
Rationale and Objectives
Although studies have reported direct inhibition of inflammatory pathways with niacin, the effect of niacin on arterial wall inflammation remains unknown. We examined the effect of niacin on arterial 18 F-fluorodeoxyglucose (FDG)–positron emission tomography (PET)/computed tomography (CT).
Materials and Methods
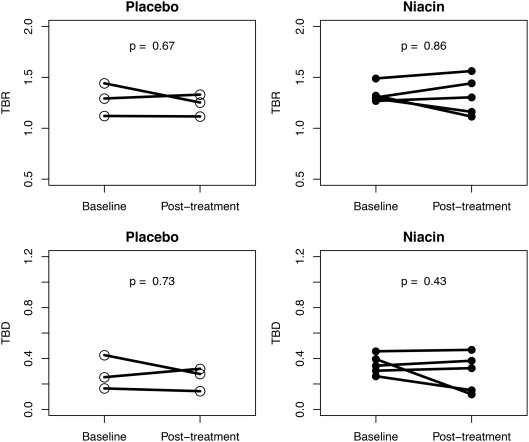
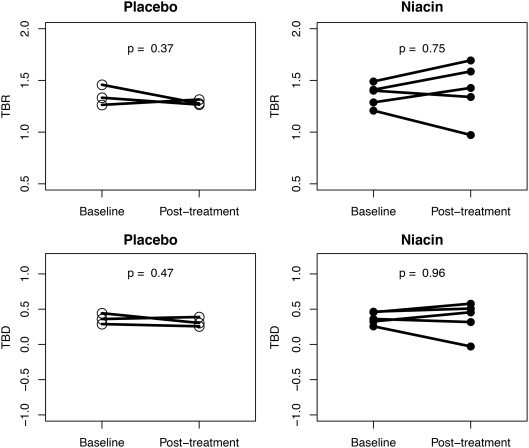
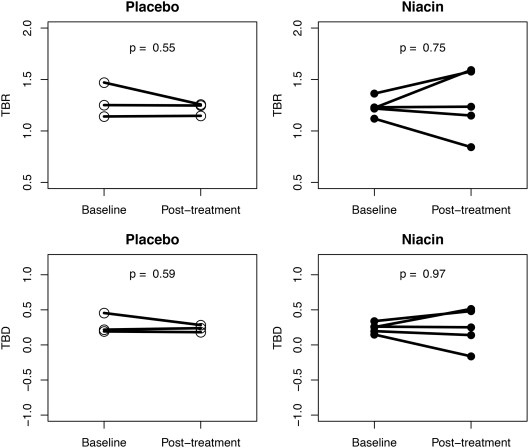
Nine statin-treated patients with coronary disease were randomized to niacin 6000 mg/day or placebo. FDG-PET/CT and lipids were assessed at baseline and at 12 weeks. FDG was quantified in the aorta, right carotid artery, and left carotid artery as the target-to-background ratio (TBR) and target-to-background difference (TBD).
Results
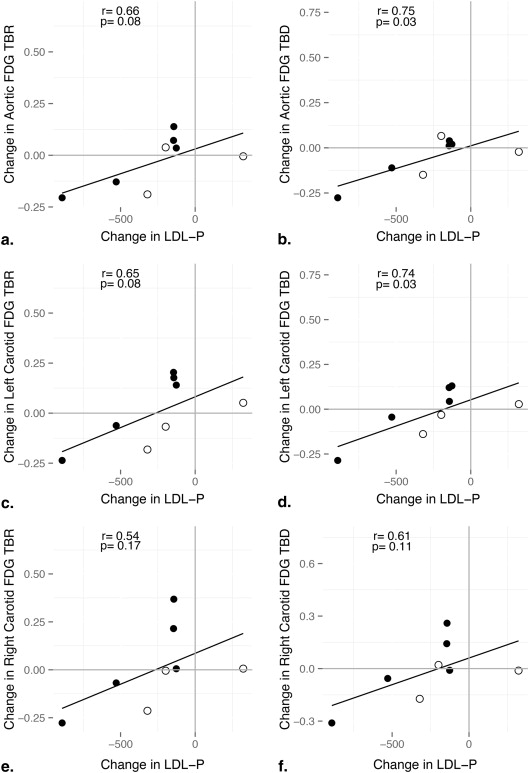
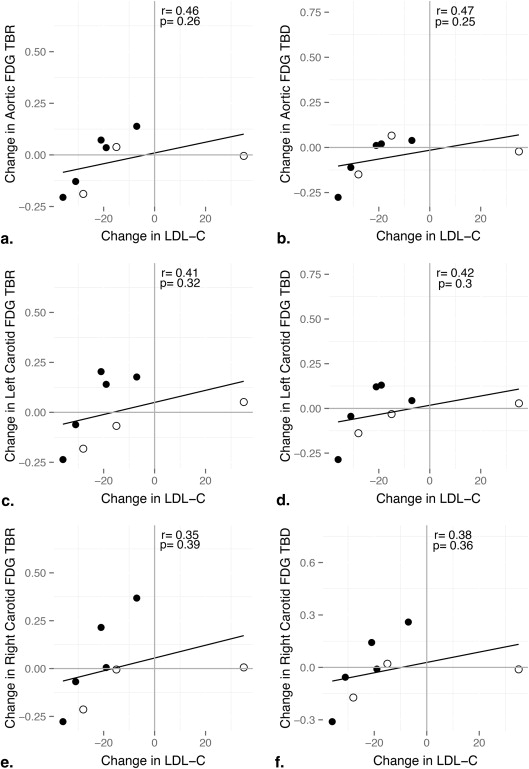
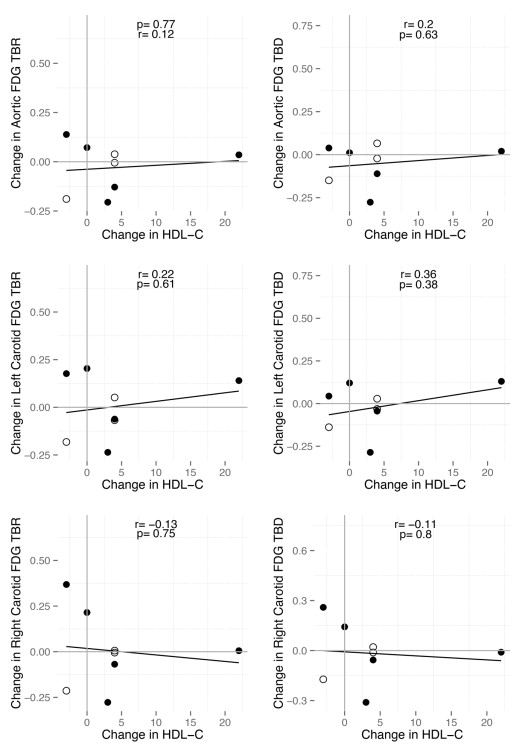
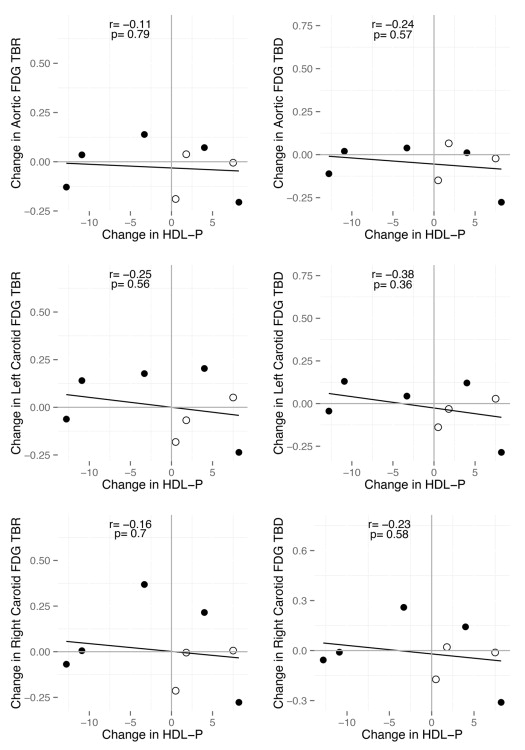
Eight patients completed the study. No significant changes in FDG measured by aortic, left carotid, or right carotid TBR or TBD were seen in either group. Compared to baseline, niacin-treated subjects exhibited a significant 29% reduction in low-density lipoprotein cholesterol (LDL-C; 95% confidence interval [CI], −50% to 8%; P = .01) and a nonsignificant 29% reduction in LDL particle number (LDL-P; 95% CI, −58% to 0.2%; P = .07). A nonsignificant 11% increase in HDL-C (95% CI, −15% to 37%; P = .30) and 8% decrease in HDL-P (95% CI, −44% to 28%; P = .51) were observed with niacin treatment. In a pooled analysis, changes in LDL-P were positively correlated with FDG uptake in the aorta (TBR r = 0.66, P = .08; TBD r = 0.75, P = .03), left carotid (TBR r = 0.65, P = .08; TBD r = 0.74, P = .03), and right carotid (TBR r = 0.54, P = .17; TBD r = 0.61, P = .11).
Conclusions
In this pilot study, adding niacin to statin therapy did not affect arterial wall inflammation measured by FDG-PET/CT. However, an association between changes in arterial FDG uptake and LDL-P was observed. Larger studies are needed to definitively examine the effect of niacin on arterial wall inflammation.
Despite over 50 years of use for the management of dyslipidemia , the potential role of niacin in the prevention of atherothrombotic disease and its mechanism of action remain uncertain. In two large randomized trials, AIM-HIGH and HPS2-THRIVE , niacin failed to achieve an incremental benefit in cardiovascular risk reduction when added to an aggressive low-density lipoprotein (LDL)–lowering approach with statin therapy. Independent of its effects on circulating lipids, niacin has more recently been shown to directly inhibit inflammation through activation of the G-protein–coupled receptor GPR109A . Therefore, we sought to characterize the effects of niacin on arterial wall inflammation using 18 F-fluorodeoxyglucose (FDG)–positron emission tomography (PET)/computed tomography (CT), an emerging imaging surrogate measure of atherosclerotic risk .
A growing body of evidence from clinical studies supports the utility of FDG-PET/CT imaging for the noninvasive characterization of atherosclerosis . Cross-sectional analyses initially performed in cancer patients demonstrated a consistent positive association between arterial FDG signal and traditional atherosclerotic risk factors including age , hypertension , and body mass index and a higher prevalence of cardiovascular disease among patients with increased vascular FDG uptake . Case–control studies of patients with clinically manifested atherosclerotic disease demonstrated more avid FDG uptake in arteries harboring atherosclerotic plaques compared to unaffected vessels and greater FDG signal among culprit plaques causing stroke or acute coronary syndrome compared to clinically silent plaque. Most recently, a prospective cohort study demonstrated significant improvement in risk prediction of incident cardiovascular events with incorporation of aortic FDG uptake into a model of traditional risk factors . Large studies, such as the Progression and Early detection of Subclinical Atherosclerosis study targeting enrollment of 4000 adults, are underway to further evaluate the potential incremental prognostic value of arterial FDG uptake above and beyond classical cardiovascular risk factors .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Design and Subjects
Get Radiology Tree app to read full this article<
Study Treatment
Get Radiology Tree app to read full this article<
Lipids, Lipoproteins, and Metabolic Assessment
Get Radiology Tree app to read full this article<
FDG-PET/CT Imaging
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Clinical Characteristics
Get Radiology Tree app to read full this article<
Lipids and Lipoproteins
Get Radiology Tree app to read full this article<
Table 1
Plasma Lipids and Lipoproteins
Placebo ( n = 3) Niacin ( n = 5) Baseline Posttreatment Baseline Posttreatment Total cholesterol (mg/dL) 150 (23) 150 (17) 164 (39) 132 (47) Triglycerides (mg/dL) 89 (31) 108 (55) 129 (43) 81 (28) HDL-C (mg/dL) 38 (2) 40 (4) 45 (5) 50 (12) LDL-C (mg/dL) 91 (13) 89 (24) 90 (40) 67 (40) ∗ LDL-P (nmol/L) 1403 (286) 1337 (305) 1315 (563) 948 (552) † HDL-P (μmol/L) 28 (6.3) 31 (2.9) 32 (3.2) 29 (7.4)
C, cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; P, particle number.
Differences between the two treatment groups were examined using the unpaired Student t test. No significant differences in posttreatment values were observed. Mean (standard deviation) are provided for placebo- and niacin-treated groups. The paired Student t test was performed for the comparison of the data before and after treatment for a given treatment group.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
FDG-PET/CT Imaging
Get Radiology Tree app to read full this article<
Table 2
Mean (Standard Deviation) of TBR and TBD in Placebo- and Niacin-Treated Groups
Vessel FDG Index Placebo Niacin Baseline 12 Weeks Change Baseline 12 Weeks Change Aorta TBR 1.28 (0.16) 1.23 (0.11) −0.05 (0.12) 1.33 (0.09) 1.32 (0.19) −0.02 (0.14) TBD 0.28 (0.13) 0.25 (0.09) −0.03 (0.11) 0.35 (0.08) 0.29 (0.15) −0.06 (0.13) Left carotid TBR 1.35 (0.10) 1.29 (0.03) −0.07 (0.12) 1.36 (0.11) 1.40 (0.28) 0.04 (0.19) TBD 0.36 (0.08) 0.32 (0.07) −0.05 (0.08) 0.37 (0.09) 0.37 (0.24) −0.01 (0.17) Right carotid TBR 1.29 (0.17) 1.22 (0.06) −0.07 (0.12) 1.23 (0.09) 1.28 (0.31) 0.05 (0.25) TBD 0.29 (0.14) 0.23 (0.05) −0.05 (0.10) 0.24 (0.07) 0.24 (0.28) 0.01 (0.22)
FDG, 18 F-fluorodeoxyglucose; TBD, target-to-background difference; TBR, target-to-background ratio.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Correlation Between Aortic, Left Carotid, and Right Carotid Indices of FDG Uptake
Vessel FDG Index_r__P_ Aorta versus left carotid TBR 0.90 <.01 TBD 0.87 <.01 Aorta versus right carotid TBR 0.92 <.01 TBD 0.86 <.01 Left versus right carotid TBR 0.90 <.01 TBD 0.82 .01
FDG, 18 F-fluorodeoxyglucose; TBD, target-to-background difference; TBR, target-to-background ratio.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Supplementary Tables 1–4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Carlson L.A.: Nicotinic acid: the broad-spectrum lipid drug. A 50th anniversary review. J Intern Med 2005; 258: pp. 94-114.
2. Boden W.E., Probstfield J.L., Anderson T., et. al.: Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med 2011; 365: pp. 2255-2267.
3. Landray M.J., Haynes R., Hopewell J.C., et. al.: Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med 2014; 371: pp. 203-212.
4. Digby J.E., Martinez F., Jefferson A., et. al.: Anti-inflammatory effects of nicotinic acid in human monocytes are mediated by GPR109A dependent mechanisms. Arterioscler Thromb Vasc Biol 2012; 32: pp. 669-676.
5. Lukasova M., Hanson J., Tunaru S., et. al.: Nicotinic acid (niacin): new lipid-independent mechanisms of action and therapeutic potentials. Trends Pharmacol Sci 2011; 32: pp. 700-707.
6. Rudd J.H., Myers K.S., Bansilal S., et. al.: (18)Fluorodeoxyglucose positron emission tomography imaging of atherosclerotic plaque inflammation is highly reproducible: implications for atherosclerosis therapy trials. J Am Coll Cardiol 2007; 50: pp. 892-896.
7. Hess S., Blomberg B.A., Zhu H.J., et. al.: The pivotal role of FDG-PET/CT in modern medicine. Acad Radiol 2014; 21: pp. 232-249.
8. Sheikine Y., Akram K.: FDG-PET imaging of atherosclerosis: do we know what we see?. Atherosclerosis 2010; 211: pp. 371-380.
9. Yun M., Yeh D., Araujo L.I., et. al.: F-18 FDG uptake in the large arteries: a new observation. Clin Nucl Med 2001; 26: pp. 314-319.
10. Yun M., Jang S., Cucchiara A., et. al.: 18F FDG uptake in the large arteries: a correlation study with the atherogenic risk factors. Semin Nucl Med 2002; 32: pp. 70-76.
11. Tahara N., Kai H., Yamagishi S., et. al.: Vascular inflammation evaluated by [18F]-fluorodeoxyglucose positron emission tomography is associated with the metabolic syndrome. J Am Coll Cardiol 2007; 49: pp. 1533-1539.
12. Paulmier B., Duet M., Khayat R., et. al.: Arterial wall uptake of fluorodeoxyglucose on PET imaging in stable cancer disease patients indicates higher risk for cardiovascular events. J Nucl Cardiol 2008; 15: pp. 209-217.
13. Williams G., Kolodny G.M.: Retrospective study of coronary uptake of 18F-fluorodeoxyglucose in association with calcification and coronary artery disease: a preliminary study. Nucl Med Commun 2009; 30: pp. 287-291.
14. Davies J.R., Rudd J.H., Fryer T.D., et. al.: Identification of culprit lesions after transient ischemic attack by combined 18F fluorodeoxyglucose positron-emission tomography and high-resolution magnetic resonance imaging. Stroke 2005; 36: pp. 2642-2647.
15. Rudd J.H., Warburton E.A., Fryer T.D., et. al.: Imaging atherosclerotic plaque inflammation with [18F]-fluorodeoxyglucose positron emission tomography. Circulation 2002; 105: pp. 2708-2711.
16. Kwee R.M., Truijman M.T., Mess W.H., et. al.: Potential of integrated [18F] fluorodeoxyglucose positron-emission tomography/CT in identifying vulnerable carotid plaques. Am J Neuroradiol 2011; 32: pp. 950-954.
17. Moustafa R.R., Izquierdo-Garcia D., Fryer T.D., et. al.: Carotid plaque inflammation is associated with cerebral microembolism in patients with recent transient ischemic attack or stroke: a pilot study. Circ Cardiovasc Imaging 2010; 3: pp. 536-541.
18. Rogers I.S., Nasir K., Figueroa A.L., et. al.: Feasibility of FDG imaging of the coronary arteries: comparison between acute coronary syndrome and stable angina. JACC Cardiovasc Imaging 2010; 3: pp. 388-397.
19. Figueroa A.L., Abdelbaky A., Truong Q.A., et. al.: Measurement of arterial activity on routine FDG PET/CT images improves prediction of risk of future CV events. JACC Cardiovasc Imaging 2013; 6: pp. 1250-1259.
20. Fernandez-Ortiz A., Jimenez-Borreguero L.J., Penalvo J.L., et. al.: The Progression and Early detection of Subclinical Atherosclerosis (PESA) study: rationale and design. Am Heart J 2013; 166: pp. 990-998.
21. Tawakol A., Fayad Z.A., Mogg R., et. al.: Intensification of statin therapy results in a rapid reduction in atherosclerotic inflammation: results of a multicenter fluorodeoxyglucose-positron emission tomography/computed tomography feasibility study. J Am Coll Cardiol 2013; 62: pp. 909-917.
22. Tahara N., Kai H., Ishibashi M., et. al.: Simvastatin attenuates plaque inflammation: evaluation by fluorodeoxyglucose positron emission tomography. J Am Coll Cardiol 2006; 48: pp. 1825-1831.
23. Fayad Z.A., Mani V., Woodward M., et. al.: Safety and efficacy of dalcetrapib on atherosclerotic disease using novel non-invasive multimodality imaging (dal-PLAQUE): a randomised clinical trial. Lancet 2011; 378: pp. 1547-1559.
24. Schwartz G.G., Olsson A.G., Abt M., et. al.: Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med 2012; 367: pp. 2089-2099.
25. Cholesterol Treatment Trialists C, Mihaylova B., Emberson J., Blackwell L., et. al.: The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012; 380: pp. 581-590.
26. Baigent C., Keech A., Kearney P.M., et. al.: Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet 2005; 366: pp. 1267-1278.
27. Kolodgie F.D., Virmani R., Burke A.P., et. al.: Pathologic assessment of the vulnerable human coronary plaque. Heart 2004; 90: pp. 1385-1391.
28. Tawakol A., Migrino R.Q., Bashian G.G., et. al.: In vivo 18F-fluorodeoxyglucose positron emission tomography imaging provides a noninvasive measure of carotid plaque inflammation in patients. J Am Coll Cardiol 2006; 48: pp. 1818-1824.
29. Davies JR, Izquierdo-Garcia D, Rudd JH et al. FDG-PET can distinguish inflamed from non-inflamed plaque in an animal model of atherosclerosis. Int J Cardiovasc Imaging;26:41–48.
30. Ogawa M., Ishino S., Mukai T., et. al.: (18)F-FDG accumulation in atherosclerotic plaques: immunohistochemical and PET imaging study. J Nucl Med 2004; 45: pp. 1245-1250.
31. Zhang Z., Machac J., Helft G., et. al.: Non-invasive imaging of atherosclerotic plaque macrophage in a rabbit model with F-18 FDG PET: a histopathological correlation. BMC Nucl Med 2006; 6: pp. 3.
32. Mackey R.H., Greenland P., Goff D.C., et. al.: High-density lipoprotein cholesterol and particle concentrations, carotid atherosclerosis, and coronary events: Results from the Multi-Ethnic Study of Atherosclerosis. J Am Coll Cardiol 2012; 60: pp. 508-516.
33. Jeyarajah E.J., Cromwell W.C., Otvos J.D.: Lipoprotein particle analysis by nuclear magnetic resonance spectroscopy. Clin Lab Med 2006; 26: pp. 847-870.
34. Rennick A., Kalakeche R., Seel L., et. al.: Nicotinic acid and nicotinamide: a review of their use for hyperphosphatemia in dialysis patients. Pharmacotherapy 2013; 33: pp. 683-690.
35. Mehta N.N., Torigian D.A., Gelfand J.M., et. al.: Quantification of atherosclerotic plaque activity and vascular inflammation using [18-F] fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT). J Vis Exp 2012; pp. e3777.
36. Bural G.G., Torigian D.A., Chamroonrat W., et. al.: Quantitative assessment of the atherosclerotic burden of the aorta by combined FDG-PET and CT image analysis: a new concept. Nucl Med Biol 2006; 33: pp. 1037-1043.
37. Digby J.E., Ruparelia N., Choudhury R.P.: Niacin in cardiovascular disease: recent preclinical and clinical developments. Arterioscler Thromb Vasc Biol 2012; 32: pp. 582-588.
38. O’Keefe J.H., Cordain L., Harris W.H., et. al.: Optimal low-density lipoprotein is 50 to 70 mg/dl: lower is better and physiologically normal. J Am Coll Cardiol 2004; 43: pp. 2142-2146.
39. Ference B.A., Yoo W., Alesh I., et. al.: Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease: a Mendelian randomization analysis. J Am Coll Cardiol 2012; 60: pp. 2631-2639.
40. Otvos J.D., Collins D., Freedman D.S., et. al.: Low-density lipoprotein and high-density lipoprotein particle subclasses predict coronary events and are favorably changed by gemfibrozil therapy in the Veterans Affairs High-Density Lipoprotein Intervention Trial. Circulation 2006; 113: pp. 1556-1563.
41. deGoma E.M., Davis M.D., Dunbar R.L., et. al.: Discordance between non-HDL-cholesterol and LDL-particle measurements: results from the Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2013; 229: pp. 517-523.
42. McKenney J.M., Proctor J.D., Harris S., et. al.: A comparison of the efficacy and toxic effects of sustained- vs immediate-release niacin in hypercholesterolemic patients. JAMA 1994; 271: pp. 672-677.
43. Airan-Javia S.L., Wolf R.L., Wolfe M.L., et. al.: Atheroprotective lipoprotein effects of a niacin–simvastatin combination compared to low- and high-dose simvastatin monotherapy. Am Heart J 2009; 157: 687.e1–8
44. Jafri H., Alsheikh-Ali A.A., Mooney P., et. al.: Extended-release niacin reduces LDL particle number without changing total LDL cholesterol in patients with stable CAD. J Clin Lipidol 2009; 3: pp. 45-50.
45. Hillis G.S., Pearson C.V., Harding S.A., et. al.: Effects of a brief course of azithromycin on soluble cell adhesion molecules and markers of inflammation in survivors of an acute coronary syndrome: a double-blind, randomized, placebo-controlled study. Am Heart J 2004; 148: pp. 72-79.
46. Kim W.H., Ko Y.G., Kang K.W., et. al.: Effects of combination therapy with celecoxib and doxycycline on neointimal hyperplasia and inflammatory biomarkers in coronary artery disease patients treated with bare metal stents. Yonsei Med J 2012; 53: pp. 68-75.
47. Grayston J.T., Kronmal R.A., Jackson L.A., et. al.: Azithromycin for the secondary prevention of coronary events. N Engl J Med 2005; 352: pp. 1637-1645.
48. O’Connor C.M., Dunne M.W., Pfeffer M.A., et. al.: Azithromycin for the secondary prevention of coronary heart disease events: the WIZARD study: a randomized controlled trial. JAMA 2003; 290: pp. 1459-1466.
49. Cannon C.P., Braunwald E., McCabe C.H., et. al.: Antibiotic treatment of Chlamydia pneumoniae after acute coronary syndrome. New Engl J Med 2005; 352: pp. 1646-1654.
50. HPS2-THRIVE Collaborative Group: Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med 2014; 371: pp. 203-212.
51. Clofibrate and niacin in coronary heart disease. JAMA 1975; 231: pp. 360-381.
52. Blankenhorn D.H., Nessim S.A., Johnson R.L., et. al.: Beneficial effects of combined colestipol-niacin therapy on coronary atherosclerosis and coronary venous bypass grafts. JAMA 1987; 257: pp. 3233-3240.
53. Brown G., Albers J.J., Fisher L.D., et. al.: Regression of coronary artery disease as a result of intensive lipid-lowering therapy in men with high levels of apolipoprotein B. N Engl J Med 1990; 323: pp. 1289-1298.
54. Brinton E.A.: Search and rescue for hypotheses surviving AIM-HIGH, the niacin therapy earthquake: still problematic after the primary publication. J Clin Lipidol 2012; 6: pp. 312-317.
55. Group HTC: HPS2-THRIVE randomized placebo-controlled trial in 25 673 high-risk patients of ER niacin/laropiprant: trial design, pre-specified muscle and liver outcomes, and reasons for stopping study treatment. Eur H J 2013; 34: pp. 1279-1291.
56. Muntendam P., McCall C., Sanz J., et. al., High-Risk Plaque I: The BioImage Study: novel approaches to risk assessment in the primary prevention of atherosclerotic cardiovascular disease—study design and objectives. Am Heart J 2010; 160: pp. 49-57.