
Rationale and Objectives
Infectious encephalitis is a relatively common cause of morbidity and mortality. Treatment of infectious encephalitis with antiviral medication can be highly effective when administered promptly. Clinical mimics of encephalitis arise from a broad range of pathologic processes, including toxic, metabolic, neoplastic, autoimmune, and cardiovascular etiologies. These mimics need to be rapidly differentiated from infectious encephalitis to appropriately manage the correct etiology; however, the many overlapping signs of these various entities present a challenge to accurate diagnosis. A systematic approach that considers both the clinical manifestations and the imaging findings of infectious encephalitis and its mimics can contribute to more accurate and timely diagnosis.
Materials and Methods
Following an institutional review board approval, a health insurance portability and accountability act (HIPAA)-compliant search of our institutional imaging database (teaching files) was conducted to generate a list of adult and pediatric patients who presented between January 1, 1995 and October 10, 2013 for imaging to evaluate possible cases of encephalitis. Pertinent medical records, including clinical notes as well as surgical and pathology reports, were reviewed and correlated with imaging findings. Clinical and imaging findings were combined to generate useful flowcharts designed to assist in distinguishing infectious encephalitis from its mimics. Key imaging features were reviewed and were placed in the context of the provided flowcharts.
Results
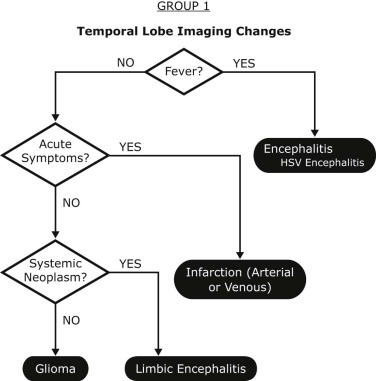
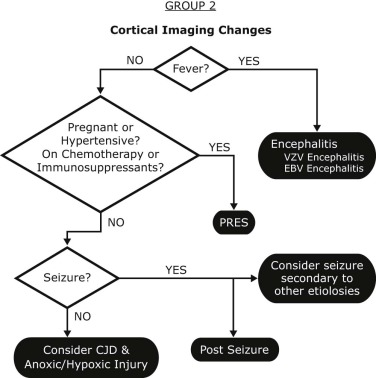
Four flowcharts were presented based on the primary anatomic site of imaging abnormality: group 1: temporal lobe; group 2: cerebral cortex; group 3: deep gray matter; and group 4: white matter. An approach that combines features on clinical presentation was then detailed. Imaging examples were used to demonstrate similarities and key differences.
Conclusions
Early recognition of infectious encephalitis is critical, but can be quite complex due to diverse pathologies and overlapping features. Synthesis of both the clinical and imaging features of infectious encephalitis and its mimics is critical to a timely and accurate diagnosis. The use of the flowcharts presented in this article can further enable both clinicians and radiologists to more confidently differentiate encephalitis from its mimics and improve patient care.
Introduction
Infectious encephalitis is a relatively common cause of morbidity and mortality. Herpes simplex virus (HSV) alone results in an estimated 2000 deaths per year in the United States . Treatment of infectious encephalitis with antiviral medication can be highly effective when administered promptly. This has been most clearly demonstrated in HSV encephalitis, with antiviral medication resulting in impressive reductions in mortality . Despite advances in treatment, the complexity of the imaging findings and clinical symptomatology associated with infectious encephalitis can result in delays in diagnosis and treatment, and consequently poor outcomes.
Clinical mimics of encephalitis arise from a broad range of pathologic processes, including toxic, metabolic, neoplastic, autoimmune, and cardiovascular etiologies. These distinct entities need to be rapidly differentiated from infectious encephalitis to appropriately manage their separate root causes. When combined, the imaging findings and the clinical symptomatology of both infectious encephalitis and its associated noninfectious mimics are often unique. Thus, assessment of imaging and clinical findings together can frequently reveal the appropriate diagnosis, often before laboratory results are available.
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results and Discussion
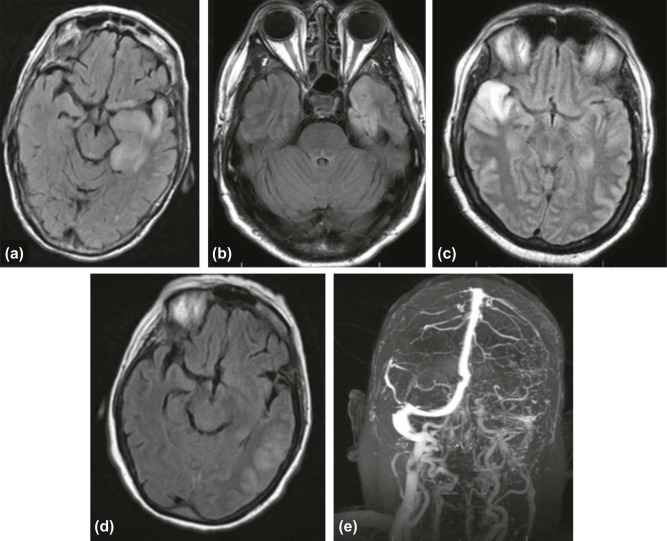
Group 1: Temporal Lobe Lesions
Herpes Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Infarction
Get Radiology Tree app to read full this article<
Primary Brain Tumors
Get Radiology Tree app to read full this article<
Limbic Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
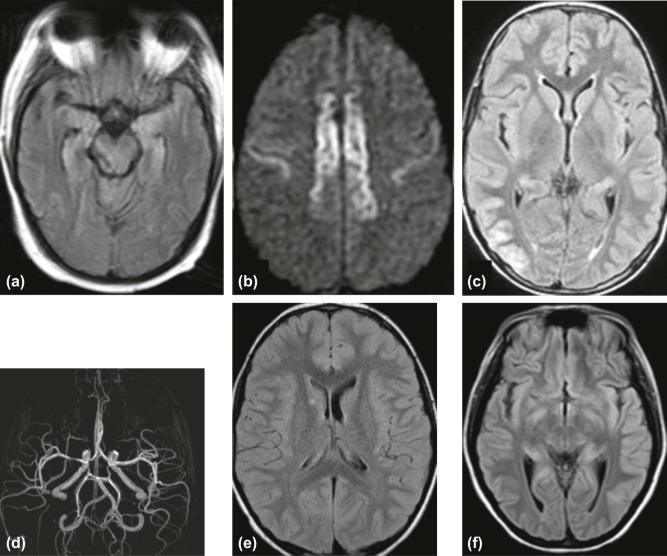
Group 2: Imaging Changes Centered on the Cerebral Cortex
Varicella Zoster Virus Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Epstein-Barr Virus Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Posterior Reversible Encephalopathy Syndrome
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Seizure
Get Radiology Tree app to read full this article<
Creutzfeldt-Jakob Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Group 3: Imaging Changes Centered on the Deep Gray Nuclei
West Nile Virus Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Rabies Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Toxic and Metabolic Abnormalities
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Group 4: Imaging Changes Centered on the White Matter
Human Immunodeficiency Virus Encephalitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acute Disseminated Encephalomyelitis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Lymphoma
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
 Open full size image
Open full size image
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Johnston R.T.: Viral infections of the central nervous system.2nd ed.1998.Lippincott-RavenPhiladelphia
2. Whitley R.J., Alford C.A., Hirsch M.S., et. al.: Vidarabine versus acyclovir therapy in herpes simplex encephalitis. N Engl J Med 1986; 314: pp. 144-149.
3. Skoldenberg B., Forsgren M., Alestig K., et. al.: Acyclovir versus vidarabine in herpes simplex encephalitis. Randomised multicentre study in consecutive Swedish patients. Lancet 1984; 2: pp. 707-711.
4. Fernandes A.F., Lange M.C., Novak F.T., et. al.: Extra-temporal involvement in herpes simplex encephalitis. J Clin Neurosci 2010; 17: pp. 1221-1223.
5. Akyildiz B.N., Gumus H., Kumandas S., et. al.: Diffusion-weighted magnetic resonance is better than polymerase chain reaction for early diagnosis of herpes simplex encephalitis—a case report. Pediatr Emerg Care 2008; 24: pp. 377-379.
6. Domingues R.B., Fink M.C., Tsanaclis A.M., et. al.: Diagnosis of herpes simplex encephalitis by magnetic resonance imaging and polymerase chain reaction assay of cerebrospinal fluid. J Neurol Sci 1998; 157: pp. 148-153.
7. Falcone S., Post M.J.: Encephalitis, cerebritis, and brain abscess: pathophysiology and imaging findings. Neuroimaging Clin N Am 2000; 10: pp. 333-353.
8. Obeid M., Franklin J., Shrestha S., et. al.: Diffusion-weighted imaging findings on MRI as the sole radiographic findings in a child with proven herpes simplex encephalitis. Pediatr Radiol 2007; 37: pp. 1159-1162.
9. Darnell R.B., Posner J.B.: Paraneoplastic syndromes involving the nervous system. N Engl J Med 2003; 349: pp. 1543-1554.
10. Gultekin S.H., Rosenfeld M.R., Voltz R., et. al.: Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings and tumour association in 50 patients. Brain 2000; 123: pp. 1481-1494.
11. Anderson N.E., Barber P.A.: Limbic encephalitis—a review. J Clin Neurosci 2008; 15: pp. 961-971.
12. Urbach H., Soeder B.M., Jeub M., et. al.: Serial MRI of limbic encephalitis. Neuroradiology 2006; 48: pp. 380-386.
13. Bien C.G., Urbach H., Schramm J., et. al.: Limbic encephalitis as a precipitating event in adult-onset temporal lobe epilepsy. Neurology 2007; 69: pp. 1236-1244.
14. Grahn A., Studahl M.: Varicella-zoster virus infections of the central nervous system—prognosis, diagnostics and treatment. J Infect 2015; 71: pp. 281-293.
15. Nagel M.A., Cohrs R.J., Mahalingam R., et. al.: The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features. Neurology 2008; 70: pp. 853-860.
16. Gilden D., Cohrs R.J., Mahalingam R., et. al.: Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment. Lancet Neurol 2009; 8: pp. 731-740.
17. Russman A.N., Lederman R.J., Calabrese L.H., et. al.: Multifocal varicella-zoster virus vasculopathy without rash. Arch Neurol 2003; 60: pp. 1607-1609.
18. Dunmire S.K., Hogquist K.A., Balfour H.H.: Infectious mononucleosis. Curr Top Microbiol Immunol 2015; 390: pp. 211-240.
19. Fujimoto H., Asaoka K., Imaizumi T., et. al.: Epstein-Barr virus infections of the central nervous system. Intern Med 2003; 42: pp. 33-40.
20. Hagemann G., Mentzel H.J., Weisser H., et. al.: Multiple reversible MR signal changes caused by Epstein-Barr virus encephalitis. AJNR Am J Neuroradiol 2006; 27: pp. 1447-1449.
21. Morris M.C., Edmunds W.J.: The changing epidemiology of infectious mononucleosis?. J Infect 2002; 45: pp. 107-109.
22. Shian W.J., Chi C.S.: Epstein-Barr virus encephalitis and encephalomyelitis: MR findings. Pediatr Radiol 1996; 26: pp. 690-693.
23. Hugonnet E., Da Ines D., Boby H., et. al.: Posterior reversible encephalopathy syndrome (PRES): features on CT and MR imaging. Diagn Interv Imaging 2013; 94: pp. 45-52.
24. Ni J., Zhou L.X., Hao H.L., et. al.: The clinical and radiological spectrum of posterior reversible encephalopathy syndrome: a retrospective series of 24 patients. J Neuroimaging 2011; 21: pp. 219-224.
25. Bartynski W.S., Boardman J.F.: Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome. AJNR Am J Neuroradiol 2007; 28: pp. 1320-1327.
26. Kim J.A., Chung J.I., Yoon P.H., et. al.: Transient MR signal changes in patients with generalized tonicoclonic seizure or status epilepticus: periictal diffusion-weighted imaging. AJNR Am J Neuroradiol 2001; 22: pp. 1149-1160.
27. Parmar H., Lim S.H., Tan N.C., et. al.: Acute symptomatic seizures and hippocampus damage: DWI and MRS findings. Neurology 2006; 66: pp. 1732-1735.
28. Johnson R.T., Gibbs C.J.: Creutzfeldt-Jakob disease and related transmissible spongiform encephalopathies. N Engl J Med 1998; 339: pp. 1994-2004.
29. Iwasaki Y., Mimuro M., Yoshida M., et. al.: Clinical diagnosis of Creutzfeldt-Jakob disease: accuracy based on analysis of autopsy-confirmed cases. J Neurol Sci 2009; 277: pp. 119-123.
30. Meissner B., Kallenberg K., Sanchez-Juan P., et. al.: MRI lesion profiles in sporadic Creutzfeldt-Jakob disease. Neurology 2009; 72: pp. 1994-2001.
31. Clarencon F., Gutman F., Giannesini C., et. al.: MRI and FDG PET/CT findings in a case of probable Heidenhain variant Creutzfeldt-Jakob disease. J Neuroradiol 2008; 35: pp. 240-243.
32. Collie D.A., Summers D.M., Sellar R.J., et. al.: Diagnosing variant Creutzfeldt-Jakob disease with the pulvinar sign: MR imaging findings in 86 neuropathologically confirmed cases. AJNR Am J Neuroradiol 2003; 24: pp. 1560-1569.
33. Heinemann U., Krasnianski A., Meissner B., et. al.: Brain biopsy in patients with suspected Creutzfeldt-Jakob disease. J Neurosurg 2008; 109: pp. 735-741.
34. Asnis D.S., Conetta R., Teixeira A.A., et. al.: The West Nile virus outbreak of 1999 in New York: the Flushing Hospital experience. Clin Infect Dis 2000; 30: pp. 413-418.
35. Hayes E.B., Gubler D.J.: West Nile virus: epidemiology and clinical features of an emerging epidemic in the United States. Annu Rev Med 2006; 57: pp. 181-194.
36. Petersen L.R., Brault A.C., Nasci R.S.: West Nile virus: review of the literature. JAMA 2013; 310: pp. 308-315.
37. Mostashari F., Bunning M.L., Kitsutani P.T., et. al.: Epidemic West Nile encephalitis, New York, 1999: results of a household-based seroepidemiological survey. Lancet 2001; 358: pp. 261-264.
38. Madden K.: West Nile virus infection and its neurological manifestations. Clin Med Res 2003; 1: pp. 145-150.
39. Petersen L.R., Marfin A.A.: West Nile virus: a primer for the clinician. Ann Intern Med 2002; 137: pp. 173-179.
40. Petropoulou K.A., Gordon S.M., Prayson R.A., et. al.: West Nile virus meningoencephalitis: MR imaging findings. AJNR Am J Neuroradiol 2005; 26: pp. 1986-1995.
41. Kraushaar G., Patel R., Stoneham G.W.: West Nile virus: a case report with flaccid paralysis and cervical spinal cord: MR imaging findings. AJNR Am J Neuroradiol 2005; 26: pp. 26-29.
42. Agid R., Ducreux D., Halliday W.C., et. al.: MR diffusion-weighted imaging in a case of West Nile virus encephalitis. Neurology 2003; 61: pp. 1821-1823.
43. Ali M., Safriel Y., Sohi J., et. al.: West Nile virus infection: MR imaging findings in the nervous system. AJNR Am J Neuroradiol 2005; 26: pp. 289-297.
44. Conomy J.P., Leibovitz A., McCombs W., et. al.: Airborne rabies encephalitis: demonstration of rabies virus in the human central nervous system. Neurology 1977; 27: pp. 67-69.
45. Houff S.A., Burton R.C., Wilson R.W., et. al.: Human-to-human transmission of rabies virus by corneal transplant. N Engl J Med 1979; 300: pp. 603-604.
46. Crowcroft N.S., Thampi N.: The prevention and management of rabies. BMJ 2015; 350: pp. g7827.
47. Noah D.L., Drenzek C.L., Smith J.S., et. al.: Epidemiology of human rabies in the United States, 1980 to 1996. Ann Intern Med 1998; 128: pp. 922-930.
48. Mrak R.E., Young L.: Rabies encephalitis in humans: pathology, pathogenesis and pathophysiology. J Neuropathol Exp Neurol 1994; 53: pp. 1-10.
49. Laothamatas J., Hemachudha T., Mitrabhakdi E., et. al.: MR imaging in human rabies. AJNR Am J Neuroradiol 2003; 24: pp. 1102-1109.
50. Awasthi M., Parmar H., Patankar T., et. al.: Imaging findings in rabies encephalitis. AJNR Am J Neuroradiol 2001; 22: pp. 677-680.
51. Levy R.M., Bredesen D.E., Rosenblum M.L.: Neurological manifestations of the acquired immunodeficiency syndrome (AIDS): experience at UCSF and review of the literature. J Neurosurg 1985; 62: pp. 475-495.
52. Smith A.B., Smirniotopoulos J.G., Rushing E.J.: From the archives of the AFIP: central nervous system infections associated with human immunodeficiency virus infection: radiologic-pathologic correlation. Radiographics 2008; 28: pp. 2033-2058.
53. Maschke M., Kastrup O., Esser S., et. al.: Incidence and prevalence of neurological disorders associated with HIV since the introduction of highly active antiretroviral therapy (HAART). J Neurol Neurosurg Psychiatry 2000; 69: pp. 376-380.
54. Wender M.: Acute disseminated encephalomyelitis (ADEM). J Neuroimmunol 2011; 231: pp. 92-99.
55. Tenembaum S., Chitnis T., Ness J., et. al.: Acute disseminated encephalomyelitis. Neurology 2007; 68: pp. S23-S36.
56. Lin C.H., Jeng J.S., Hsieh S.T., et. al.: Acute disseminated encephalomyelitis: a follow-up study in Taiwan. J Neurol Neurosurg Psychiatry 2007; 78: pp. 162-167.
57. Sonneville R., Klein I., de Broucker T., et. al.: Post-infectious encephalitis in adults: diagnosis and management. J Infect 2009; 58: pp. 321-328.
58. Sonneville R., Demeret S., Klein I., et. al.: Acute disseminated encephalomyelitis in the intensive care unit: clinical features and outcome of 20 adults. Intensive Care Med 2008; 34: pp. 528-532.
59. Toh C.H., Castillo M., Wong A.M., et. al.: Primary cerebral lymphoma and glioblastoma multiforme: differences in diffusion characteristics evaluated with diffusion tensor imaging. AJNR Am J Neuroradiol 2008; 29: pp. 471-475.