
Rationale and Objectives
Accuracy of ultrasound-guided biopsy and Gleason score is limited, and diagnosis of insignificant cancer with Gleason score ≤6 is frequent when extended biopsy schemes are used. We evaluated whether the magnetic resonance imaging (MRI)-targeted in-bore prostate biopsy correctly identifies the Gleason score of prostate cancer in histopathologic correlation after prostatectomy. Simultaneously a targeted concept is expected to keep down the rate of insignificant cancer.
Materials and Methods
We compared retrospectively the Gleason score of the MRI-targeted in-bore biopsy with prostatectomy specimens in 50 men with prostate cancer. Endorectal MRI included T2-weighted imaging, diffusion-weighted imaging, dynamic contrast-enhanced imaging, and spectroscopy. Lesions with a prostate imaging–reporting and data system (PI-RADS) score ≥3 were considered. Upgrading and downgrading of tumors was evaluated, and significant upgrading was defined as a shift in Gleason score from 6 to 7 or more.
Results
Gleason score was concordant in 66% of the patients, overall upgraded in 30% of patients, and downgraded in 4% of patients. Significant upgrading of the Gleason score from 6 to 7 occurred in eight patients; upgrading did not exceed one step in the Gleason score. After prostatectomy the Gleason score 6 was found in 20% of patients. The median number of cores obtained was 4 (range 2–6), and the median number of positive cores was 2 (range 1–4).
Conclusions
In-bore MRI-targeted biopsy offers good accuracy in the Gleason score with postprostatectomy histopathologic control when compared to the literature. A limited number of cores are sufficient to achieve these results. The fraction of insignificant cancer identified by targeted only-biopsy is low. Upgrading is restricted to one step in the Gleason score. Clinicians should be aware of positive findings in MRI and the biopsy technique used when assessing prostate biopsy results.
Prostate cancer has become the most common cancer among men. Widespread use of prostate-specific antigen (PSA) screening has led to an increasing number of diagnoses and at the same time to an increasing detection rate of insignificant cancer. Prediction of cancer significance is predominantly based on the Gleason score. According to the Consensus Conference on Gleason grading, the Gleason score combines the most frequent and the highest Gleason grade in biopsy and the most frequent and second most frequent Gleason grade in prostatectomy specimens .
Now there are alternative treatment options to radical prostatectomy (RP) such as radiation therapy or active surveillance. Appropriate treatment depends on preoperative tumor grading in biopsy specimens.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
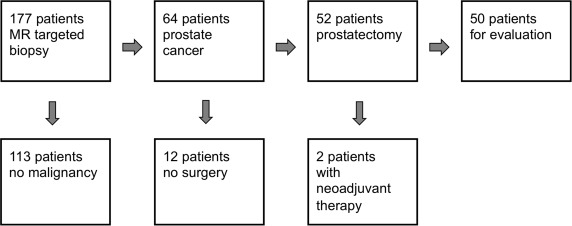
Get Radiology Tree app to read full this article<
Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Biopsy
Get Radiology Tree app to read full this article<

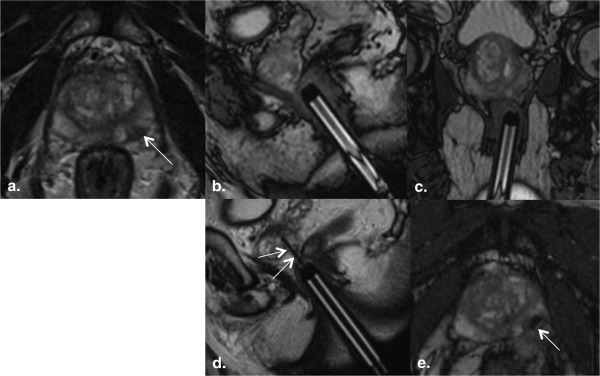
Table 1
MRI Protocol for MR-Targeted In-bore Prostate Biopsy
Objective Sequence Plane TR/TE (msec) Slice Thickness (mm) Matrix FOV (mm) Voxel Size (mm) Flip Angle Acquisitions PAT Time of Acquisition Planning of slice orientation trueFISP Axial, coronal, sagittal 4.2/2.1 msec 3.5 256 × 256 400 × 400 1.6 × 1.6 × 3.5 57 1 2 45 seconds Define landmarks ( Fig 4 a) T2-weighted TSE Axial 4930/100 3 205 × 256 200 × 200 1.0 × 0.8 × 3.0 1 1:53 minutes Navigation of needle holder ( Fig 4 b and c) trueFISP Sagittal and coronal 4.2/2.1 3.5 256 × 256 400 × 400 1.6 × 1.6 × 1.6 × 3.5 57 1 2 27 seconds Control of needle position ( Fig 4 d) BLADE Sagittal 4260/138 3 320 × 320 420 × 420 1.3 × 1.3 × 3 148 1 2 34 seconds Control of needle position ( Fig 4 e) trueFISP Axial 4.5/2.3 3.5 384 × 384 400 × 400 1.0 × 1.0 × 3.5 57 2 2 39 seconds
BLADE, proprietary name for periodically rotated overlapping parallel lines with enhanced reconstruction; FOV, field of view; MRI, magnetic resonance imaging; PAT, parallel imaging technique; TE, echo time; TR, repetition time; trueFISP, true fast imaging with steady-state precession; TSE, turbo spin echo.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Patient Characteristics
Variable Mean Median Range Age (years) 66 66 47–80 PSA (ng/mL) 10.79 8 3.03–38.8 Prostate volume (mL) 40.5 36.5 20–79 PSA density (ng/mL 2 ) 0.28 0.24 0.09–0.9 Time between biopsy and surgery (days) 39.78 38.5 12–106 Biopsy cores obtained per patient 3.96 4 2–6 Cores with tumor per patient 2.4 2 1–4 Tumor length per core (mm) 4.47 4 0.3–15 Tumor percentage per core (%) 39.8 33 3–100
PSA, prostate-specific antigen.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Distribution of Biopsy and Prostatectomy Gleason Grades
Biopsy Grades Prostatectomy Grades (% of Biopsy Grades) Total 5 6 7 8 9 6 1 (6%)9 (50%) 8 (44%) — — 18 7 — —19 (79%) 5 (21%) — 24 8 — — 1 (20%)2 (40%) 2 (40%) 5 9 — — — —3 (100%) 3 Total 1 9 28 7 5 50
Concordant Gleason scores are set in bold.
Get Radiology Tree app to read full this article<
Discussion
Overall Accuracy
Get Radiology Tree app to read full this article<
Table 4
Data Published for an Accuracy of Gleason Score in Prostate Biopsy
Study_n_ Patients Time Period Biopsy Technique Number of Cores Obtained Accuracy Upgrading Significant Upgrading (Gleason Score 6 to >7 or More) Downgrading Prevalence of Gleason score ≤6 Capitanio et al. 301
Only Gleason score ≤6 2001–2007 TRUS 18 (Median) — — 32% — — Chun et al. 2982 1992–2004 TRUS 6–12 56% 29% 37% 14% 47% Chung et al. 247 2006–2011 TRUS ≥12 57% 35% 42% 8% 30% Cohen et al. own data 2890 1982–2007 TRUS — 58% 36% 46% 5% 40% Cohen et al. meta-analysis 14,839 1973–2007 TRUS — 63% 30% 38% 7% 47% Corcoran et al. 1629 1995–2010 TRUS 8 (Median) 62% 29% 41% 10% 17% Corcoran et al. 684
Only Gleason score 6, 7 2003–2008 TRUS 10, 3–30 (Median, range) — — 67% — — Divrik et al. 206 1998–2005 TRUS 11, 10–14 (Median, range) 57% 34% — 10% 50% 186 1998–2005 TRUS 6–9 (Sextant biopsy) 41% 38% — 22% 46% Epstein et al. 7643 2002–2010 TRUS ≥10 73% ∗ 19% ∗ 36% 8% ∗ 50% Fanning et al. 206 2003–2008 TRUS ≥12 52% ∗ 36% ∗ 52% 12% 31% Freedland et al. 1113 1996–2006 TRUS 10, 6–40 (Median, range) 62% 27% 32% 11% 53% Gofrit et al. 448
Only Gleason score 6 2003–2006 TRUS ≥8 — — 20% — — Kahl et al. 185 1999–2003 TRUS 24, 13–33 (Mean, range) 20% 57% — 24% 42% 55 1997–2001 TRUS 9 (Mean, ≤12) 24% 60% — 16% 37% Numao et al. 143 2002–2006 TRUS + transperineal 26 92% — 26% — 20% Richstone et al. 4035 1983–2003 TRUS 6, 2–39 (Median, range) 66% ∗ 30% 36% 6% 49% Sfoungaristos et al. 271 2005–2010 TRUS 11–13 (Mean, different groups) 44% 42% 64% 14% 31% Arsov et al. 8 2010–2011 TRUS + MRI visually directed 11 (Median) 63% 37% 25% 0% 0% Baco et al. 128 2010–2013 TRUS + MRI fusion Targeted cores 2, 1–4 per lesion (median, range) + mapping biopsies (number not specified) 80% ∗ 16% 30% 14% 20% Hambrock et al. 64 2006–2009 TRUS 10 55% 44% 56% 1% 28% 34 MRI in-bore 3, 1–5 (Median, range) 88% 12% 8% 0% 35% Labanaris et al. 70 2004–2009 TRUS + MRI visually directed 3–6 90% 9% 9% 1% — Le et al. 54 2010–2013 TRUS + MRI fusion combined 18, 15–20 (Mean, range) 72% 7% — 20% 13% 54 2010–2013 TRUS 12 50% 39% — 11% 54 2010–2013 MRI fusion 6, 4–8 (Mean, range) 57% 31% — 11% Zhang et al. 40 (48 Tumors in 40 patients) 2010–2013 TRUS 12-core versus TRUS + MRI visually directed 12–18 77% 13% 29% 2% 29% Own data 50 2007–2014 MRI in-bore 4, 2–6 (Median, range) 66% 30% 44% 4% 20%
MRI, magnetic resonance imaging; TRUS, transrectal ultrasound.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Upgrading
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Significant Upgrading
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Downgrading
Get Radiology Tree app to read full this article<
Number and Quality of Positive Cores
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Epstein J.I., Allsbrook W.C., Amin M.B., et. al.: The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason grading of prostatic carcinoma. Am J Surg Pathol 2005; 29: pp. 1228-1242.
2. Cohen M.S., Hanley R.S., Kurteva T., et. al.: Comparing the Gleason prostate biopsy and Gleason prostatectomy grading system: the Lahey Clinic Medical Center experience and an international meta-analysis. Eur Urol 2008; 54: pp. 371-381.
3. Epstein J.I., Feng Z., Trock B.J., et. al.: Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur Urol 2012; 61: pp. 1019-1024.
4. Corcoran N.M., Hong M.K., Casey R.G., et. al.: Upgrade in Gleason score between prostate biopsies and pathology following radical prostatectomy significantly impacts upon the risk of biochemical recurrence. BJU Int 2011; 108: pp. E202-E210.
5. Sfoungaristos S., Perimenis P.: Clinical and pathological variables that predict changes in tumour grade after radical prostatectomy in patients with prostate cancer. Can Urol Assoc J 2013; 7: pp. E93-E97.
6. Kahl P., Wolf S., Adam A., et. al.: Saturation biopsy improves preoperative Gleason scoring of prostate cancer. Pathol Res Pract 2009; 205: pp. 259-264.
7. Divrik R.T., Eroglu A., Sahin A., et. al.: Increasing the number of biopsies increases the concordance of Gleason scores of needle biopsies and prostatectomy specimens. Urol Oncol 2007; 25: pp. 376-382.
8. Chun F.K., Steuber T., Erbersdobler A., et. al.: Development and internal validation of a nomogram predicting the probability of prostate cancer Gleason sum upgrading between biopsy and radical prostatectomy pathology. Eur Urol 2006; 49: pp. 820-826.
9. Fanning D.M., Kay E., Fan Y., et. al.: Prostate cancer grading: the effect of stratification of needle biopsy Gleason score 4 + 3 as high or intermediate grade. BJU Int 2010; 105: pp. 631-635.
10. Chung M.S., Lee S.H., Lee D.H., et. al.: Is small prostate volume a predictor of Gleason score upgrading after radical prostatectomy?. Yonsei Med J 2013; 54: pp. 902-906.
11. Richstone L., Bianco F.J., Shah H.H., et. al.: Radical prostatectomy in men aged > or =70 years: effect of age on upgrading, upstaging, and the accuracy of a preoperative nomogram. BJU Int 2008; 101: pp. 541-546.
12. Freedland S.J., Kane C.J., Amling C.L., et. al.: Upgrading and downgrading of prostate needle biopsy specimens: risk factors and clinical implications. Urology 2007; 69: pp. 495-499.
13. Corcoran N.M., Hovens C.M., Hong M.K., et. al.: Underestimation of Gleason score at prostate biopsy reflects sampling error in lower volume tumours. BJU Int 2012; 109: pp. 660-664.
14. Heidenreich A., Bastian P.J., Bellmunt J., et. al.: EAU guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol 2014; 65: pp. 124-137.
15. Arsov C., Quentin M., Rabenalt R., et. al.: Repeat transrectal ultrasound biopsies with additional targeted cores according to results of functional prostate MRI detects high-risk prostate cancer in patients with previous negative biopsy and increased PSA—a pilot study. Anticancer Res 2012; 32: pp. 1087-1092.
16. Zhang J., Xiu J., Dong Y., et. al.: Magnetic resonance imaging directed biopsy improves the prediction of prostate cancer aggressiveness compared with a 12 core transrectal ultrasound guided prostate biopsy. Mol Med Rep 2014; 9: pp. 1989-1997.
17. Moore C.M., Robertson N.L., Arsanious N., et. al.: Image-guided prostate biopsy using magnetic resonance imaging-derived targets: a systematic review. Eur Urol 2013; 63: pp. 125-140.
18. Le J.D., Stephenson S., Brugger M., et. al.: Magnetic resonance imaging-ultrasound fusion biopsy for prediction of final prostate pathology. J Urol 2014; 192: pp. 1367-1373.
19. Haffner J., Lemaitre L., Puech P., et. al.: Role of magnetic resonance imaging before initial biopsy: comparison of magnetic resonance imaging-targeted and systematic biopsy for significant prostate cancer detection. BJU Int 2011; 108: pp. E171-E178.
20. Numao N., Kawakami S., Yokoyama M., et. al.: Improved accuracy in predicting the presence of Gleason pattern 4/5 prostate cancer by three-dimensional 26-core systematic biopsy. Eur Urol 2007; 52: pp. 1663-1668.
21. Gofrit O.N., Zorn K.C., Taxy J.B., et. al.: Predicting the risk of patients with biopsy Gleason score 6 to harbor a higher grade cancer. J Urol 2007; 178: pp. 1925-1928.
22. Capitanio U., Karakiewicz P.I., Valiquette L., et. al.: Biopsy core number represents one of foremost predictors of clinically significant Gleason sum upgrading in patients with low-risk prostate cancer. Urology 2009; 73: pp. 1087-1091.
23. Baco E., Ukimura O., Rud E., et. al.: Magnetic resonance imaging-transectal ultrasound image-fusion biopsies accurately characterize the index tumor: correlation with step-sectioned radical prostatectomy specimens in 135 patients. Eur Urol 2015; 67: pp. 787-794.
24. Labanaris A.P., Zugor V., Smiszek R., et. al.: Guided e-MRI prostate biopsy can solve the discordance between Gleason score biopsy and radical prostatectomy pathology. Magn Reson Imaging 2010; 28: pp. 943-946.
25. Hambrock T., Hoeks C., Hulsbergen-van de Kaa C., et. al.: Prospective assessment of prostate cancer aggressiveness using 3-T diffusion-weighted magnetic resonance imaging-guided biopsies versus a systematic 10-core transrectal ultrasound prostate biopsy cohort. Eur Urol 2012; 61: pp. 177-184.
26. Dickinson L., Ahmed H.U., Allen C., et. al.: Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: recommendations from a European consensus meeting. Eur Urol 2011; 59: pp. 477-494.
27. Tofts P.S., Brix G., Buckley D.L., et. al.: Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging 1999; 10: pp. 223-232.
28. Barentsz J.O., Richenberg J., Clements R., et. al.: ESUR prostate MR guidelines 2012. Eur Radiol 2012; 22: pp. 746-757.
29. Weiner A.B., Etzioni R., Eggener S.E.: Ongoing Gleason grade migration in localized prostate cancer and implications for use of active surveillance. Eur Urol 2014; 66: pp. 611-612.
30. Chun F.K., Briganti A., Shariat S.F., et. al.: Significant upgrading affects a third of men diagnosed with prostate cancer: predictive nomogram and internal validation. BJU Int 2006; 98: pp. 329-334.
31. Franiel T., Fritzsche F., Staack A., et. al.: Histopathologic quality of prostate core biopsy specimens: comparison of an MR-compatible biopsy needle and a ferromagnetic biopsy needle used for ultrasound-guided prostate biopsy. Rofo 2006; 178: pp. 1212-1218.
32. Jung A.J., Westphalen A.C., Kurhanewicz J., et. al.: Clinical utility of endorectal MRI-guided prostate biopsy: preliminary experience. J Magn Reson Imaging 2014; 40: pp. 314-323.
33. Pokorny M.R., de Rooij M., Duncan E., et. al.: Prospective study of diagnostic accuracy comparing prostate cancer detection by transrectal ultrasound-guided biopsy versus magnetic resonance (MR) imaging with subsequent MR-guided biopsy in men without previous prostate biopsies. Eur Urol 2014; 66: pp. 22-29.
34. Naughton C.K., Ornstein D.K., Smith D.S., et. al.: Pain and morbidity of transrectal ultrasound guided prostate biopsy: a prospective randomized trial of 6 versus 12 cores. J Urol 2000; 163: pp. 168-171.
35. Netto G.J., Eisenberger M., Epstein J.I., Investigators TAXT: Interobserver variability in histologic evaluation of radical prostatectomy between central and local pathologists: findings of TAX 3501 multinational clinical trial. Urology 2011; 77: pp. 1155-1160.
36. Allsbrook W.C., Mangold K.A., Johnson M.H., et. al.: Interobserver reproducibility of Gleason grading of prostatic carcinoma: urologic pathologists. Hum Pathol 2001; 32: pp. 74-80.
37. Turker P., Bas E., Bozkurt S., et. al.: Presence of high grade tertiary Gleason pattern upgrades the Gleason sum score and is inversely associated with biochemical recurrence-free survival. Urol Oncol 2013; 31: pp. 93-98.