
Rationale and Objectives
Diagnostic measures that can be used for sliding hiatal hernia are barium swallow radiography, endoscopy, manometry, and computed tomography. The aim of this study was to evaluate the diagnostic accuracy of transabdominal ultrasonography for sliding hiatal hernias.
Materials and Methods
This retrospective study was performed in the radiology department of a tertiary care center between May 2011 and May 2012. Twenty-one patients (10 females, 11 males) with sliding hiatal hernias and 41 controls (37 females, 4 males) were enrolled in this study. Esophageal hiatal diameters measured by ultrasonography and computerized tomography were compared. Correlation was tested via Pearson correlation analysis.
Results
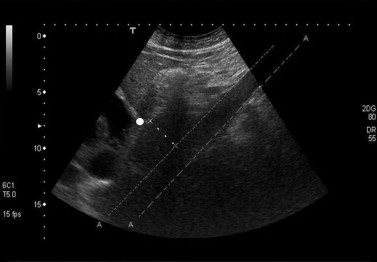
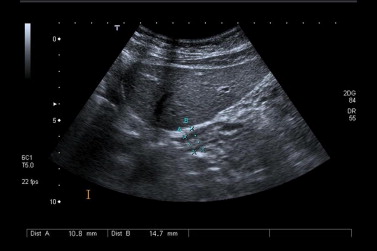
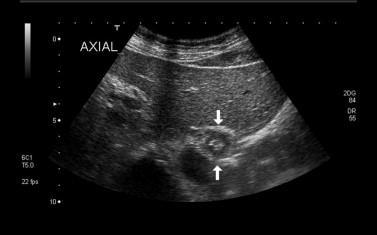
The average age of patients and controls were 58.6 and 40.1, respectively. There was a statistically significant difference between esophageal hiatal diameters measured via ultrasonography in patients (31.7 mm) and controls (11.6 mm) ( P < .001). Similarly, esophageal hiatal diameters measured via computed tomography in patients (31.4 mm) was statistically significantly higher than controls (11.5 mm) ( P < .001). The average body mass index of patients (28.3) was higher than that of control group ( P = .015). Ultrasonographic measurements were correlated well with tomographic results ( P = .000, r = 0.995).
Conclusion
Ultrasonography seems to be a valuable, safe, and practical alternative that avoids the side effects of contrast agents in the diagnosis of sliding hiatal hernias. Overall, we suggest that inclusion of ultrasound in the initial diagnostic steps for patients with sliding hiatal hernias may reduce the requirement for more expensive procedures.
Hiatal hernia (HH) is characterized with the proximal displacement of the gastroesophageal junction and stomach into the mediastinum through the esophageal hiatus. During normal swallowing, gastroesophageal junction and a small portion of the stomach is proximally displaced through the esophageal hiatus. If the phrenoesophageal ligament becomes loose because of the loss of elastic tissues with aging or repetitive stress of swallowing, HH may occur. HH is closely related to reflux symptoms, esophagitis, Barrett’s esophagus, and esophageal adenocarcinoma. Sliding HH must be included in the differential diagnosis of cardiac and pulmonary vascular diseases .
Diagnostic measures that can be used for sliding HH are barium swallow radiography, endoscopy, manometry, and computed tomography (CT). Even though the transabdominal ultrasonography (US) is known to be a practical and safe method, its role in the evaluation of gastroesophageal reflux and sliding HH has been limited up to now .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<


Table 1
Our Routine Protocol for Computed Tomography Scanning
Parameter Route and Duration of Administration Oral contrast 750–1000 mL iodized contrast Intravenous contrast 100–120 mL, iodized contrast, injected at 2 mL/sec Interval of image acquisition 70–90 sec (portal venous phase) Zone of image acquisition Superior border of diaphragm-symphysis pubis Section thickness 5–8 mm Pitch 1.5 Reconstruction interval 5–8 mm
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Demographic, Clinical, and Radiological Data of Our Cases
Patients ( n = 21) Controls ( n = 41)P Value Average age (y) (range) 58.6 (34–88) 40.1 (18–75) <.001 Gender (female; male; %) 10; 11 (47.6; 52.4) 37; 4 (90.2; 9.8) .002 Body-mass index (kg/m 2 ) (average; range) 28.3 (22.5–36) 15.0 (17.3–43.3) .015 Esophageal diameter (mm) at US (average; range) 31.7 (22.5–46.5) 11.6 (7.5–19.2) <.001 Esophageal diameter (mm) at CT (average; range) 31.4 (22.5–47.9) 11.5 (7.2–11.5) <.001
CT, computed tomography; US, ultrasonography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hyun J.J., Bak Y.T.: Clinical significance of hiatal hernia. Gut Liver 2011; 5: pp. 267-277.
2. Kahrilas P.J., Kim H.C., Pandolfino J.E.: Approaches to the diagnosis and grading of hiatal hernia. Best Pract Res Clin Gastroenterol 2008; 22: pp. 601.
3. Eren S., Ciriş F.: Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol 2005; 54: pp. 448.
4. Barone M., Di Lernia P., Carbonara M., et. al.: Sliding gastric hiatal hernia diagnosis by transabdominal ultrasonography: an easy, reliable and non-invasive procedure. Scand J Gastroenterol 2006; 41: pp. 851.
5. Aliotta A., Rapaccini G.L., Pompili M., et. al.: Ultrasonographic signs of sliding gastric hiatal hernia and their prospective evaluation. J Ultrasound Med 1995; 14: pp. 457.
6. Westra S.J., Wolf B.H., Staalman C.R.: Ultrasound diagnosis of gastroesophageal reflux and hiatal hernia in infants and young children. J Clin Ultrasound 1990; 18: pp. 477.
7. Changchien C.S., Hsu C.C.: Use of sonography in the evaluation of the gastroesophageal junction. J Clin Ultrasound 1996; 24: pp. 67-72.
8. Chen M.H., Kikuchi Y., Chu B.C., et. al.: Demonstration of the distal end of the esophagus by transabdominal ultrasound. Br J Radiol 1997; 70: pp. 1215.