
Rationale and Objectives
To evaluate whether the presence of facial photographs obtained at the point-of-care of portable radiography leads to increased detection of wrong-patient errors.
Materials and Methods
In this institutional review board–approved study, 166 radiograph–photograph combinations were obtained from 30 patients. Consecutive radiographs from the same patients resulted in 83 unique pairs (ie, a new radiograph and prior, comparison radiograph) for interpretation. To simulate wrong-patient errors, mismatched pairs were generated by pairing radiographs from different patients chosen randomly from the sample. Ninety radiologists each interpreted a unique randomly chosen set of 10 radiographic pairs, containing up to 10% mismatches (ie, error pairs). Radiologists were randomly assigned to interpret radiographs with or without photographs. The number of mismatches was identified, and interpretation times were recorded.
Results
Ninety radiologists with 21 ± 10 (mean ± standard deviation) years of experience were recruited to participate in this observer study. With the introduction of photographs, the proportion of errors detected increased from 31% (9 of 29) to 77% (23 of 30; P = .006). The odds ratio for detection of error with photographs to detection without photographs was 7.3 (95% confidence interval: 2.29–23.18). Observer qualifications, training, or practice in cardiothoracic radiology did not influence sensitivity for error detection. There is no significant difference in interpretation time for studies without photographs and those with photographs (60 ± 22 vs. 61 ± 25 seconds; P = .77).
Conclusions
In this observer study, facial photographs obtained simultaneously with portable chest radiographs increased the identification of any wrong-patient errors, without substantial increase in interpretation time. This technique offers a potential means to increase patient safety through correct patient identification.
The Institute of Medicine’s Quality Report estimates that nearly 98,000 deaths annually may be attributed to medical errors . Within radiology, an important source of error is the wrong-patient error , wherein one patient’s imaging study may be placed in another patient’s folder in a picture archiving and communication system (PACS). Such errors can create problems for both the involved patients. In fact, the National Quality Forum recognizes that wrong-patient errors can affect radiologic practice and that agency, along with the Agency for Healthcare Research and Quality, specifically endorses implementation of a “standardized protocol to prevent mislabeling of radiographs” .
Based on a statewide adverse event reporting system, the Pennsylvania Patient Safety Authority published that, in 2009, it received 652 reports on radiology events: 196 (30.1%) of these reported events were related to wrong-patient events. Of these 196 wrong-patient events, 93 (47%) occurred in the imaging modality of radiography. The report concluded that such errors “occur more frequently than health care providers and patients may realize” despite various quality improvement measures .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Acquisition and Case Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
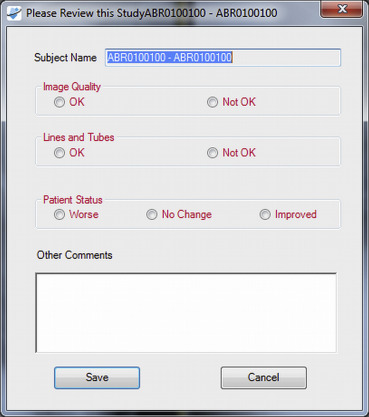
Display Workstation Environment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Observer Study Design
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Observer Characteristics
Get Radiology Tree app to read full this article<
Table 1
Observer Characteristics
Characteristic Value without Photos ( n = 45) Value with Photos ( n = 45) Total ( n = 90) Age (years) ∗ 53 ± 10 (35, 83) 53 ± 9 (37, 82) 53 ± 10 (35–83) Gender † Male 27 29 56 (62) Female 18 16 34 (38) Years postresidency training ∗ 22 ± 10(4, 52) 20 ± 10 (6, 50) 21 ± 10 (4–52) Fellowship training † Yes 38 38 76 (84) No 7 7 14 (16) Fellowship subspecialty † Abdominal 11 5 16 (18) Breast 2 4 6 (7) Cardiothoracic 7 9 16 (18) Interventional 5 5 10 (11) Musculoskeletal 2 5 7 (8) Neuroradiology 2 2 4 (4) Nuclear medicine 2 3 5 (6) Pediatric 4 5 9 (10) Other 3 1 4 (4) Not applicable 7 6 13 (14) Current subspecialty practice † Abdominal 11 6 17 (19) Breast 8 7 15 (17) Cardiothoracic 9 9 18 (20) Interventional 4 5 9 (10) Musculoskeletal 3 7 10 (11) Neuroradiology 2 2 4 (4) Nuclear Medicine 2 2 4 (4) Pediatric 3 6 9 (10) General radiology 3 1 4 (4)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
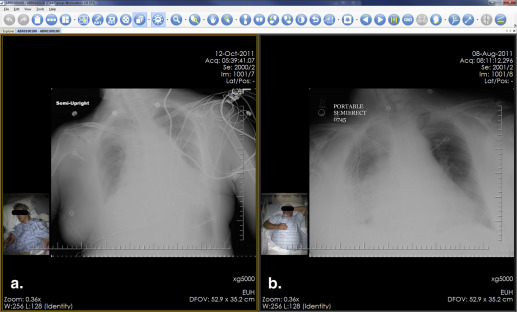
Qualitative Results Examples
Get Radiology Tree app to read full this article<
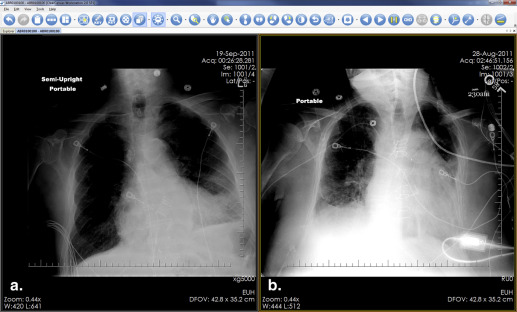
Get Radiology Tree app to read full this article<
Quantitative Results
Get Radiology Tree app to read full this article<
Table 2
Likelihood of Detecting a Wrong-patient Error: All Radiologists
Characteristic Without Photos With Photos Radiologists unexposed to wrong-patient error ( n = 31) 0/16 (0) 0/15 (0) Radiologists exposed to wrong-patient error ( n = 59) 9/29 (31) 23/30 (77)
Data are presented as ratio of errors detected to number of observers in each category and percent in parentheses.
Table 3
Likelihood of Detecting Wrong-patient Error by Radiologist Characteristics
Characteristic Without Photos Errors detected ∗ With Photos Errors Detected Odds Ratio † P Value ‡ Total readers ( n = 59) 9/29 (31) 23/30 (77) 7.30 (2.29–23.18) 0.006 Current subspecialty Cardiothoracic ( n = 12) 1/5 (20) 6/7 (86) 24 (1.14–505.19) 0.072 Noncardiothoracic ( n = 47) 8/24 (33) 17/23 (74) 5.67 (1.61–19.99) 0.008 Portable chest radiograph interpretation Specialties with current expertise in chest radiography ( n = 36) § 6/18 (33) 14/18 (78) 7 (1.5–30.80) 0.017 Specialties without current expertise in chest radiography ( n = 23) ‖ 3/11 (27) 9/12 (75) 8 (1.24–51.50) 0.039 Experience level >10 year postresidency ( n = 50) 8/25 (32) 20/25 (80) 8.5 (2.34–30.98) 0.014 ≤10 year postresidency ( n = 9) 1/4 (25) 3/5 (60) 4.5 (0.25–80.56) 0.524 Fellowship subspecialty Cardiothoracic ( n = 10) 1/3 (33) 7/10 (86) 12 (0.49–294.55) 0.183 Noncardiothoracic ( n = 49) 8/26 (31) 17/23 (74) 6.38 (1.83–22.23) 0.004 Fellowship trained Yes ( n = 51) 8/25 (32) 21/26 (81) 8.93 (2.46–32.33) 0.006 No ( n = 8) 1/4 (25) 2/4 (50) 3 (0.15–59.89) 1.000
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
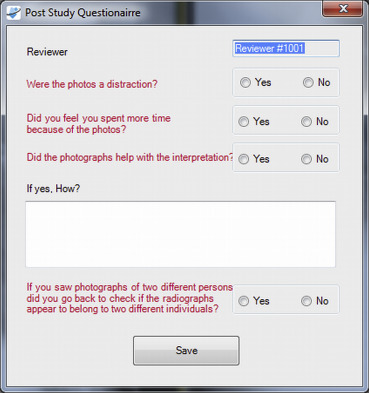
Poststudy Questionnaire
Get Radiology Tree app to read full this article<
Table 4
Results of Questionnaire That Observers Who Interpreted Studies with Photographs Completed at the End of Their Interpretation Session ∗
Question Response Yes No 1) Were the photographs a distraction? 8 (20) 31 (80) 2) Did you feel you spent more time because of the photographs? 18 (42) 25 (58) 3) Did the photographs help with the interpretation? 19 (44) 24 (56) 4) If you noted mismatched photographs, did you go back and check the radiographs? † 22 (96) 1 (4)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Relationship to Prior Studies
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Committee on Quality of Health Care in America, Institute of Medicine: To err is human: building a safer health system.1999.National Academy PressWashington, DC
2. National Quality Forum. 30 Safe practices for better health care fact sheet. Available at: http://www.ahrq.gov/qual/30safe.htm . Accessed June 23, 2012.
3. Pennsylvania Patient Safety Advisory: Applying the universal protocol to improve patient safety in radiology. Pennsylvania Patient Safety Authority 2011; 8: pp. 63-70.
4. Joint Commission on Accreditation of Healthcare Organizations 2012 National patient safety goals. Available at: http://www.jointcommission.org/assets/1/6/HAP_NPSG_Chapter_2014.pdf . Accessed May 26, 2014.
5. Ramamurthy S.P., Bhatti P., Arepalli C.D., et. al.: Integrating patient digital photographs with medical imaging examinations. Journal of Digital Imaging 2013; 26: pp. 875-885.
6. Tridandapani S, Provenzale J, Salama M, et al. Systems, methods and computer readable storage media storing instructions for generating an image series. U.S. Patent Application No. 2013/0177,222. July 11, 2013.
7. Tridandapani S., Ramamurthy S., Galgano S., et. al.: Increasing rate of detection of wrong patient radiographs: use of photographs obtained at the time of radiography. AJR Am J Roentgenol 2013; 200: pp. W345-W352.
8. Morishita J., Watanabe H., Katsuragawa S., et. al.: Investigation of misfiled cases in the PACS environment and a solution to prevent filing errors for chest radiographs. Acad Radiol 2005; 12: pp. 97-103.
9. Schultz S., Watson R., Prescott S., et. al.: Patient safety event reporting in a large radiology department. AJR Am J of Roentgenol 2011; 197: pp. 684-688.
10. Versel, N. Making the most of patient safety I.T. Health Data Management Magazine. Available at: http://www.healthdatamanagement.com/issues/19-8/making-the-most-of-patient-safety-i.t.-42891-1.html . Accessed February 25, 2014.Pubmed Partial Author STitle
11. Horowitz, B. Fingerprint biometrics allow hospitals to securely access e-prescriptions, EHRs. eWeek 2011. Available at: http://www.eweek.com/c/a/Health-Care-IT/Fingerprint-Biometrics-Allow-Hospitals-to-Securely-Access-ePrescriptions-EHRs-386667 . Accessed February 25, 2014.
12. Anderson H. Iris scans for patient ID. Healthcare Infosecurity 2010. Available at: http://www.healthcareinfosecurity.com/articles.php?art_id=2439 . Accessed February 25, 2014.
13. Brown C.L.: Health-care data protection and biometric authentication policies: comparative culture and technology acceptance in China and in the United States. Review of Policy Research 2012; 29: pp. 141-159.
14. Morishita J., Katsuragawa S., Konda K., et. al.: An automated patient recognition method based on an imaging matching technique using previous chest radiographs in the picture archiving and communication environment. Med Physics 2001; 28: pp. 1093-1097.
15. Kao E.-F., Lin W.-C., Jaw T.-S., et. al.: Automated patient identify recognition by analysis of chest radiograph features. Acad Radiol 2013; 20: pp. 1024-1031.
16. Turner Y., Hadas-Halpern I.: “The effects of including a patient’s photograph to the radiographic examination.”.Radiological Society of North America scientific assembly and annual meeting.2008.Radiological Society of North AmericaOak Brook, Ill:pp. 576.
17. Weiss F., Safdar N.: Do digital pictures add to the interpretation of diagnostic imaging: a survey along the spectrum of experience. AJR Am J Roentgenol 2010; 194: pp. A5.
18. Slasky B.S., Gur D., Good W.F., et. al.: Receiver operating characteristic analysis of chest image interpretation with conventional, laser-printed, and high-resolution workstation images. Radiology 1990; 174: pp. 775-780.