
Rationale and Objectives
To investigate the effect of low-tube-voltage technique on a cardiac computed tomography (CT) for coronary arterial and cardiac functional analyses and radiation dose in slim patients.
Materials and Methods
We enrolled 80 patients (52women, 28 men; mean age, 68.7 ± 8.9 years) undergoing retrospective electrocardiogram-gated 64-slice cardiac CT. Forty were subjected to the low (80-kV) and 40 to the standard (120-kV) tube-voltage protocol. Quantitative parameters of the coronary arteries (ie, CT attenuation, image noise, and the contrast-to-noise ratio [CNR]) were calculated, as were the effective radiation dose and the figure of merit (FOM). Each coronary artery segment was visually evaluated using a 5-point scale. Cardiac function calculated by using low-tube-voltage cardiac CT was compared with that on echocardiographs.
Results
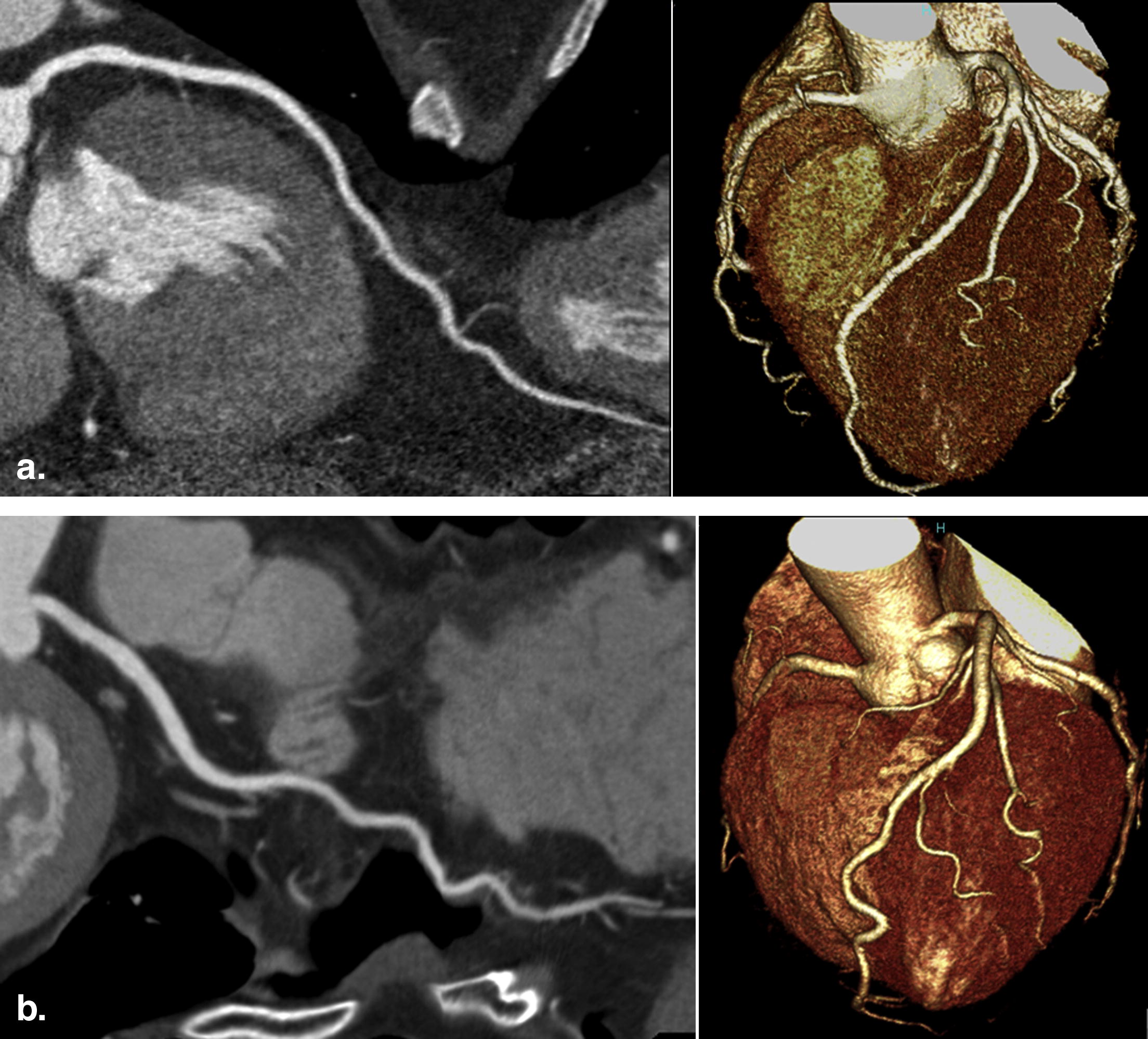
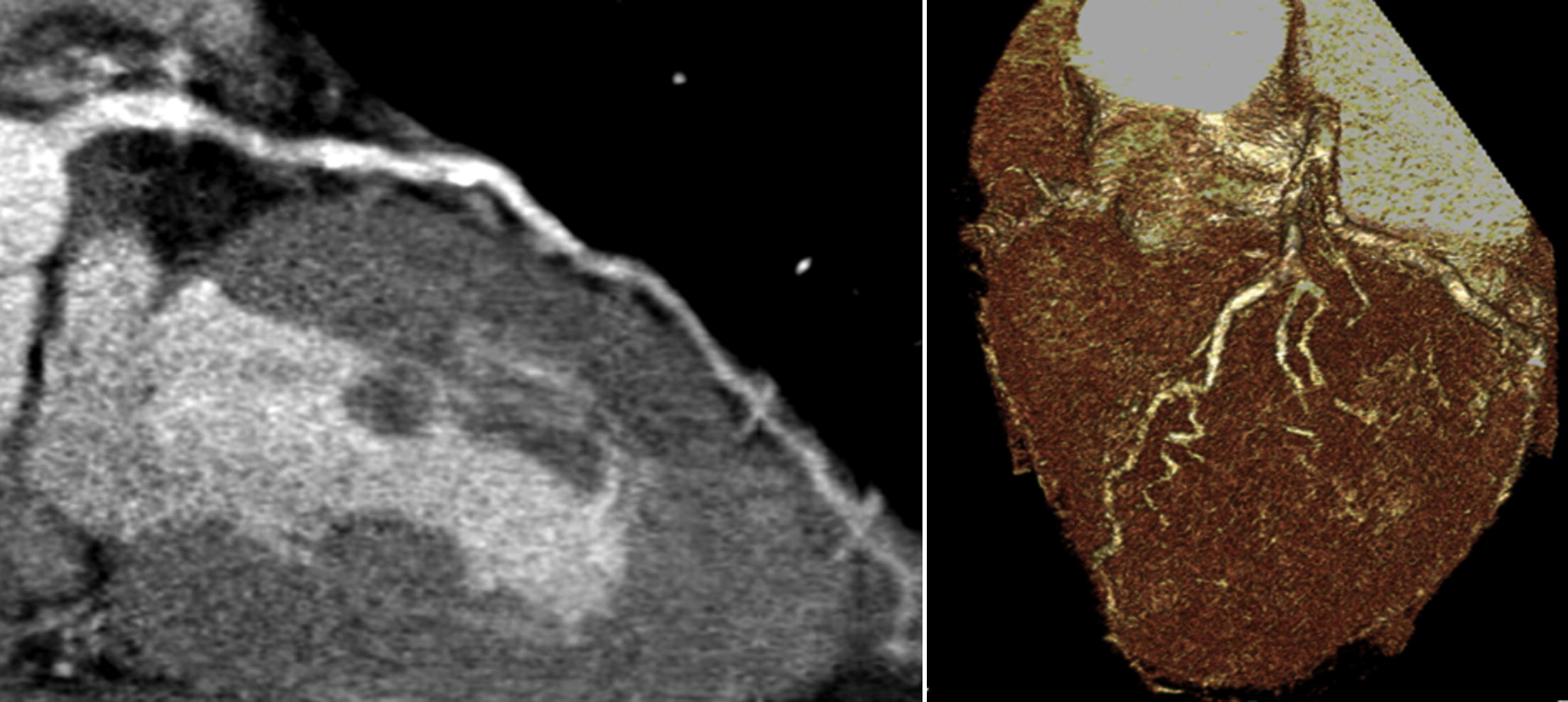
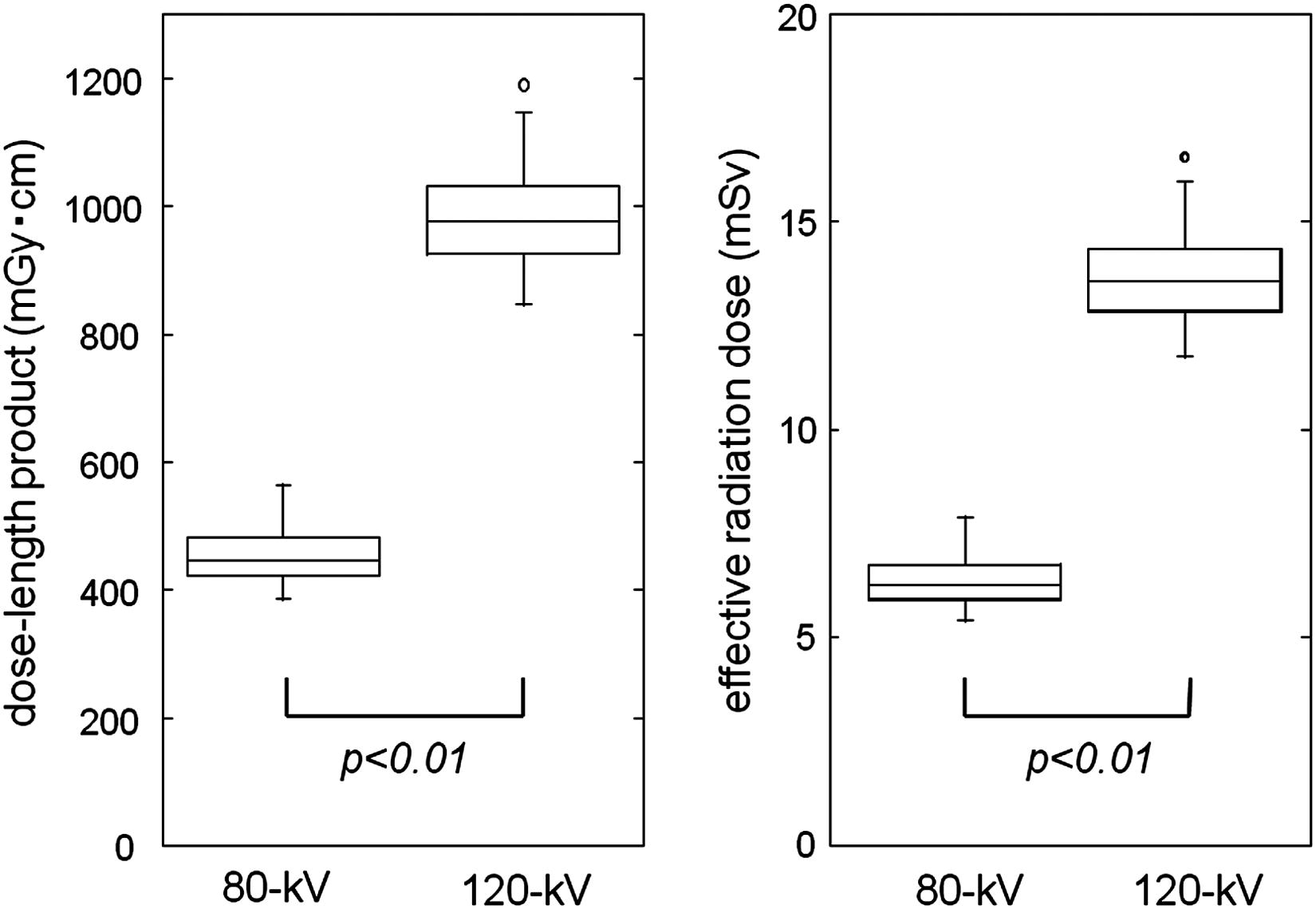
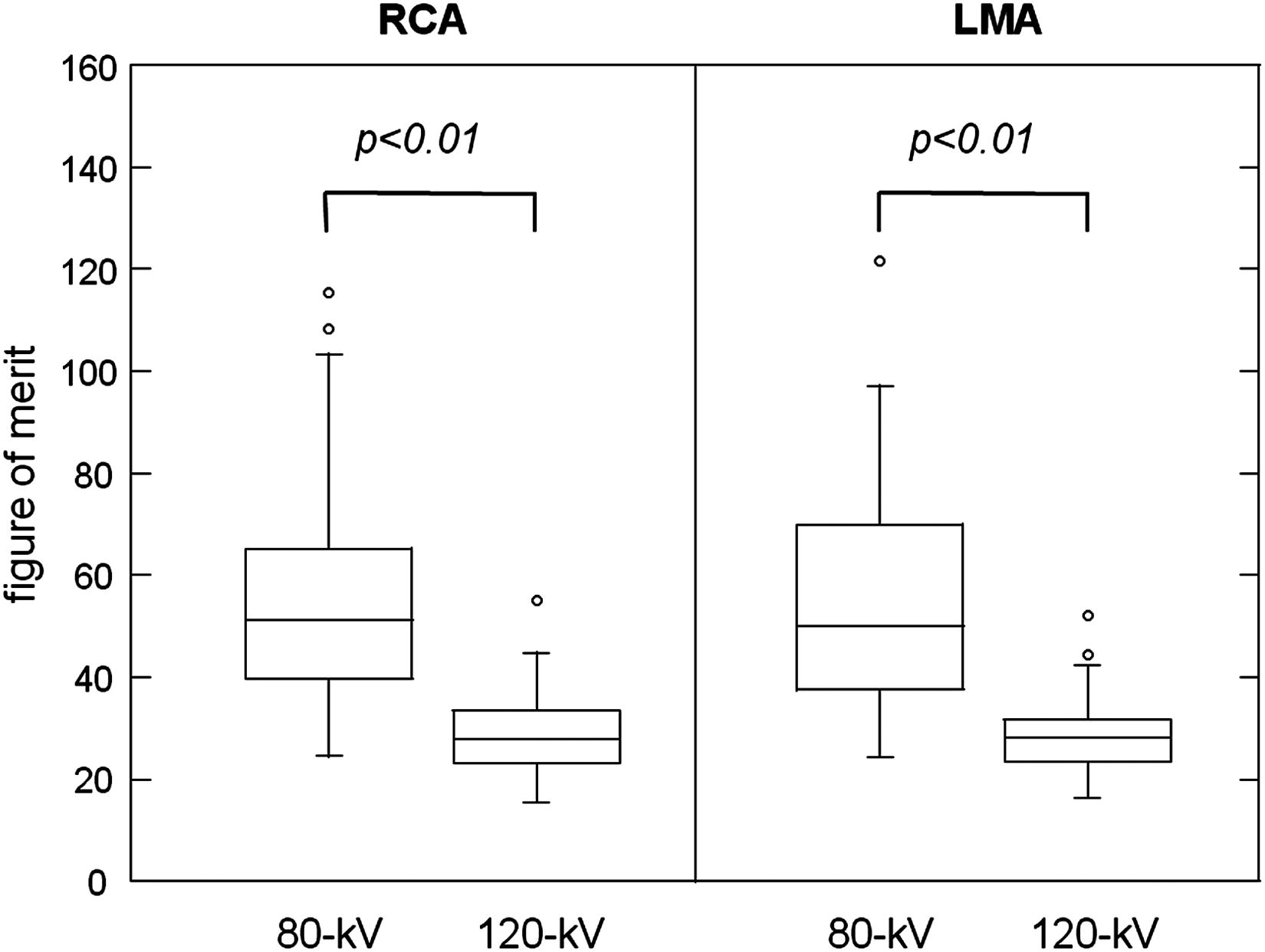
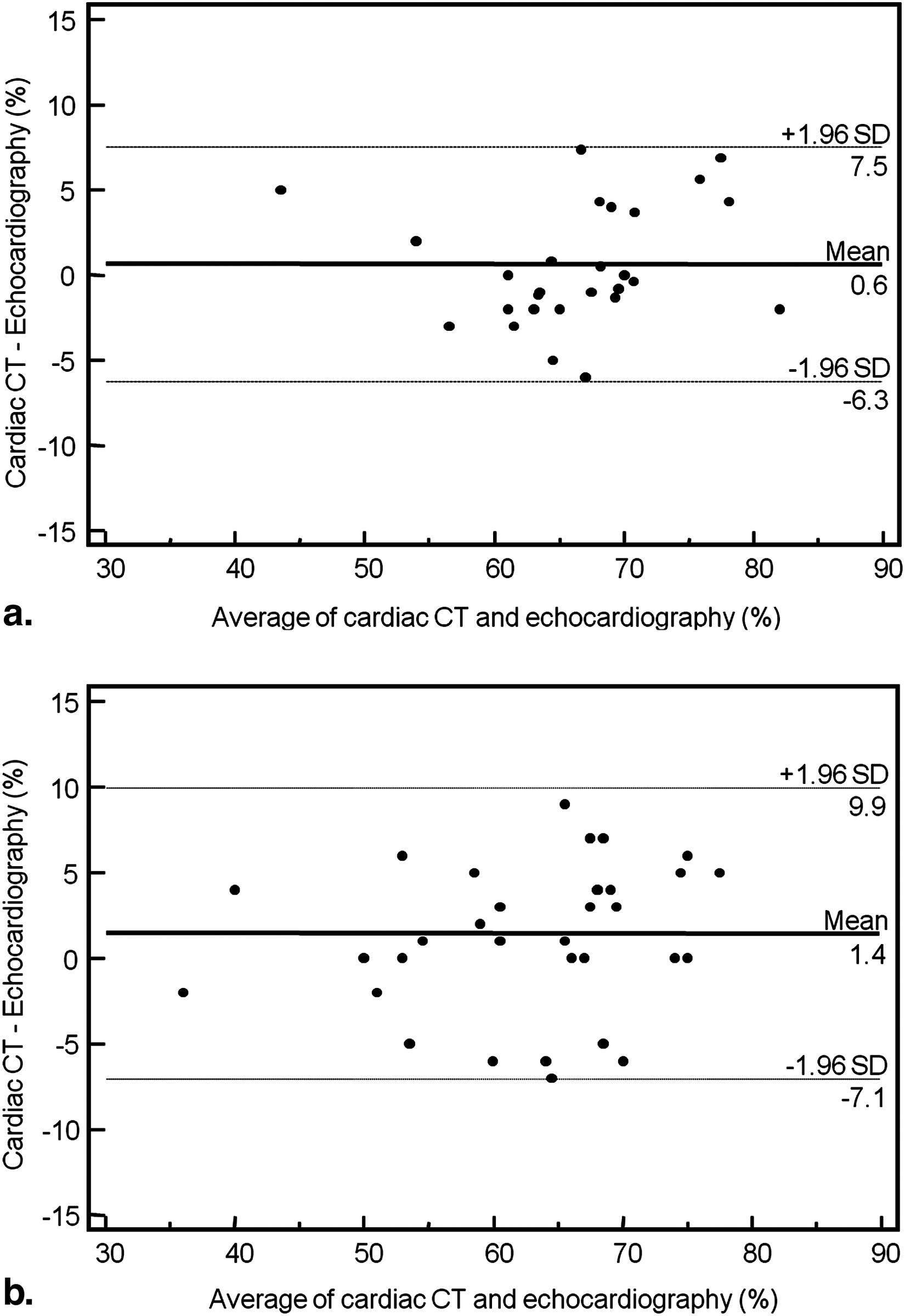
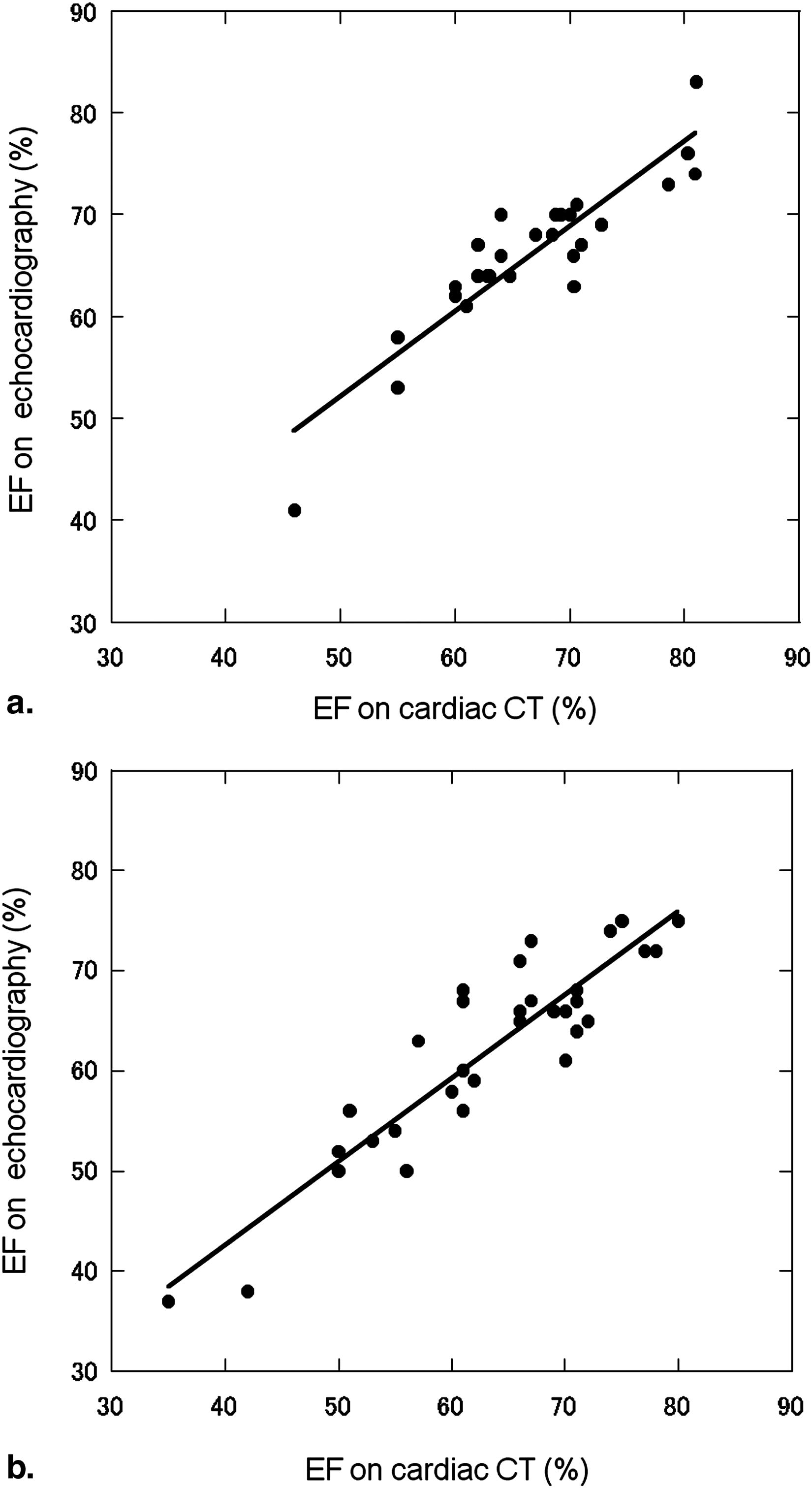
CT attenuation and image noise were significantly higher at 80- than 120-kV ( P < .01). CNR of the left and right coronary artery was 18.4 ± 3.8 and 18.5 ± 3.3, respectively, at 80 kV; these values were 19.7 ± 2.7 and 19.8 ± 2.8 at 120 kV; the difference was not significant. The estimated effective radiation dose was significantly lower at 80 than 120 kV (6.3 ± 0.6 vs. 13.9 ± 1.1 mSv, P < .01) and FOM was significantly higher at 80 than 120 kV ( P < .01). At visual assessment, 99% of the coronary segments were diagnostic quality; the two protocols did not differ significantly. We observed a strong correlation and good agreement between low-tube-voltage cardiac CT and echocardiography for cardiac functional analyses.
Conclusion
Low-tube-voltage cardiac CT significantly reduced the radiation dose by approximately 55% in slim patients while maintaining anatomical image quality and accuracy of cardiac functional analysis.
Cardiac computed tomography (CT) using multidetector CT (MDCT) yields high diagnostic accuracy for the evaluation of coronary artery stenosis and cardiac function . However, the widespread use of cardiac CT raises concerns with respect to radiation exposure. At 64-slice MDCT, the radiation exposure is high; it ranges from 11–15 mSv to 21 mSv for the coronary artery and from 14 to 26 mSv for coronary bypass graft studies with an extended scan length. To minimize the patient dose, conventional electrocardiogram (ECG)-dependent tube current modulation is used; at 37–40%, the savings from this technique are moderate . Another recently-implemented low-dose CT technique is prospective “step-and-shoot” ECG triggering. This technique allows for a radiation dose reduction of 77–79% . However, it requires a regular, low heart rate, which may not be obtainable in all patients, and the evaluation of cardiac function is not possible because images are acquired during end-diastole only. Strategies for reducing the radiation dose for anatomical and functional analyses at cardiac CT involve lowering the tube voltage. The use of a low-tube-voltage technique drastically reduces the radiation dose and effectively increases contrast enhancement . However, with the low-tube-voltage technique, the transmitted radiation is decreased and image noise is increased; this may constitute a disadvantage in clinical practice where diagnostic image quality must be maintained. To our knowledge, the effects of the low-tube-voltage technique on anatomical and functional analyses at cardiac CT have not been adequately assessed.
We investigated the effects of low-tube-voltage retrospective ECG-gated cardiac CT on qualitative and quantitative image quality parameters and the radiation dose in slim patients by comparing low- (80 kV) and standard tube-voltage settings (120 kV).
Materials and methods
Get Radiology Tree app to read full this article<
Study Population
Get Radiology Tree app to read full this article<
Cardiac CT Examination Technique
Get Radiology Tree app to read full this article<
Qualitative Image Quality Analysis
Get Radiology Tree app to read full this article<
Quantitative Image Quality Analysis
Get Radiology Tree app to read full this article<
Evaluation of the CT Radiation Dose
Get Radiology Tree app to read full this article<
Evaluation of Cardiac Function
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographic Data of Patients
80-kV Protocol 120-kV Protocol_P_ Value Number of patients 40 40 Age 68.3 ± 8.2 69.0 ± 9.6 .71 Sex (male/female) 13/27 15/25 .64 Body weight (kg) 50.5 ± 5.9 51.7 ± 7.9 .45 Body mass index (kg/m 2 ) 20.7 ± 2.2 21.1 ± 2.3 .39 Heart rate (beats/minute) 56.5 ± 7.4 59.4 ± 6.8 .08
Get Radiology Tree app to read full this article<
Qualitative Image Quality
Get Radiology Tree app to read full this article<
Table 2
Qualitative Assessment of Overall Image Quality
80-kV Protocol 120-kV Protocol_P_ Value Total number of evaluated segments 320 320 Mean score 4.83 4.82 .80 Diagnostic image 316 (98.8) 318 (99.4) .41 Nondiagnostic image 4 (1.3) 2 (0.6) .41
Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Quantitative Image Quality
Get Radiology Tree app to read full this article<
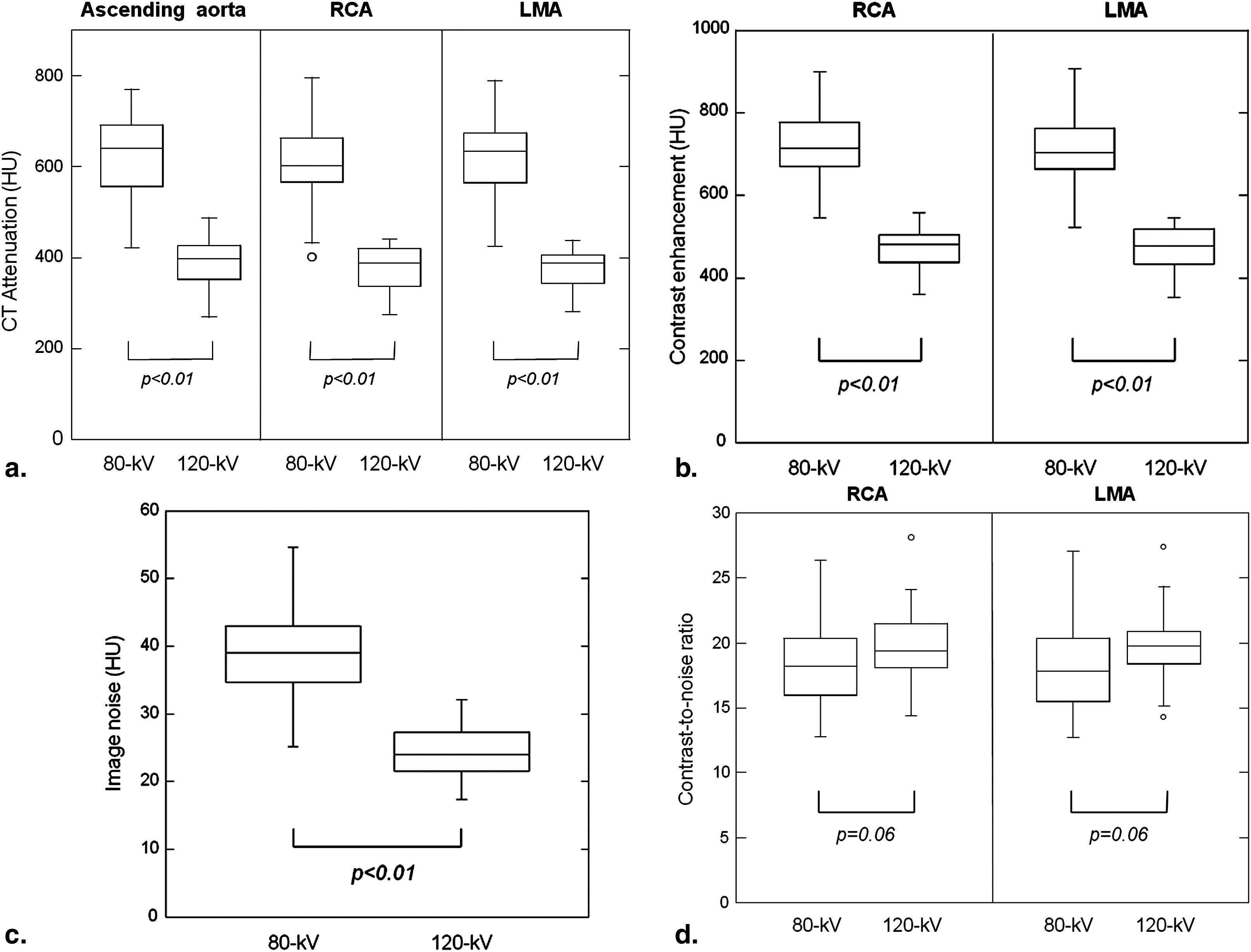
Table 3
Quantitative Assessment of Image Quality
80-kV Protocol 120-kV Protocol_P_ Value CT attenuation (HU) Ascending aorta 624.9 ± 88.1 388.2 ± 51.8 <.01 Proximal RCA 613.8 ± 81.4 374.7 ± 41.1 <.01 LMA 612.4 ± 89.0 374.3 ± 50.8 <.01 Contrast enhancement (HU) Proximal RCA 715.2 ± 78.9 472.1 ± 45.7 <0.01 LMA 713.8 ± 88.0 471.7 ± 55.4 <0.01 Image noise (HU) 39.6 ± 6.3 24.3 ± 3.6 <0.01 CNR Proximal RCA 18.5 ± 3.3 19.8 ± 2.8 0.06 LMA 18.4 ± 3.8 19.7 ± 2.7 0.06
CNR, contrast-to-noise ratio; HU, Hounsfield units; LMA, left main coronary artery; RCA, right coronary artery.
Data are presented as the mean ± SD.
Get Radiology Tree app to read full this article<
CT Radiation Dose and FOM
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cardiac Function
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
2. Scheffel H., Alkadhi H., Plass A., et. al.: Accuracy of dual-source CT coronary angiography: First experience in a high pre-test probability population without heart rate control. Eur Radiol 2006; 16: pp. 2739-2747.
3. Juergens K.U., Grude M., Fallenberg E.M., et. al.: Using ECG-gated multidetector CT to evaluate global left ventricular myocardial function in patients with coronary artery disease. AJR Am J Roentgenol 2002; 179: pp. 1545-1550.
4. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
5. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
6. Hermann F., Martinoff S., Meyer T., et. al.: Reduction of radiation dose estimates in cardiac 64-slice CT angiography in patients after coronary artery bypass graft surgery. Invest Radiol 2008; 43: pp. 253-260.
7. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
8. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
9. Funama Y., Awai K., Nakayama Y., et. al.: Radiation dose reduction without degradation of low-contrast detectability at abdominal multisection CT with a low-tube voltage technique: phantom study. Radiology 2005; 237: pp. 905-910.
10. Nakayama Y., Awai K., Funama Y., et. al.: Abdominal CT with low tube voltage: preliminary observations about radiation dose, contrast enhancement, image quality, and noise. Radiology 2005; 237: pp. 945-951.
11. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Direction Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
12. Cademartiri F., Nieman K., van der Lugt A., et. al.: Intravenous contrast material administration at 16-detector row helical CT coronary angiography: test bolus versus bolus-tracking technique. Radiology 2004; 233: pp. 817-823.
13. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the ad hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
14. Menzel H.Schibilla H.Teunen D.European guidelines on quality criteria for computed tomography. Publication no. EUR 16262 EN.2000.European CommissionLuxembourg, Luxembourg:
15. Samei E., Dobbins J.T., Lo J.Y., et. al.: A framework for optimising the radiographic technique in digital X-ray imaging. Radiat Prot Dosim 2005; 114: pp. 220-229.
16. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
17. Vanhoenacker P.K., Heijenbrok-Kal M.H., Van Heste R., et. al.: Diagnostic performance of multidetector CT angiography for assessment of coronary artery disease: meta-analysis. Radiology 2007; 244: pp. 419-428.
18. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
19. Nakayama Y., Awai K., Funama Y., et. al.: Lower tube voltage reduces contrast material and radiation doses on 16-MDCT aortography. AJR Am J Roentgenol 2006; 187: pp. W490-W497.
20. Schueller-Weidekamm C., Schaefer-Prokop C.M., Weber M., et. al.: CT angiography of pulmonary arteries to detect pulmonary embolism: improvement of vascular enhancement with low kilovoltage settings. Radiology 2006; 241: pp. 899-907.
21. Leschka S., Stolzmann P., Schmid F.T., et. al.: Low kilovoltage cardiac dual-source CT: attenuation, noise, and radiation dose. Eur Radiol 2008; 18: pp. 1809-1817.
22. Yanaga Y., Awai K., Nakaura T., et. al.: Effect of contrast injection protocols with dose adjusted to the estimated lean patient body weight on aortic enhancement at CT angiography. AJR Am J Roentgenol 2009; 192: pp. 1071-1078.
23. Abada H.T., Larchez C., Daoud B., et. al.: MDCT of the coronary arteries: Feasibility of low-dose CT with ECG-pulsed tube current modulation to reduce radiation dose. AJR Am J Roentgenol 2006; 186: pp. S387-S390.
24. Feuchtner G.M., Jodocy D., Klauser A., et. al.: Radiation dose reduction by using 100-kV tube voltage in cardiac 64-slice computed tomography: a comparative study. Eur J Radiol 2009; 75: pp. e51-e56.
25. Hausleiter J., Meyer T., Hermann F., et. al.: Estimated radiation dose associated with cardiac CT angiography. JAMA 2009; 301: pp. 500-507.
26. Poll L.W., Cohnen M., Brachten S., et. al.: Dose reduction in multi-slice CT of the heart by use of ECG-controlled tube current modulation (“ECG pulsing”): phantom measurements. Rofo 2002; 174: pp. 1500-1505.
27. Schoenhagen P.: Back to the future: coronary CT angiography using prospective ECG triggering. Eur Heart J 2008; 29: pp. 153-154.
28. Klass O., Jeltsch M., Feuerlein S., et. al.: Prospectively gated axial CT coronary angiography: preliminary experiences with a novel low-dose technique. Eur Radiol 2009; 19: pp. 829-836.
29. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
30. Marin D., Nelson R.C., Schindera S.T., et. al.: Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm–initial clinical experience. Radiology 2010; 254: pp. 145-153.
31. Brooks R.A.: A quantitative theory of the Hounsfield unit and its application to dual energy scanning. J Comput Assist Tomogr 1977; 1: pp. 487-493.
32. Sigal-Cinqualbre A.B., Hennequin R., Abada H.T., et. al.: Low-kilovoltage multi-detector row chest CT in adults: feasibility and effect on image quality and iodine dose. Radiology 2004; 231: pp. 169-174.