
Rationale and Objectives
The apprenticeship model for training of percutaneous liver biopsy has limitations, and costs of commercially available simulation models can be prohibitive. We created an inexpensive tissue phantom for liver biopsy simulation and evaluated the utility of this model for training radiology residents.
Materials and Methods
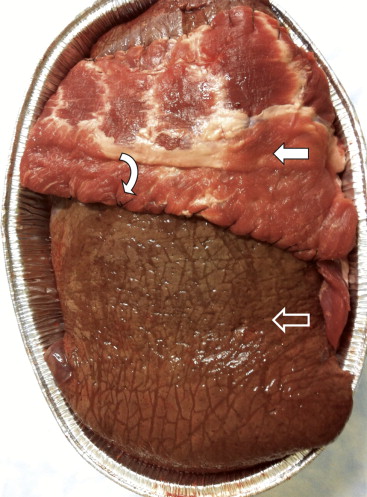
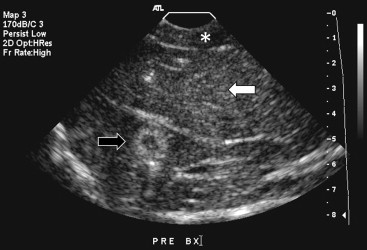
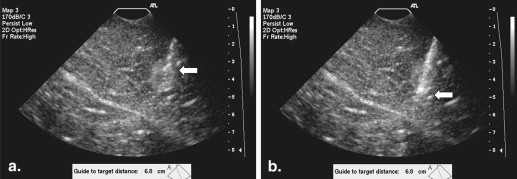
A bovine–porcine tissue phantom was devised as a simulation model and consisted of bovine liver with a porcine rib layer and inserted pimento olives simulating target lesions. Training sessions (a 20-minute didactic lecture and a 90-minute practice session) were offered to all residents in a diagnostic radiology residency. Effect of training was assessed by questionnaire before and after training. Level of knowledge of topics covered in the didactic session, confidence in technical skills, and anxiety level were evaluated on a five-point scale (1, poor to 5, excellent).
Results
Thirty-five of 38 residents received training on the models (∼$40). Mean reported value score for training was 4.88/5. Improvement was greatest for knowledge of technique (2.3–4.1/5, P < .001) and knowledge of postprocedure care (2.2–4.1/5, P < .001). Technical confidence increased (2.4–3.8/5, P < .001) and anxiety related to performing liver biopsy improved (2.7–3.7/5, P < .001). Residents with no prior experience in liver biopsy ( n = 21) had significantly greater increases in all categories than residents with prior experience ( n = 14), except for knowledge about obtaining informed consent and anxiety levels.
Conclusions
Utilization of an inexpensively created bovine/porcine liver biopsy simulation model was well perceived by radiology residents and can be used as an educational tool during residency.
Ultrasound guidance for procedures is a skill used in many radiology subspecialty areas, such as body imaging, interventional radiology, mammography, and musculoskeletal radiology. Proficiency with ultrasound-guided (US-guided) procedures should be a part of a radiology residency core curriculum.
Percutaneous liver biopsy is a commonly performed procedure for staging of diffuse liver disease and diagnosis of hepatic lesions; however, it does carry the risk of hemorrhage, biliary leak, injury to adjacent structures, and even death . Ultrasound guidance for nontargeted liver biopsy can significantly decrease complication rate from 2.1% for blinded liver biopsy to 0.53% for those with ultrasound guidance . Learning to perform liver biopsies under ultrasound guidance also provides a solid foundation for percutaneous interventions on other solid organs and is a necessary step before performing targeted liver biopsies.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Study Design
Get Radiology Tree app to read full this article<
Creation of a Bovine–Porcine Tissue Phantom
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Selection of Participants
Get Radiology Tree app to read full this article<
Training Sessions
Get Radiology Tree app to read full this article<
Table 1
Didactic Topics
Didactic lecture content (20 minutes) Indications for nontargeted and targeted biopsy Target selection Coagulation parameters Informed consent and specific risks of liver biopsy Considerations for pain control and/or conscious sedation Collaboration with nursing and pathology colleagues Technique: equipment setup, preliminary imaging and selection of an entry site, preprocedure time out, sterile technique, local anesthesia, breathing instructions, needle deployment, and sample handling Postprocedure care
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Survey Results
Get Radiology Tree app to read full this article<
Table 2
Survey Results
Survey Query Mean Preintervention Rating (Scale 1–5) Mean Postintervention Rating (Scale 1–5) Wilcoxon Signed Rank Test, P Value Indications 2.7 4.2 <.001 Informed consent 3.4 4.4 <.001 Target selection 2.3 4.0 <.001 Coagulation parameters 2.7 4.4 <.001 Local anesthesia 2.7 4.4 <.001 Technique 2.3 4.1 <.001 Postprocedure instructions 2.2 4.1 <.001 Technical confidence 2.4 3.8 <.001 Anxiety 2.7 3.7 <.001
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Appendix
Get Radiology Tree app to read full this article<
Appendix 1
Preintervention Survey
Item Number Query Response 1 In what year of training are you? PGY 2 PGY 3 PGY 4 PGY 5 2 How many ultrasound guided core biopsies of any abdominal organ have you performed? None 1–5 >5–10 >10–20 >20 3 How many liver biopsies have you performed? None 1–5 >5–10 >10–20 >20 4 How knowledgeable do you consider yourself regarding the following components of the procedure? (Rank from 1–5, 1 = no knowledge, 5 = extremely knowledgeable) Indications for liver biopsy 1 2 3 4 5 Informed consent 1 2 3 4 5 Feasibility of lesions/approach 1 2 3 4 5 Coagulation parameters 1 2 3 4 5 Local anesthesia and pain control 1 2 3 4 5 Technique 1 2 3 4 5 Postprocedure instructions 1 2 3 4 5 5 How confident are you in your technical skills? (Rank from 1–5: 1 = lack confidence, 5 = extremely confident) 1 2 3 4 5 6 How do you estimate your anxiety level prior to performing this procedure on a patient? (Rank from 1–5: 1 = extremely anxious, 5 = not anxious) 1 2 3 4 5
PGY, postgraduate year.
Appendix 2
Postintervention Survey
Item Number Query Response 1 How many liver biopsies did you perform on the phantom during the simulation? None 1–2 3–4 5–6 ≥7 2 How knowledgeable do you consider yourself regarding the following components of the procedure? (Rank from 1–5, 1 = no knowledge, 5 = extremely knowledgeable) Indications for liver biopsy 1 2 3 4 5 Informed consent 1 2 3 4 5 Feasibility of lesions/approach 1 2 3 4 5 Coagulation parameters 1 2 3 4 5 Local anesthesia and pain control 1 2 3 4 5 Technique 1 2 3 4 5 Postprocedure instructions 1 2 3 4 5 3 How confident are you in your technical skills? (Rank from 1–5: 1 = lack confidence, 5 = extremely confident) 1 2 3 4 5 4 How do you estimate your anxiety level prior to performing this procedure on a patient? (Rank from 1–5: 1 = extremely anxious, 5 = not anxious) 1 2 3 4 5 5 How helpful did you find the simulation training? (Rank from 1–2: 1 = not helpful, 5 = extremely helpful) 1 2 3 4 5 6 Any comments/suggestions?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bravo A.A., Sheth S.G., Chopra S.: Liver biopsy. N Engl J Med 2001; 344: pp. 495-500.
2. Rockey D.C., Caldwell S.H., Goodman Z.D., et. al.: AASLD position paper: liver biopsy. Hepatology 2009; 49: pp. 1017-1044.
3. Copel L., Sosna J., Kruskal J.B., et. al.: Ultrasound-guided percutaneous liver biopsy: indications, risk, and technique. Surg Technol Int 2003; 11: pp. 154-160.
4. Caturelli E., Giacobbe A., Facciorusso D., et. al.: Percutaneous biopsy in diffuse liver disease: increasing diagnostic yield and decreasing complication rate by routine ultrasound assessment of puncture site. Am J Gastroenterol 1996; 91: pp. 1318-1321.
5. Desser T.S.: Simulation-based training: the next revolution in radiology education?. JACR 2007; 4: pp. 816-824.
6. Dawson S.: Procedural simulation: a primer. Radiology 2006; 241: pp. 17-25.
7. Johnson S.J., Hunt C.M., Woolnough H.M., et. al.: Virtual reality, ultrasound-guided liver biopsy simulator: development and performance discrimination. Br J Radiol 2012; 85: pp. 555-561.
8. Scalese R.J., Obeso V.T., Issenberg S.B.: Simulation technology for skills training and competency assessment in medical education. J Gen Intern Med 2008; 23: pp. 46-49.
9. Desser T.S.: Simulation-based training: the next revolution in radiology education?. JACR 2007; 4: pp. 816-824.
10. Patel A.A., Gould D.A.: Simulators in interventional radiology training and evaluation: a paradigm shift IS on the horizon. JVIR 2006; 17: pp. S163-S173.
11. Harvey J.A., Morgan R.E., Hamer M.M., et. al.: Evaluation of a turkey-breast phantom for teaching freehand, US-guided core-needle breast biopsy. Acad Radiol 1997; 8: pp. 565-569.
12. Fischmann A., Siegmann K.C.: Low-cost phantoms for training of stereotactic vacuum-assisted biopsy of the breast. Clinical Imaging 2010; 34: pp. 97-99.
13. Larrison M., Di Bona A., Hogg D.: Low-cost phantom for stereotactic breast biopsy training. AJR 2006; 187: pp. 972-974.
14. Mendiratta-Lala M., Williams T., de Quadros N., et. al.: The use of a simulation center to improve resident proficiency in performing ultrasound-guided procedures. Acad Radiol 2010; 4: pp. 535-540.
15. Triple modality 3D abdominal phantom. Available at: http://www.cirsinc.com/products/modality/65/triple-modality-3d-abdominal-phantom/ . Accessed October 24, 2013.
16. Mrug M., Bissler J.J.: Simulation of real-time ultrasound-guided renal biopsy. Kidney International 2010; 78: pp. 705-707.
17. MCdougall E.M.: Validation of surgical simulators. J Endourol 2007; 21: pp. 244-247.
18. Rockey D.C.: Non-invasive assessment of liver fibrosis and portal hypertension with transient elastography. Gastroenterology 2008; 134: pp. 8-14.
19. Bari V.: Direct observation of procedural skills in radiology. AJR 2010; 195: pp. W14-W18.
20. Mendiratta-Lala M., Eisenberg R.L., Steele J.R., et. al.: Quality initiatives. Measuring and managing the procedural competency of radiologists. Radiographics 2011; 31: pp. 1477-1488.
21. Kneebone R., Kidd J., Nestel D., et. al.: An innovative model for teaching and learning clinical procedures. Med Educ 2002; 36: pp. 628-634.
22. Kneebone R., Nestel D., Yadollahi F., et. al.: Assessing procedural skills in context: exploring the feasibility of an Integrated Procedural Performance Instrument (IPPI). Med Educ 2006; 40: pp. 1105-1114.
23. Gaies M.G., Morris S.A., Hafler J.P., et. al.: Reforming procedural skills training for pediatric residents: a randomized, interventional trial. Pediatrics 2009; 124: 619–9