
Rationale and Objectives
To determine whether angled gantry acquisition might be used to image the heart with a shorter scan length and reduced breast exposure during coronary computed tomography angiography.
Materials and Methods
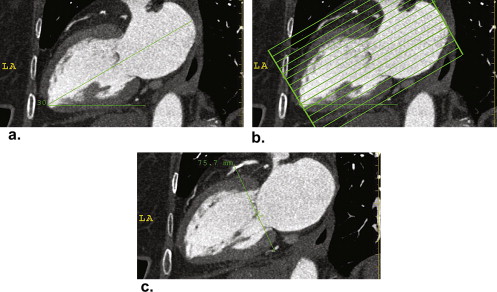
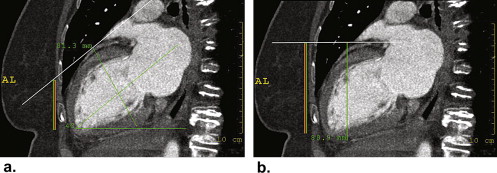
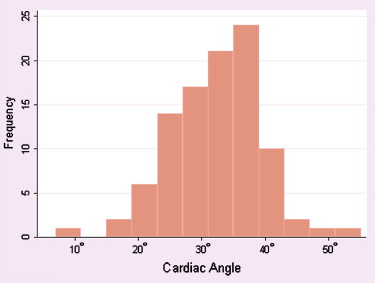
One hundred consecutive coronary computed tomography angiography examinations of female patients were retrospectively evaluated to define the angle between the long axis of the left heart and the axial imaging plane. The scan length required to image the entire left ventricle along with the coronary arteries was measured for an axial scan plane as well as for a scan plane parallel to the long axis of the left heart. The overlap between these imaging volumes and the lower portion of the breast was measured.
Results
The long axis of the left heart varied from 7° to 54° off the axial plane (mean 32° ± 7°). The required scan length to include the entire left ventricle and coronary arteries ranged from 8.2 to 12.4 cm (mean, 10.0 ± 0.9 cm) for the axial scan plane and 5.6–10.1 cm (mean, 7.5 ± 0.8 cm) for a scan plane parallel to the long axis of the heart ( P < .001). cCTA in the axial plane required a 7.4 ± 1.6 cm overlap with the lower breast, whereas cCTA in the long axis of the heart reduced the overlap to 4.5 ± 1.8 cm ( P < .001).
Conclusions
Using an angled gantry approach, the coronary arteries can be fully imaged in a plane along the long axis of the left heart with a single 10-cm acquisition and with substantial reduction in amount of breast tissue within the irradiated field.
Coronary computed tomography angiography (cCTA) demonstrates high sensitivity and specificity for the detection of coronary artery stenosis . An important obstacle to consistent high-quality coronary imaging is the beat to beat variability in cardiac rhythm. The latest generation of commercial computed tomography (CT) scanners includes a larger number of detector rings (256–320 slice scanners) that provide an extended z-axis acquisition during a single gantry rotation (8–16 cm). These scanners can image the entire coronary system in 1–2 heart beats, eliminating the degradation of image quality related to variability in heart rate .
After the limitations of image quality have been addressed, a remaining major limitation to the clinical application of cCTA is radiation dose . Of particular concern is the radiation dose to the breast of younger women, with an estimated lifetime attributable risk of cancer incidence of 0.7% for a 20-year-old woman receiving a standard cCTA without tube current modulation . Several strategies have been employed to reduce radiation dose, including breast shields , prospective electrocardiogram (ECG)-gated tube current modulation during helical acquisition and prospective ECG gating during axial image acquisition . These techniques reduce overall radiation exposure, but each includes the breast within the scan field of view.
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Scan Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Achenbach S.: Cardiac CT: state of the art for the detection of coronary arterial stenosis. J Cardiovasc Comput Tomogr 2007; 1: pp. 3-20.
2. Rybicki F.J., Otero H.J., Steigner M.L., et. al.: Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging 2008; 24: pp. 535-546.
3. Brenner D.J., Hall E.J.: Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
4. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
5. Parker M.S., Kelleher N.M., Hoots J.A., et. al.: Absorbed radiation dose of the female breast during diagnostic multidetector chest CT and dose reduction with a tungsten-antimony composite breast shield: preliminary results. Clin Radiol 2008; 63: pp. 278-288.
6. Vollmar S.V., Kalender W.A.: Reduction of dose to the female breast in thoracic CT: a comparison of standard-protocol, bismuth-shielded, partial and tube-current-modulated CT examinations. Eur Radiol 2008; 18: pp. 1674-1682.
7. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
8. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
9. Takakuwa KM, Halpern EJ, Gingold EL, et al. Radiation dose in a “triple rule-out” coronary CT angiography protocol of emergency department patients using 64-slice multidetector computed tomography: impact of scan parameters, prospective ECG-based tube current modulation, age, gender and body mass index. Am J Roentgenol AJR. In press.
10. Ketelsen D., Thomas C., Werner M., et. al.: Dual-source computed tomography: Estimation of radiation exposure of ECG-gated and ECG-triggered coronary angiography. Eur J Radiol 2008 Dec 17; [Epub ahead of print]
11. Earls J.P., Schrack E.C.: Prospectively gated low-dose CCTA: 24 months experience in more than 2,000 clinical cases. Int J Cardiovasc Imaging 2008 Nov 25; [Epub ahead of print]
12. International Commission on Radiological Protection: Relative biological effectiveness (RBE), quality factor (Q), and radiation weighting factor (Wr). ICRP Publication 92.2004.Elsevier Science LtdOxford, UK
13. Hsieh J.: Tomographic reconstruction for tilted helical multislice CT. IEEE Trans Med Imaging 2000; 19: pp. 864-872.
14. Noo F., Defrise M., Kudo H.: General reconstruction theory for multislice X-ray computed tomography with a gantry tilt. IEEE Trans Med Imaging 2004; 23: pp. 1109-1116.
15. Kachelriess M., Fuchs T., Schaller S., et. al.: Advanced single-slice rebinning for tilted spiral cone-beam CT. Med Phys 2001; 28: pp. 1033-1041.
16. Hein I., Taguchi K., Silver M.D., et. al.: Feldkamp-based cone-beam reconstruction for gantry-tilted helical multislice CT. Med Phys 2003; 30: pp. 3233-3242.
17. Morin R.L., Gerber T.C., McCollough C.H.: Radiation dose in computed tomography of the heart. Circulation 2003; 107: pp. 917-922.
18. Hunold P., Vogt F.M., Schmermund A., et. al.: Radiation exposure during cardiac CT: effective doses at multi-detector row CT and electron-beam CT. Radiology 2003; 226: pp. 145-152.