
Rationale and Objectives
To assess whether the accuracy of opposed-phase magnetic resonance (MR) imaging to differentiate spinal metastases from benign lesions is influenced by treatment.
Materials and Methods
We retrospectively evaluated 25 benign lesions, 25 untreated spinal metastases, and 89 treated spinal metastases in 101 patients who underwent opposed-phase MR spine imaging at our institution. The largest possible region of interest was placed over the lesion in question on out-of-phase and in-phase MR sequences, and the signal intensity ratio (SIR) of the lesions was calculated. The SIRs were compared between benign, untreated, and treated lesions. Receiver operator characteristic (ROC) curves were used to identify the optimal threshold to differentiate benign lesions from untreated spinal metastases, and the accuracy of this threshold was assessed for treated spinal metastases, chemotherapy-treated spinal metastases, and radiated spinal metastases.
Results
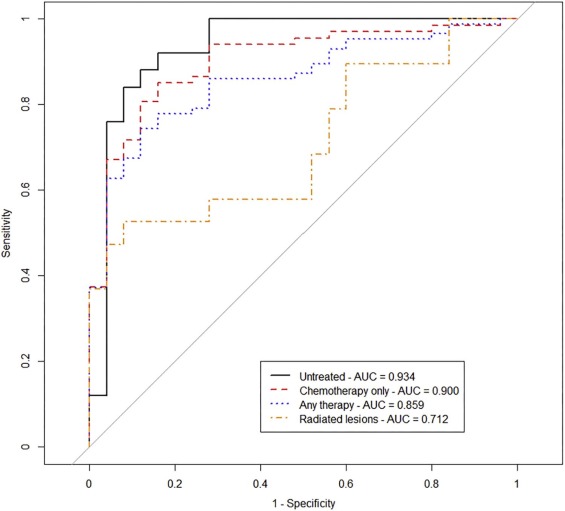
Benign lesions had lower mean SIR than untreated ( P = 2.4 × 10 −8 , 95% confidence interval [0.29, 0.51]) and treated spinal metastases ( P = .51; 95% confidence interval [−0.13, 0.06]). A cutoff SIR of 0.856 had an accuracy of 88.00% for untreated lesions, 77.48% for previously treated lesions, and 70.45% for previously radiated lesions. The ROC curve to differentiate benign lesions from radiated spinal metastases was significantly different from the ROC curve to differentiate benign lesions from untreated spinal metastases ( P = .0180). The ROC curve to differentiate benign lesions from lesions treated with chemotherapy only was significantly different from the ROC curve to differentiate between benign lesions and radiated spinal metastases ( P = .041).
Conclusions
Opposed-phase imaging is less accurate for treated spinal metastases, in particular after radiation.
Introduction
Differentiating benign lesions from spinal metastases is sometimes a challenge for radiologists using conventional magnetic resonance imaging (MRI) . This is of tremendous clinical importance because spinal metastases represent advanced stage disease and portends poor prognosis. Mistakenly proposing that a lesion is a spinal metastasis when it is a benign lesion may result in biopsy of the lesion or, in some cases, may alter the potential therapy available to the patient and consequently affect patient survival. Therefore, it is important that a radiologist accurately differentiate benign lesions from spinal metastases. Different MRI techniques have been used to evaluate suspected spinal metastases including routine spin echo sequences, contrast enhancement, and diffusion-weighted imaging .
Of the techniques used, opposed-phase MRI may be the most promising . Opposed-phase MRI uses chemical shift to detect intracytoplasmic lipid. Because fat- and water-associated protons resonate at different frequencies, imaging can be obtained when fat and water protons are aligned in the same direction (in-phase) and when they are aligned in opposite directions (out-of-phase). When these protons are “in-phase,” there is an additive effect increasing the signal intensity (SI) produced in the corresponding voxel. When the protons are “out of phase,” the signal from fat and water protons are in opposite directions, resulting in decreased SI in the corresponding voxel. Benign osseous lesions often have intracellular fat and higher lipid content, and as a result have decreased SI on out-of-phase images . Opposed-phase MRI has been used in imaging to differentiate benign from malignant lesions of the adrenal gland on the basis of intracellular lipid content . Opposed-phase MRI has been used for the evaluation of lesions of the spine to differentiate benign lesions from spinal metastases . The ratio of the SI on out-of-phase imaging to the SI on in-phase imaging is the signal intensity ratio (SIR). An SIR less than 0.80 has been used as a threshold to diagnose benign lesions , and lesions that have an SIR between 0.80 and 1.00 are often designated as indeterminate in clinical practice. Previous studies have shown that opposed-phase imaging can be used to differentiate benign from pathologic vertebral body fractures . Kenneally et al. also reported that opposed-phase imaging may be useful in differentiating benign from malignant primary tumors of bone .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 1, Forty-one–year-old female with oligometastatic breast cancer and L2 lesion. (a) Sagittal proton density-weighted magnetic resonance (MR) sequence (repetition time [TR] 1690 ms, echo time [TE] 8.7 ms) demonstrates a T1-hypointense lesion in the L2 vertebral body. White arrow shows the L2 metastatic lesion. (b) In-phase (TR 140 ms, TE 5.04 ms) and (c) out-of-phase images (TR 140 ms, TE 2.56 ms) demonstrate method of region of interest (ROI) measurement; SIR = 0.993.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/AccuracyofOpposedphaseMagneticResonanceImagingfortheEvaluationofTreatedandUntreatedSpinalMetastases/0_1s20S1076633217305123.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Reproducibility
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Demographic and Clinical Characteristics
Variable Benign ( N = 25) Untreated Spinal Metastases ( N = 25) Treated Spinal Metastases ( N = 86)P Value \* P Value † P Value ‡ Mean age (SD) 57.3 (13.9) 73.5 (9.6) 60.4 (10.3) 2.0 × 10 −5 .319 4.8 × 10 −7 Male sex, N (% male) 7 (28.0) 12 (48.0) 43 (50.0) .244 .068 1.00 Lesion location 1.00 1.00 .85 Cervical (%) 2 (8.0) 2 (8.0) 10 (11.6) Thoracic (%) 11 (44.0) 10 (40.0) 37 (43.0) Lumbar (%) 12 (48.0) 13 (52.0) 39 (45.3)
N , number of patients; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reproducibility
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of Mean SIR Values Between Benign, Treated, and Untreated Spinal Metastases
Comparison Group 1 Comparison Group 2 Wilcoxon Rank Sum P Value_t_ Test
P Value 95% CIBenign lesions ( N = 25)Untreated spinal metastases ( N = 25) 0.60 (0.25) 0.99 (0.10)4.0 × 10 −92.4 × 10 −8 (0.29, 0.51)Benign lesions ( N = 25)Treated spinal metastases ( N = 86) 0.60 (0.25) 1.03 (0.39)5.4 × 10 −81.4 × 10 −8 (0.30, 0.56)Untreated spinal metastases ( N = 25)Treated spinal metastases ( N = 86) 0.99 (0.10) 1.03 (0.39) 0.919 0.508 (−0.13, 0.06)
Bolded P Values are statistically significant.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Sensitivity, Specificity, Positive Predictive Value, Negative Predictive Value, and Accuracy of Opposed-phase MRI Using a Threshold SIR of 0.856
Treatment Sensitivity Specificity PPV NPV Accuracy Untreated spinal metastases 92.00% 84.00% 85.19% 91.30% 88.00% Spinal metastases treated with chemotherapy only 82.09% 84.00% 93.22% 65.63% 82.61% Spinal metastases treated with either chemotherapy and/or radiation therapy 75.58% 84.00% 94.20% 50.00% 77.48% Spinal metastases treated with radiation therapy 52.63% 84.00% 71.43% 70.00% 70.45%
NPV, negative predictive value; PPV, positive predictive value.
Table 4
DeLong Test Comparing ROC Curves
ROC Curve A ROC Curve B_P_ Value Benign lesions vs untreated spinal metastases Benign lesions vs radiated spinal metastases.018 Benign lesions vs untreated spinal metastases Benign lesions vs any prior therapy .164 Benign lesions vs untreated spinal metastases Benign lesions vs chemotherapy only .518 Benign lesions vs radiated spinal metastases Benign lesions vs any prior chemotherapy .113 Benign lesions vs radiated spinal metastases Benign lesions vs chemotherapy only.041 Benign lesions vs any prior chemotherapy Benign lesions vs chemotherapy only .420
ROC, receiver operating characteristic; vs, versus.
Bolded P Values are statistically significant.
Any prior therapy—radiation and/or chemotherapy.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Shah L.M., Salzman K.L.: Imaging of spinal metastatic disease. Int J Surg Oncol 2011; 2011: pp. 769753.
2. O’Sullivan G.J., Carty F.L., Cronin C.G.: Imaging of bone metastasis: an update. World J Radiol 2015; 7: pp. 202-211.
3. Kransdorf M.J., Bridges M.D.: Current developments and recent advances in musculoskeletal tumor imaging. Semin Musculoskelet Radiol 2013; 17: pp. 145-155.
4. Adam S.Z., Nikolaidis P., Horowitz J.M., et. al.: Chemical shift MR imaging of the adrenal gland: principles, pitfalls, and applications. Radiographics 2016; 36: pp. 414-432.
5. Disler D.G., McCauley T.R., Ratner L.M., et. al.: In-phase and out-of-phase MR imaging of bone marrow: prediction of neoplasia based on the detection of coexistent fat and water. AJR Am J Roentgenol 1997; 169: pp. 1439-1447.
6. Erly W.K., Oh E.S., Outwater E.K.: The utility of in-phase/opposed-phase imaging in differentiating malignancy from acute benign compression fractures of the spine. AJNR Am J Neuroradiol 2006; 27: pp. 1183-1188.
7. Ragab Y., Emad Y., Gheita T., et. al.: Differentiation of osteoporotic and neoplastic vertebral fractures by chemical shift {in-phase and out-of phase} MR imaging. Eur J Radiol 2009; 72: pp. 125-133.
8. Thawait S.K., Marcus M.A., Morrison W.B., et. al.: Research synthesis: what is the diagnostic performance of magnetic resonance imaging to discriminate benign from malignant vertebral compression fractures? Systematic review and meta-analysis. Spine 2012; 37: pp. E736-E744.
9. Zajick D.C., Morrison W.B., Schweitzer M.E., et. al.: Benign and malignant processes: normal values and differentiation with chemical shift MR imaging in vertebral marrow. Radiology 2005; 237: pp. 590-596.
10. Kenneally B.E., Gutowski C.J., Reynolds A.W., et. al.: Utility of opposed-phase magnetic resonance imaging in differentiating sarcoma from benign bone lesions. J Bone Oncol 2015; 4: pp. 110-114.
11. DeLong E.R., DeLong D.M., Clarke-Pearson D.L.: Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988; 44: pp. 837-845.
12. Martel Villagrán J., Bueno Horcajadas Á., Pérez Fernández E., et. al.: Accuracy of magnetic resonance imaging in differentiating between benign and malignant vertebral lesions: role of diffusion-weighted imaging, in-phase/opposed-phase imaging and apparent diffusion coefficient. Radiologia 2015; 57: pp. 142-149.
13. Amin W.M., Kotb H.T., Abdel-Kerim A.A., et. al.: Diffusion-weighted MRI and in-phase/opposed-phase sequences in the assessment of bone tumors. J Magn Reson Imaging 2016; 44: pp. 565-572.