early stroke using unenhanced CT and diffusion-weighted MR imaging. Am J Roentgenol 2002; 179: pp. 223-228.
4. Suzuki S., Ikusaka M., Ohira Y., et. al.: Effect of diagnostic predictions combined with clinical information on avoiding perceptual errors of computed tomography. Jpn J Radiol 2013; 31: pp. 731-736.
5. Boonn W.W., Langlotz C.P.: Radiologist use of and perceived need for patient data access. J Digit Imaging 2009; 22: pp. 357-362.
6. Alkasab T.K., Alkasab J.R., Abujudeh H.H.: Effects of a computerized provider order entry system on clinical histories provided in emergency department radiology requisitions. J Am Coll Radiol 2009; 6: pp. 194-200.
7. Pirnejad H., Niazkhani Z., Bal R.: Clinical communication in diagnostic imaging studies: mixed-method study of pre-and post-implementation of a hospital information system. Appl Clin Inform 2013; 4: pp. 541.
8. Pevnick J.M., Herzik A.J., Li X., et. al.: Effect of computerized physician order entry on imaging study indication. J Am Coll Radiol 2015; 12: pp. 70-74.
9. Benard M., Bouaud J., Marsault C., et. al.: Diagnostic imaging requisition quality when using an electronic medical record: a before-after study. Stud Health Technol Inform 2015; pp. 364-368.
10. Hawkins C.M., Anton C.G., Bankes W.M., et. al.: Improving the availability of clinical history accompanying radiographic examinations in a large pediatric radiology department. Am J Roentgenol 2014; 202: pp. 790-796.
11. Gunderman R.B., Phillips M.D., Cohen M.D.: Improving clinical histories on radiology requisitions. Acad Radiol 2001; 8: pp. 299-303.
12. Kalisz K., Garg V., Basques K., et. al.: Emergency room plain radiograph imaging study indications: an analysis of quality and trends at a large academic medical center. Acad Radiol 2016; 23: pp. 1582-1586.
13. Bosmans J.M., Weyler J.J., Parizel P.M.: Structure and content of radiology reports, a quantitative and qualitative study in eight medical centers. Eur J Radiol 2009; 72: pp. 354-358.