
Rationale and Objectives
Obscure gastrointestinal bleeding (OGIB) is the bleeding from the gastrointestinal tract without definite source that persists and recurs after a negative endoscopic evaluation. The study aimed to systematically evaluate the diagnostic accuracy of computed tomography enterography on OGIB detection by meta-analysis.
Materials and Methods
Studies were searched in relevant databases. With predefined inclusion criteria, eligible studies were included, followed by quality assessment using the Quality Assessment of Diagnostic Accuracy Studies scoring system. The Meta-DiSc software was used to implement the meta-analysis, and sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio with their 95% confidence intervals (CIs) were used as the effect size. Publication bias was determined by Egger test.
Results
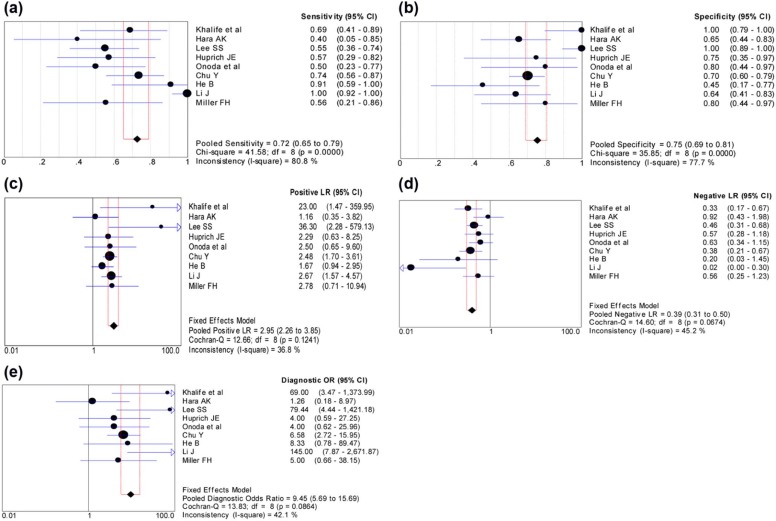
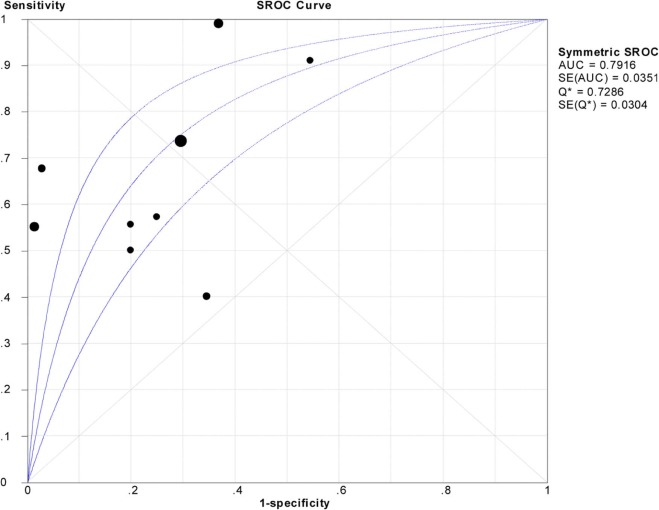
A set of nine studies was included in this meta-analysis, having a relatively high quality. Under the random effects model, the pooled sensitivity and specificity were 0.724 (95% CI: 0.651–0.789) and 0.752 (95% CI: 0.691–0.807), respectively. Under the fixed effects model, the pooled positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio were 2.949 (95% CI: 2.259–3.850), 0.393 (95% CI: 0.310–0.497), and 9.452 (95% CI: 5.693–15.692), respectively. The area under curve of the summary receiver operating characteristic curve was 0.7916 (95% CI: 0.723–0.860). No obvious publication bias was detected (t = 1.62, P = .181).
Conclusions
Computed tomography enterography might be used as a complementary to video capsule endoscopy instead of an alternative for the detection of OGIB.
Introduction
Gastrointestinal (GI) bleeding is a common clinical emergency. Annually, the incidence of GI bleeding is estimated about 150 per 100,000 persons, and the mortality is varied from 2% to 10% . Obscure GI bleeding (OGIB) is designated as the bleeding from the GI tract without definite source that persists and recurs after a negative endoscopic evaluation, and it accounts for nearly 5% of all GI hemorrhage cases . Based on whether the bleeding is visible or, OGIB is classified into two types as overt or occult bleeding .
With the standard endoscopic techniques, there is a huge challenge on diagnosis of patients with OGIB because it is hardly accessible to the jejunum and ileum . The video capsule endoscopy (VCE), a noninvasive diagnostic method for the entire small bowel, has been identified as the first-line evaluation tool for OGIB . Other advanced endoscopic methods like deep enteroscopy (eg, single-balloon enteroscopy, double-balloon enteroscopy, and spiral enteroscopy) have been developed for a better identification of the small bowel bleeding sites . Despite these improvements, the diagnostic results are undesirable, and the diagnostic yield of VCE is only 32%–83% . Meanwhile, VCE has its own limitations. For instance, its high sensitivity in occult bleeding might reduce the specificity. Additionally, the images of VCE tend to be obscured by blood, which could conceal the location of underlying lesion . Having the advantages of easy operation and extra evaluation on small bowel strictures, the computed tomography (CT) is often considered as a complementary of VCE . CT enterography (CTE) integrates the resolution of CT with the neutral oral contrast agents, which allows detailed visualization of the small intestines . For the diagnosis of potential small bowel bleeding, CTE, in combination with VCE, has a significantly greater sensitivity than VCE or CTE alone ( P < .05), but the sample size with 52 patients is relatively small . A meta-analysis has been published to evaluate the yield of CTE in evaluating OGIB, compared to CE, double-balloon enteroscopy, and digital subtraction angiography , and finds that CTE has a better diagnostic result than other alternate modalities in the evaluation of OGIB, especially of overt bleeding. However, detailed sensitivity and specificity of CTE have not been evaluated.
Get Radiology Tree app to read full this article<
Methods
Literature Search
Get Radiology Tree app to read full this article<
Inclusion and Exclusion Criteria
Get Radiology Tree app to read full this article<
Data Extraction and Quality Assessment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Eligible Studies and Their Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
Characteristics of the Included Studies
First Author Year Country Study Year Gender (M/F) Age (y) Channels Diagnostic Method Reference Standard TP FP FN TN QUADAS score Khalife et al 2011 France 2007.1–2009.8 19/13 55.9 ± 20.3 64 CTE Pathology, surgery, endoscopy 11 0 5 16 10 Hara AK 2009 USA 2006.6–2007.7 NA NA 16/64 CTE Pathology, endoscopy, angiography 2 9 3 17 9 Lee SS 2011 Korea 2005.8–2007.7 46/19 18–85 16/64 CTE Surgery, endoscopy, clinical follow-up 16 0 13 32 10 Huprich JE 2008 USA NA 11/11 37–83 64 CTE Surgery, conventional angiography, colonoscopy 8 2 6 6 9 Onoda et al 2010 Japan 2008.4–2009.7 NA NA 64 CTE Endoscopy 7 2 7 8 10 Chu Y 2016 China 2007.7–2014.7 60/61 51.1 ± 17.1 NA CTE Pathology 25 27 5 64 11 He B 2014 China 2008.5–2013.9 12/10 54.1 ± 19.1 64 CTE,CTA Double-balloon enteroscopy, digital subtraction angiography, intraoperative pathologic examination 10 6 1 5 9 Li J 2016 China 2011.2–2015.5 40/24 18–65 NA CTE Capsule endoscopy 42 8 0 14 8 Miller FH 2004 USA 1998.7–2011.11 NA NA NA CTE Angiography 5 2 4 8 10
CTA, computed tomography angiography; CTE, computed tomography enteroclysis; FN, false negatives; FP, false positives; M/F, male/female; NA, not available; QUADAS, quality assessment tool of diagnostic accuracy studies; TN, true negatives; TP, true positives.
Get Radiology Tree app to read full this article<
Pooled Effect Size of the Diagnostic Indicators
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Publication Bias
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Kärkkäinen J.M., Miilunpohja S., Rantanen T., et. al.: Alcohol abuse increases rebleeding risk and mortality in patients with non-variceal upper gastrointestinal bleeding. Dig Dis Sci 2015; 60: pp. 3707-3715.
2. Ohmiya N., Nakagawa Y., Nagasaka M., et. al.: Obscure gastrointestinal bleeding: diagnosis and treatment. Dig Endosc 2015; 27: pp. 285-294.
3. Leung W.K., Ho S.S., Suen B.Y., et. al.: Capsule endoscopy or angiography in patients with acute overt obscure gastrointestinal bleeding: a prospective randomized study with long-term follow-up. Am J Gastroenterol 2012; 107: pp. 1370-1376.
4. Bonnet S., Douard R., Malamut G., et. al.: Intraoperative enteroscopy in the management of obscure gastrointestinal bleeding. Dig Liver Dis 2013; 45: pp. 277-284.
5. Min Y.W., Kim J.S., Jeon S.W., et. al.: Long-term outcome of capsule endoscopy in obscure gastrointestinal bleeding: a nationwide analysis. Endoscopy 2014; 46: pp. 59-65.
6. Sidhu R., Sanders D.S.: Double-balloon enteroscopy in the elderly with obscure gastrointestinal bleeding: safety and feasibility. Eur J Gastroenterol Hepatol 2013; 25: pp. 1230-1234.
7. Pintopais T., Pinho R., Rodrigues A., et. al.: Emergency single-balloon enteroscopy in overt obscure gastrointestinal bleeding: efficacy and safety. United European Gastroenterol J 2014; 2: pp. 490-496.
8. Agrawal J.R., Travis A.C., Mortele K.J., et. al.: Diagnostic yield of dual-phase computed tomography enterography in patients with obscure gastrointestinal bleeding and a non-diagnostic capsule endoscopy. J Gastroenterol Hepatol 2012; 27: pp. 751-759.
9. Jeon S.R., Jinoh K., Gun K.H., et. al.: Is there a difference between capsule endoscopy and computed tomography as a first-line study in obscure gastrointestinal bleeding?. Turk J Gastroenterol 2014; 25: pp. 257-263.
10. Limsrivilai J., Srisajjakul S., Pongprasobchai S., et. al.: A prospective blinded comparison of video capsule endoscopy versus computed tomography enterography in potential small bowel bleeding: clinical utility of computed tomography enterography. J Clin Gastroenterol 2017;
11. Wang Z., Chen J.Q., Liu J.L., et. al.: CT enterography in obscure gastrointestinal bleeding: a systematic review and meta-analysis. J Med Imaging Radiat Oncol 2013; 57: pp. 263-273.
12. Whiting P., Rutjes A.W., Reitsma J.B., et. al.: The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003; 3: pp. 25.
13. Mocellin S., Marchet A., Nitti D.: EUS for the staging of gastric cancer: a meta-analysis. Gastrointest Endosc 2011; 73: pp. 1122-1134.
14. Zamora J., Abraira V., Muriel A., et. al.: Meta-DiSc: a software for meta-analysis of test accuracy data. BMC Med Res Methodol 2006; 6: pp. 31.
15. Chu Y., Wu S., Qian Y., et. al.: Complimentary imaging modalities for investigating obscure gastrointestinal bleeding: capsule endoscopy, double-balloon enteroscopy, and computed tomographic enterography. Gastroenterol Res Pract 2016; 2016: pp. 1-8.
16. Hara A.K., Walker F.B., Silva A.C., et. al.: Preliminary estimate of triphasic CT enterography performance in hemodynamically stable patients with suspected gastrointestinal bleeding. AJR Am J Roentgenol 2012; 193: pp. 1252-1260.
17. He B., Gong S., Hu C., et. al.: Obscure gastrointestinal bleeding: diagnostic performance of 64-section multiphase CT enterography and CT angiography compared with capsule endoscopy. Br J Radiol 2014; 87: pp. 20140229.
18. Huprich J.E., Fletcher J.G., Alexander J.A., et. al.: Obscure gastrointestinal bleeding: evaluation with 64-section multiphase CT enterography—initial experience. Radiology 2008; 246: pp. 562-571.
19. Khalife S., Soyer P., Alatawi A., et. al.: Obscure gastrointestinal bleeding: preliminary comparison of 64-section CT enteroclysis with video capsule endoscopy. Eur Radiol 2011; 21: pp. 79-86.
20. Lee S.S., Oh T.S., Kim H.J., et. al.: Obscure gastrointestinal bleeding: diagnostic performance of multidetector CT enterography. Radiology 2011; 259: pp. 739-748.
21. Miller F.H., Hwang C.M.: An initial experience: using helical CT imaging to detect obscure gastrointestinal bleeding. Clin Imaging 2004; 28: pp. 245-251.
22. Onoda H., Shimizu K., Washida Y., et. al.: Usefulness of computed tomography enteroclysis in the intestinal tract. Jpn J R 2010; 28: pp. 193-198.
23. Li J., Li X., Han P., et. al.: MSCT enterography as a diagnostic tool in the evaluation of obscure gastrointestinal bleeding. J Clin Radiol 2016; 35: pp. 750-753.
24. Guo R., Cai L., Fan Y., et. al.: Magnetic resonance imaging on disease reclassification among active surveillance candidates with low-risk prostate cancer: a diagnostic meta-analysis. Prostate Cancer Prostatic Dis 2015; 18:
25. Solem C.A., Loftus E.V., Fletcher J.G., et. al.: Small-bowel imaging in Crohn’s disease: a prospective, blinded, 4-way comparison trial. Gastrointest Endosc 2008; 68: pp. 255-266.
26. Bruining D.H., Siddiki H.A., Fletcher J.G., et. al.: Benefit of computed tomography enterography in Crohn’s disease: effects on patient management and physician level of confidence. Inflamm Bowel Dis 2012; 18: pp. 219-225.
27. Qiu Y., Mao R., Chen B.L., et. al.: Systematic review with meta-analysis: magnetic resonance enterography vs. computed tomography enterography for evaluating disease activity in small bowel Crohn’s disease. Aliment Pharmacol Ther 2014; 40: pp. 134-146.
28. Pasha S.F., Hara A.K., Leighton J.A.: Diagnostic evaluation and management of obscure gastrointestinal bleeding: a changing paradigm. Gastroenterol Hepatol 2009; 5: pp. 839-850.
29. Santhakumar C.: Evaluation and outcomes of patients with obscure gastrointestinal bleeding. World J Gastrointest Pathophysiol 2014; 5: pp. 479-486.
30. Limsrivilai J., Pongprasobchai S., Srisajjakul S., et. al.: 334 a prospective blinded comparison of video capsule endoscopy versus computed tomography enterography in obscure gastrointestinal bleeding: appropriate position of computed tomography enterography. Gastrointest Endosc 2015; 81: pp. AB137.