
Rationale and Objectives
To determine the accuracy of 64-section coronary computed tomography angiography (CCTA) in predicting 30 day major adverse cardiac events (MACE) for patients presenting with symptoms concerning for acute coronary syndrome (ACS).
Materials and Methods
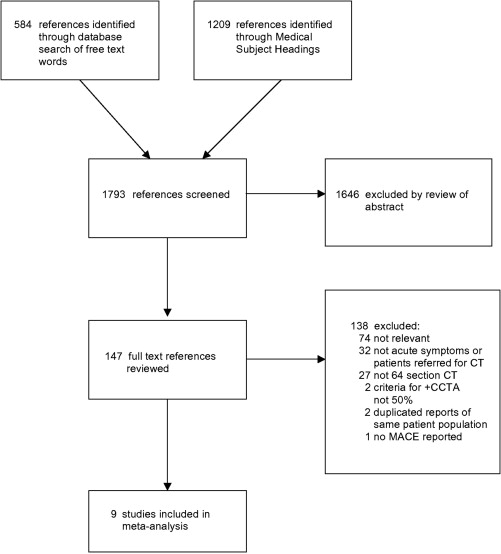
Electronic databases between January 1, 2005, and May, 1, 2011, and reference lists from relevant published research articles were searched. We included studies on adult patients who presented with active symptoms suggestive of ACS, had immediate 64-section CCTA performed and were assessed for MACE at a minimum of 30 days past their initial presentation. Studies had to report or provide sufficient detail to determine sensitivity, specificity, positive predictive value, and negative predictive value in relation to MACE using a 50% diameter stenosis as cutoff criterion for coronary artery disease.
Results
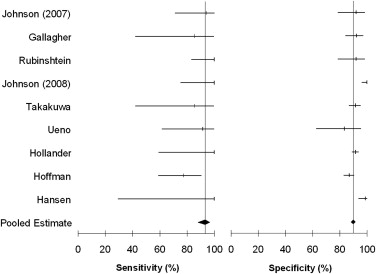
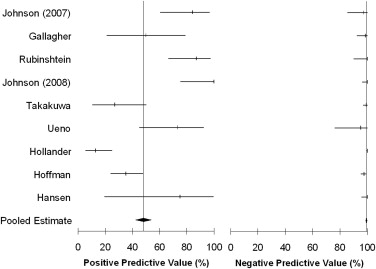
Nine studies were included for a total of 1559 patients studied (42.3% women, mean age 51.9 ± 10.6). Patients ranged from low to intermediate risk for ACS. All had initial inconclusive electrocardiograms and negative cardiac biomarker results. A total of 14.8% of patients had a positive CCTA result. The pooled sensitivity was 93.3% (95% CI 88.3%–96.6%), specificity was 89.9% (95% CI 88.3%–91.3%), positive predictive value was 48.1% (95% CI 42.5%–53.8%), and negative predictive value was 99.3% (95% CI 98.7%–99.6%).
Conclusion
Sixty-four section CCTA had a 99.3% negative predictive value in excluding MACE for 30 days after initial symptom presentation in 85.2% of our study population. Although the value of 64-section CCTA is best for identifying patients who can safely be discharged home, it is less useful for patients who have positive results.
In 2006, the US prevalence of coronary artery disease (CAD) was 80 million people . Emergency departments (ED) saw more than 6.3 million patients complaining of chest pain and related symptoms and admitted 1.976 million patients into hospitals . More than 65% of these admitted patients were ultimately not found to have an acute coronary syndrome (ACS) , resulting in an estimated loss of $6–8 billion per year to the US health care system . Detecting ACS in patients with symptoms such as chest, back and arm pain, shortness of breath, nausea, and weakness is challenging. High-risk patients are appropriately admitted into the hospital and very low-risk patients are discharged to home. But the patients with some risk of ACS—those without diagnostic electrocardiogram (ECG) changes or cardiac biomarkers—are more difficult to disposition.
There have been numerous studies attempting to accurately risk-stratify patients but no single test has reliably proven to be >99% accurate in large numbers to exclude ACS in symptomatic patients . This may partially explain the estimated 2%–5% rate of missed ACS in the ED . A highly accurate diagnostic test that can exclude ACS could potentially save the US health care system billions of dollars. Coronary computed tomography angiography (CCTA) has emerged in recent years as a test that may be able to reliably exclude ACS. Using this technology, there have been many studies examining 64-section CCTA and correlating the findings to invasive coronary angiography (ICA) . Several systematic reviews and meta-analyses correlated CCTA with ICA but none of them focused on immediate CCTA for patients with acute symptoms . Although ICA is considered the gold standard for detecting CAD, it is not practical for widespread use in undifferentiated chest pain patients: it is not routinely available in most acute settings, it would not likely improve the outcome of the majority of patients and it carries a risk of major complications. A more practical approach may be noninvasive CCTA, which correlates well with ICA. Patients found to have mild to no CAD on ICA have been shown to have good long survival rates and can presumably be safely discharged from an ED.
Get Radiology Tree app to read full this article<
Materials and methods
Search Strategy
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Selection of Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Extraction/Collection and Processing
Get Radiology Tree app to read full this article<
Quality Assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Outcome Measures
Get Radiology Tree app to read full this article<
Primary Data Analyses
Get Radiology Tree app to read full this article<
Results
Quantitative Analysis
Get Radiology Tree app to read full this article<
Table 1
Study Characteristics
Author No. Patients for Meta-analysis Patient Population (ACS Risk Criterion) Age (Year ± SD) % Men % White Triple Rule-out Study MACE Follow-up (Months) Johnson et al, 2007 55 Low to intermediate risk 67 ± 10 64 NR Yes 5 Gallagher et al, 2007 85 ∗ Low risk (Goldman, Reilly criteria) 49 ± 11 53 NR No 1 Rubinshtein et al, 2007 58 Intermediate risk (ACC/AHA guideline risk groups) 56 ± 10 64 NR No 15 Johnson et al, 2008 109 Low to intermediate risk 63 ± 14 72 NR Yes 6 Takakuwa et al, 2008 197 Low to intermediate risk (TIMI) 49 ± 11 45 46 Yes 1 Ueno et al, 2009 36 Included some high risk 66 ± 12 53 NR No 1 Hollander et al, 2009 562 † Low risk (TIMI) 47 ± 9 44 26 No 1 Hoffman et al, 2009 368 Low to intermediate risk 53 ± 12 61 85 No 6 Hansen et al, 2010 89 Low to intermediate risk 56 ± 9 63 NR No 12
ACC, American College of Cardiology; ACS, acute coronary syndrome; AHA, American Heart Association; MACE, major adverse cardiac events; NR, not reported; TIMI, Thrombolysis in Myocardial Infarction risk scores.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Individual Study Results
Author True Positive True Negative False Positive False Negative Johnson et al, 2007 16 35 3 1 Gallagher et al, 2007 6 72 6 1 Rubinshtein et al, 2007 20 35 3 0 Johnson et al, 2008 13 96 0 0 Takakuwa et al, 2008 6 174 16 1 Ueno et al, 2009 11 20 4 1 Hollander et al, 2009 7 508 47 0 Hoffman et al, 2009 24 293 44 7 Hansen et al, 2010 3 85 1 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Qualitative Analysis
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. American Heart Association: Heart Disease and Stroke Statistics 2009 Update. Dallas; AHA: 2009. Statistics Committee and Stroke Statistics Subcommittee. Circulation 2009; 119: pp. 480-486.
2. Pitts S.R., Niska R.W., Xu J., et. al.: National Hospital Ambulatory Medical Care Survey: 2006 emergency department summary. Natl Health Stat Report 2008; 6: pp. 1-38.
3. Tosteson A.N., Goldman L., Udvarhelyi I.S., et. al.: Cost-effectiveness of a coronary care unit versus an intermediate care unit for emergency department patients with chest pain. Circulation 1996; 94: pp. 143-150.
4. Storrow A.B., Gibler W.B.: Chest pain centers: diagnosis of acute coronary syndromes. Ann Emerg Med 2000; 35: pp. 449-461.
5. Goldman L., Weinberg M., Weisberg M., et. al.: A computer-derived protocol to aid in the diagnosis of emergency room patients with acute chest pain. N Engl J Med 1982; 307: pp. 588-596.
6. Tatum J.L., Jesse R.L., Kontos M.C., et. al.: Comprehensive strategy for the evaluation and triage of the chest pain patient. Ann Emerg Med 1997; 29: pp. 116-125.
7. Selker H.P., Beshansky J.R., Griffith J.L., et. al.: Use of the acute cardiac ischemia time-insensitive predictive instrument (ACI-TIPI) to assist with triage of patients with chest pain or other symptoms suggestive of acute cardiac ischemia. Ann Intern Med 1998; 129: pp. 845-855.
8. Chase M., Robey J.L., Zogby K.E., et. al.: Prospective validation of the Thrombolysis in Myocardial Infarction Risk Score in the emergency department chest pain population. Ann Emerg Med 2006; 48: pp. 252-259.
9. Pope J.H., Aufderheide T.P., Ruthazer R., et. al.: Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med 2000; 342: pp. 1163-1170.
10. Schull M., Vermeulen M.J., Stukel T.A.: The risk of missed diagnosis of acute myocardial infarction associated with emergency department volume. Ann Emerg Med 2006; 48: pp. 647-655.
11. Leschka S., Alkadhi H., Plass A., et. al.: Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005; 26: pp. 1482-1487.
12. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
13. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
14. Fine J.J., Hopkins C.B., Ruff N., et. al.: Comparison of accuracy of 64-slice cardiovascular computed tomography with coronary angiography in patients with suspected coronary artery disease. Am J Cardiol 2006; 97: pp. 173-174.
15. Ehara M., Surmely J.F., Kawai M., et. al.: Diagnostic accuracy of 64-slice computed tomography for detecting angiographically significant coronary artery stenosis in an unselected consecutive patient population: comparison with conventional invasive angiography. Circ J 2006; 70: pp. 564-571.
16. Nikolaou K., Knez A., Rist C., et. al.: Accuracy of 64-MDCT in the diagnosis of ischemic heart disease. AJR Am J Roentgenol 2006; 187: pp. 111-117.
17. Schuijf J.D., Pundziute G., Jukema J.W., et. al.: Diagnostic accuracy of 64-slice multislice computed tomography in the noninvasive evaluation of significant coronary artery disease. Am J Cardiol 2006; 98: pp. 145-148.
18. Herzog C., Zwerner P.L., Doll J.R., et. al.: Significant coronary artery stenosis: comparison on per-patient and per-vessel or per-segment basis at 64-section CT angiography. Radiology 2007; 244: pp. 112-120.
19. Muhlenbruch G., Seyfarth T., Soo C.S., et. al.: Diagnostic value of 64-slice multi-detector row cardiac CTA in symptomatic patients. Eur Radiol 2007; 17: pp. 603-609.
20. Oncel D., Oncel G., Tastan A., et. al.: Detection of significant coronary artery stenosis with 64-section MDCT angiography. Eur J Radiol 2007; 62: pp. 394-405.
21. Shabestari A.A., Abdi S., Akhlaghpoor S., et. al.: Diagnostic performance of 64-channel multislice computed tomography in assessment of significant coronary artery disease in symptomatic subjects. Am J Cardiol 2007; 99: pp. 1656-1661.
22. Schlosser T., Mohrs O.K., Magedanz A., et. al.: Noninvasive coronary angiography using 64-detector-row computed tomography in patients with a low to moderate pretest probability of significant coronary artery disease. Acta Radiol 2007; 48: pp. 300-307.
23. Bayrak F., Guneysu T., Gemici G., et. al.: Diagnostic performance of 64-slice computed tomography coronary angiography to detect significant coronary artery stenosis. Acta Cardiol 2008; 63: pp. 11-17.
24. Miller J.M., Rochitte C.E., Dewey M., et. al.: Diagnostic performance of coronary angiography by 64-row CT. N Engl J Med 2008; 359: pp. 2324-2336.
25. Budoff M.J., Dowe D., Jollis J.G., et. al.: Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol 2008; 52: pp. 1724-1732.
26. Ulimoen G.R., Gjonnaess E., Atar D., et. al.: Noninvasive coronary angiography with 64-channel multidetector computed tomography in patients with acute coronary syndrome. Acta Radiol 2008; 10: pp. 1140-1144.
27. Rixe J., Rolf A., Conradi G., et. al.: Detection of relevant coronary artery disease using dual-source computed tomography in a high probability patient series: comparison with invasive angiography. Circ J 2009; 73: pp. 316-322.
28. Alessandri N., Di Matteo A., Rondoni G., et. al.: Heart imaging: the accuracy of the 64-MSCT in the detection of coronary artery disease. Eur Rev Med Pharmacol Sci 2009; 13: pp. 163-171.
29. Sheikh M., Ben-Nakhi A.M., Shukkur A.M., et. al.: Accuracy of 64-multidetector-row computed tomography in the diagnosis of coronary artery disease. Med Princ Pract 2009; 18: pp. 323-328.
30. Sosnowski M., Pysz P., Gola A., et. al.: Coronary artery visualization using a 64-row multi-slice computed tomography in unselected patients with definite or suspected coronary artery disease: a comparison with invasive coronary angiography. Cardiol J 2009; 16: pp. 413-417.
31. Selcoki Y., Yilmaz O.C., Kankilic M.N., et. al.: Diagnostic accuracy of 64-slice computed tomography in patients with suspected or proven coronary artery disease. Turk Kardiyol Dern Ars 2010; 38: pp. 95-100.
32. Tsiflikas I., Brodoefel H., Reimann A.J., et. al.: Coronary CT angiography with dual source computed tomography in 170 patients. Eur J Radiol 2010; 74: pp. 161-165.
33. Mowatt G., Cook J.A., Hillis G.S., et. al.: 64-Slice computed tomography angiography in the diagnosis and assessment of coronary artery disease: systematic review and meta-analysis. Heart 2008; 94: pp. 1386-1393.
34. Meijboom W.B., Meijs M.F.L., Schuijf J.D., et. al.: Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 2008; 52: pp. 2135-2144.
35. Abdulla J., Asferg C., Kofoed K.F.: Prognostic value of absence or presence of coronary artery disease determined by 64-slice computed tomography coronary angiography: a systematic review and meta-analysis. Int J Cardiovasc Imaging 2011; 27: pp. 413-420.
36. Papanicolaou M.N., Califf R.M., Hlatky M.A., et. al.: Prognostic implications of angiographically normal and insignificantly narrowed coronary arteries. Am J Cardiol 1986; 58: pp. 1181-1187.
37. Pitts W.R., Lange R.A., Cigarroa J.E., et. al.: Repeat coronary angiography in patients with chest pain and previously normal coronary angiogram. Am J Cardiol 1997; 80: pp. 1086-1087.
38. Moher D., Liberati A., Tetzlaff J., et. al., PRISMA Group: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009; 151: pp. 264-269.
39. Leeflang M.M.G., Deeks J.J., Gatsonis C., et. al.: Systematic reviews of diagnostic test accuracy. Ann Intern Med 2008; 149: pp. 889-897.
40. Chang S.A., Choi S.I., Choi E.K., et. al.: Usefulness of 64-slice multidetector computed tomography as an initial diagnostic approach in patients with acute chest pain. Am Heart J 2008; 156: pp. 375-383.
41. Hoffmann U., Nagurney J.T., Moselewski F., et. al.: Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006; 114: pp. 2251-2260.
42. Hollander J.E., Litt H.I., Chase M., et. al.: Computed tomography coronary angiography for rapid disposition of low-risk emergency department patients with chest pain syndromes. Acad Emerg Med 2007; 14: pp. 112-116.
43. Goldstein J.A., Gallagher M.J., O’Neill W.W., et. al.: A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol 2007; 49: pp. 863-871.
44. Deeks J.J., Macaskill P., Irwig L.: The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol 2005; 58: pp. 882-893.
45. Higgins J.P.T., Thompson S.G.: Quantifying heterogeneity in a meta-analysis. Stat Med 2002; 21: pp. 1539-1558.
46. Johnson T.R., Nikolaou K., Wintersperger B.J., et. al.: ECG-gated 64-MDCT angiography in the differential diagnosis of acute chest pain. AJR Am J Roentgenol 2007; 188: pp. 76-82.
47. Gallagher M.J., Ross M.A., Raff G.L., et. al.: The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann Emerg Med 2007; 49: pp. 125-136.
48. Rubinshtein R., Halon D.A., Gaspar T., et. al.: Usefulness of 64-slice cardiac computed tomographic angiography for diagnosing acute coronary syndromes and predicting clinical outcome in emergency department patients with chest pain of uncertain origin. Circulation 2007; 115: pp. 1762-1768.
49. Johnson T.R., Nikolaou K., Becker A., et. al.: Dual-source CT for chest pain assessment. Eur Radiol 2008; 18: pp. 773-780.
50. Takakuwa K.M., Halpern E.J.: Evaluation of a “triple rule-out” coronary CT angiography protocol: use of 64-section CT in low-to-moderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008; 248: pp. 438-446.
51. Ueno K., Anzai T., Jinzaki M., et. al.: Diagnostic capacity of 64-slice multidetector computed tomography for acute coronary syndrome in patients presenting with acute chest pain. Cardiology 2009; 112: pp. 211-218.
52. Hollander J.E., Chang A.M., Shofer F.S., et. al.: Coronary computed tomographic angiography for rapid discharge of low-risk patients with potential acute coronary syndromes. Ann Emerg Med 2009; 53: pp. 295-304.
53. Hoffmann U., Bamberg F., Chae C.U., et. al.: Coronary computed tomography angiography for early triage of patients with acute chest pain. J Am Coll Cardiol 2009; 53: pp. 1642-1650.
54. Hansen M., Ginns J., Seneviratne S., et. al.: The value of dual-source 64-slice CT coronary angiography in the assessment of patients presenting to an acute chest pain service. Heart Lung Circulation 2010; 19: pp. 213-218.
55. Gianrossi R., Detrano R., Mulvihill D., et. al.: Exercise-induced ST depression in the diagnosis of coronary artery disease. A meta-analysis. Circulation 1989; 80: pp. 87-98.
56. Fleischmann K.E., Hunink M.G., Kuntz K.M., et. al.: Exercise echocardiography or exercise SPECT imaging? A meta-analysis of diagnostic test performance. JAMA 1998; 280: pp. 913-920.
57. Klocke F.J., Baird M.G., Lorell B.H., et. al.: ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging). J Am Coll Cardiol 2003; 42: pp. 1318-1333.
58. van Houwelingen H.C., Arends L.R., Stijnen T.: Advanced methods in meta-analysis: multivariate approach and meta-regression. Stat Med 2002; 21: pp. 589-624.