
Rationale and Objectives
To investigate whether “full” iterative reconstruction, a knowledge-based iterative model reconstruction (IMR), enables radiation dose reduction by 80% at cardiac computed tomography (CT).
Materials and Methods
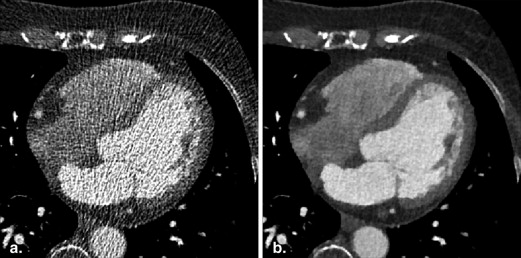
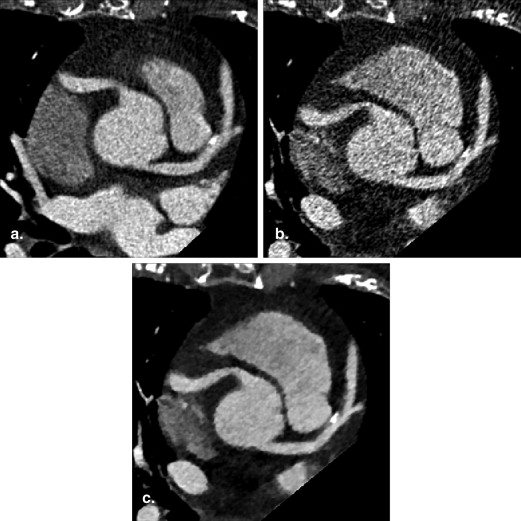
A total of 23 patients (15 men, eight women; mean age 64.3 ± 13.4 years) who underwent retrospectively electrocardiography-gated cardiac CT with dose modulation were evaluated. We compared full-dose (FD; 730 mAs) images reconstructed with filtered back projection (FBP) technique and the low-dose (LD; 146 mAs) images reconstructed with FBP and IMR techniques. Objective and subjective image quality parameters were compared among the three different CT images.
Results
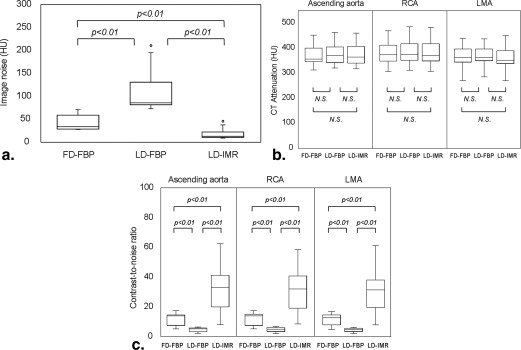
There was no significant difference in the CT attenuation among the three reconstructions. The mean image noise of LD-IMR (18.3 ± 10.6 Hounsfield units [HU]) was significantly lowest among the three reconstructions (41.9 ± 15.3 HU for FD-FBP and 109.9 ± 42.6 HU for LD-FBP; P < .01). The contrast-to-noise ratio of LD-IMR was better than that of FD-FBP and LD-FBP ( P < .01). Visual evaluation score was also highest for LD-IMR.
Conclusions
The IMR can provide improved image quality at super-low-dose cardiac CT with 20% of the standard tube current.
Cardiac computed tomography (CT) has emerged as a useful diagnostic imaging modality for the noninvasive assessment of coronary artery disease in select patient groups . Although the diagnostic performance of cardiac CT is high for the detection and exclusion of obstructive coronary artery disease , there are concerns regarding potential stochastic risks related to ionizing radiation . According to Hausleiter et al. , the mean effective dose at cardiac CT was 12 mSv; the range was 5–30 mSv. To minimize the patient dose, conventional electrocardiographic (ECG)-dependent tube current modulation is used, achieving moderate dose savings of 37%–40% . Another radiation dose saving technique, prospective “step-and-shoot” ECG-triggering, allows for a radiation dose reduction of 77%–79% . However, it requires a steady low heart rate (HR), which is not obtainable in all patients, and therefore, retrospectively ECG-gated cardiac CT is still useful for some patients. Also, the evaluation of cardiac function is not possible because images are acquired at a single, predetermined, end-diastolic, quiescent phase. It is critically important to balance the desire for low-radiation doses with the likelihood of obtaining diagnostically useful images.
An iterative reconstruction algorithm for CT was introduced to help reduce the quantum noise associated with standard convolution–filtered back projection (FBP) reconstruction algorithms . Studies that evaluated the quality of images acquired with a hybrid type of iterative reconstruction indicated that a radiation dose reduction of 23%–66% was possible while maintaining the image quality , but a certain amount of image noise and artifacts are still present. Iterative model reconstruction (IMR), a fully iterative algorithm, represents the latest advance in the field of reconstruction techniques. It applies a knowledge-based approach that yields improved image quality and virtually noise-free images through the iterative minimization of the penalty-based cost function. IMR technique can reconstruct the cardiac CT images within 5 minutes, and we posit it can be applicable in clinical practice. To our knowledge, there is no reported study involving comparative evaluation on a clinical setting of the knowledge-based iterative reconstruction algorithm and FBP algorithm at cardiac CT.
Get Radiology Tree app to read full this article<
Materials and methods
Phantom Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Study
Get Radiology Tree app to read full this article<
Study population
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics
Characteristics Value Number of patients 23 Age (years) 64.3 ± 13.4 Female/male 8/15 Body weight (kg) 62.0 ± 9.2 Body mass index (kg/m 2 ) 23.1 ± 2.5 Average heart rate (beats/min) 54.5 ± 3.8
Data are mean ± standard deviation.
Get Radiology Tree app to read full this article<
Cardiac CT acquisition
Get Radiology Tree app to read full this article<
CT image reconstruction
Get Radiology Tree app to read full this article<
Qualitative analysis of image quality
Get Radiology Tree app to read full this article<
Quantitative analysis of image quality
Get Radiology Tree app to read full this article<
Statistical analysis
Get Radiology Tree app to read full this article<
Results
Phantom Study
Get Radiology Tree app to read full this article<
Table 2
Image Quality Assessment in the Phantom Study
Parameter FD-FBP LD-FBP LD-IMR_P_ Value Visual score 3.5 ± 0.5 2.0 ± 0.4 3.3 ± 0.5 <.01 CT attenuation (HU) 373.1 ± 42.2 378.0 ± 43.9 375.7 ± 43.7 .33 Image noise (HU) 378.0 ± 49.4 384.8 ± 53.8 379.9 ± 52.0 <.01 ∗ Contrast-to-noise ratio 366.2 ± 49.3 368.1 ± 47.1 359.7 ± 49.4 <.01 ∗
FD-FBP, full-dose filtered back projection; LD-FBP, low-dose filtered back projection; LD-IMR, low-dose iterative model reconstruction.
Data are the mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Study
Qualitative analysis of image quality
Get Radiology Tree app to read full this article<
Table 3
Qualitative Assessment of Image Quality in Clinical Study
Parameter FD-FBP LD-FBP LD-IMR_P_ Value Image noise 3.0 ± 0.6 1.2 ± 0.4 3.8 ± 0.4 <.01 ∗ Beam-hardening artifact 2.5 ± 0.9 1.1 ± 0.2 3.8 ± 0.5 <.01 ∗ Vessel sharpness 3.6 ± 0.5 1.4 ± 0.5 3.1 ± 0.3 <.01 ∗ Overall image quality 3.7 ± 0.5 1.2 ± 0.4 3.1 ± 0.2 <.01 ∗
FD-FBP, full-dose filtered back projection; LD-FBP, low-dose filtered back projection; LD-IMR, low-dose iterative model reconstruction.
Data are the mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Quantitative analysis of image quality
Get Radiology Tree app to read full this article<
Table 4
Quantitative Assessment of Image Quality in Clinical Study
Parameter FD-FBP LD-FBP LD-IMR_P_ Value Contrast enhancement (HU) Ascending aorta 373.1 ± 42.2 378.0 ± 43.9 375.7 ± 43.7 .92 Proximal RCA 378.0 ± 49.4 384.8 ± 53.8 379.9 ± 52.0 .90 LMA 366.2 ± 49.3 368.1 ± 47.1 359.7 ± 49.4 .92 Image noise (HU) 41.9 ± 15.3 109.8 ± 42.6 18.3 ± 10.6 <.01 ∗ Contrast-to-noise ratio Ascending aorta 12.1 ± 3.9 4.7 ± 1.5 32.0 ± 14.3 <.01 ∗ Proximal RCA 12.2 ± 3.9 4.7 ± 1.5 32.1 ± 14.3 <.01 ∗ LMA 11.8 ± 3.6 4.5 ± 1.3 30.3 ± 12.9 <.01 ∗
FD-FBP, full-dose filtered back projection; HU, Hounsfield units; LD-FBP, low-dose filtered back projection; LD-IMR, low-dose iterative model reconstruction; LMA, left main coronary artery; RCA, right coronary artery.
Data are the mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Taylor A.J., Cerqueira M., Hodgson J.M., et. al.: ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. Circulation 2010; 122: pp. e525-e555.
2. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
3. Miller J.M., Rochitte C.E., Dewey M., et. al.: Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 2008; 359: pp. 2324-2336.
4. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
5. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
6. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
7. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
8. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
9. Silva A.C., Lawder H.J., Hara A., et. al.: Innovations in CT dose reduction strategy: application of the adaptive statistical iterative reconstruction algorithm. AJR Am J Roentgenol 2010; 194: pp. 191-199.
10. Sagara Y., Hara A.K., Pavlicek W., et. al.: comparison of low-dose CT with adaptive statistical iterative reconstruction and routine-dose CT with filtered back projection in 53 patients. AJR Am J Roentgenol 2010; 195: pp. 713-719.
11. Nakaura T., Nakamura S., Maruyama N., et. al.: Low contrast agent and radiation dose protocol for hepatic dynamic CT of thin adults at 256-detector row CT: effect of low tube voltage and hybrid iterative reconstruction algorithm on image quality. Radiology 2012; 264: pp. 445-454.
12. Cademartiri F., Nieman K., van der Lugt A., et. al.: Intravenous contrast material administration at 16-detector row helical CT coronary angiography: test bolus versus bolus-tracking technique. Radiology 2004; 233: pp. 817-823.
13. Abada H.T., Larchez C., Daoud B., et. al.: MDCT of the coronary arteries: feasibility of low-dose CT with ECG-pulsed tube current modulation to reduce radiation dose. AJR Am J Roentgenol 2006; 186: pp. S387-S390.
14. Oda S., Utsunomiya D., Funama Y., et. al.: A low tube voltage technique reduces the radiation dose at retrospective ECG-gated cardiac computed tomography for anatomical and functional analyses. Acad Radiol 2011; 18: pp. 991-999.
15. Schoenhagen P.: Back to the future: coronary CT angiography using prospective ECG triggering. Eur Heart J 2008; 29: pp. 153-154.
16. Klass O., Jeltsch M., Feuerlein S., et. al.: Prospectively gated axial CT coronary angiography: preliminary experiences with a novel low-dose technique. Eur Radiol 2009; 19: pp. 829-836.
17. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
18. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for radiation dose reduction in chest CT: comparison with the adaptive statistical iterative reconstruction technique. Eur Radiol 2012; 22: pp. 1613-1623.
19. Singh S., Kalra M.K., Do S., et. al.: Comparison of hybrid and pure iterative reconstruction techniques with conventional filtered back projection: dose reduction potential in the abdomen. J Comput Assist Tomogr 2012; 36: pp. 347-353.
20. Scheffel H., Stolzmann P., Schlett C.L., et. al.: Coronary artery plaques: cardiac CT with model-based and adaptive-statistical iterative reconstruction technique. Eur J Radiol 2012; 81: pp. e363-e369.
21. Boone J.M.: Determination of the presampled MTF in computed tomography. Med Phys 2001; 28: pp. 356-360.
22. Siewerdsen J.H., Cunningham I.A., Jaffray D.A.: A framework for noise-power spectrum analysis of multidimensional images. Med Phys 2002; 29: pp. 2655-2671.
23. McCollough C.H., Chen G.H., Kalender W., et. al.: Achieving routine submillisievert CT scanning: report from the summit on management of radiation dose in CT. Radiology 2012; 264: pp. 567-580.