
Rationale and Objectives
We sought to evaluate the automatic detection of the papillary muscle and to determine its influence on quantitative left ventricular (LV) mass assessment.
Materials and Methods
Twenty-eight Yorkshire-Landrace swine and 10 volunteers underwent cardiac magnetic resonance imaging (CMR) of the left ventricle. The variability in measurements of LV papillary muscles traced automatically and manually were compared to intra- and interobserver variabilities. CMR-derived LV mass with the papillary muscle included or excluded from LV mass measurements was compared to true mass at autopsy of the Yorkshire-Landrace swine.
Results
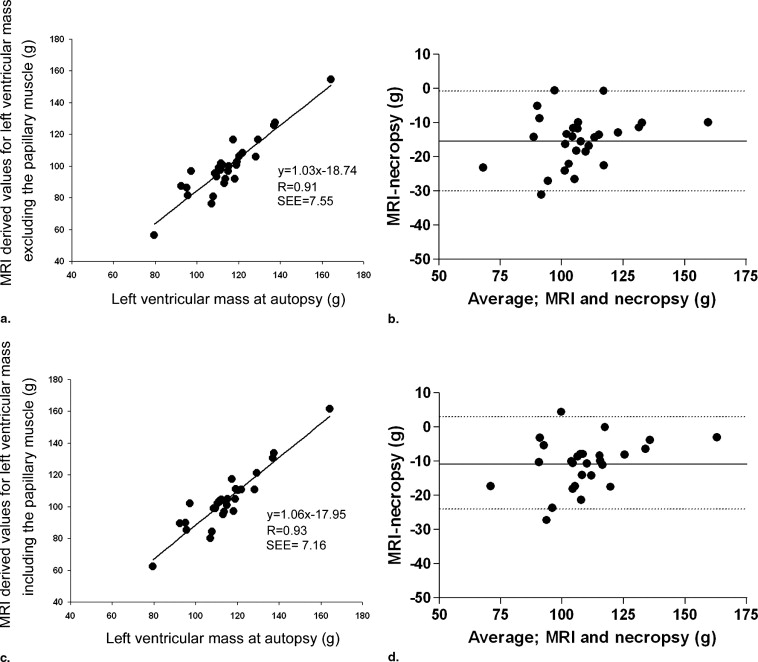
Automatic LV papillary muscle mass from all subjects correlated well with manually derived LV papillary muscle mass measurements ( r = 0.84) with no significant bias between both measurements (mean difference ± SD, 0.0 ± 1.5 g; P = .98). The variability in results related to the contour detection method used was not statistically significant different compared to intra- and interobserver variabilities ( P = .08 and P = .97, respectively). LV mass measurements including the papillary muscle showed significantly less underestimation (−10.6 ± 7.1 g) with the lowest percentage variability (6%) compared to measurements excluding the papillary muscles (mean underestimation, −15.1 ± 7.4 g percentage variability, 7%).
Conclusion
The automatic algorithm for detecting the papillary muscle was accurate with variabilities comparable to intra- and interobserver variabilities. LV mass is determined most accurately when the papillary muscles are included in the LV mass measurements. Taken together, these observations warrant the inclusion of automatic contour detection of papillary muscle mass in studies that involve the determination of LV mass.
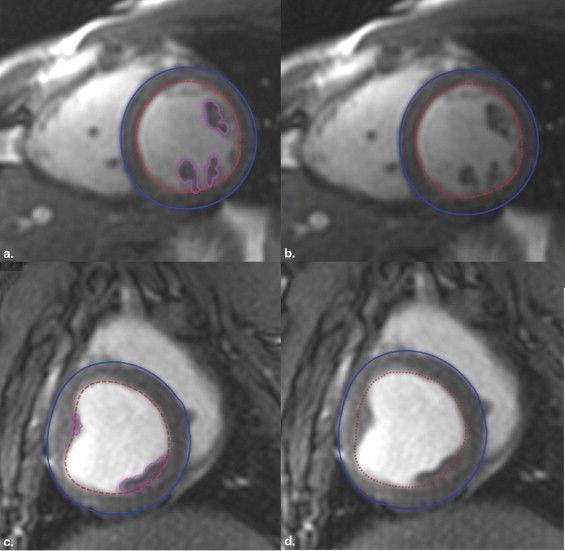
The measurements of left ventricular (LV) function by cardiac magnetic resonance imaging (CMR) are accurate and reproducible compared to those obtained through other imaging modalities ( ). Measurement of LV mass by CMR is also highly reproducible, but both significant underestimation and overestimation in comparison with LV mass at autopsy have been reported ( ). In previous CMR studies of LV mass, the papillary muscles were typically excluded because the manual tracing required to measure these complex structures is time consuming. Recent improvements in CMR sequences have increased both the resolution and contrast ratios, making it easier to distinguish between blood pool and muscle ( ). As a result, the papillary muscles are presently easier to identify. These improvements in CMR combined with modern analysis software allow automatic identification of papillary muscle, within a short time frame. This study compares the in vivo measurement of LV papillary muscle mass using automatically drawn contours on CMR scans with those obtained manually as well as with ex vivo LV mass measurements at autopsy.
Materials and methods
Animals
Twenty-eight Yorkshire-Landrace swine (35–50 kg) were sedated with 20 mg/kg ketamine and 1 mg/kg midazolam intramuscularly, anesthetized with 12 mg/kg thiopental intravenously, intubated, and mechanically ventilated with a 1:2 mixture of oxygen and nitrogen. Anesthesia was maintained with fentanyl (12.5 μg/kg/hour). All 28 swine underwent magnetic resonance imaging (MRI) and were sacrificed the next day. Subsequently, the heart was removed and the left ventricle was isolated by dissecting out the mitral and aortic valves, atria, and right ventricle. Experiments complied with The Guide for Care and Use of Laboratory Animals of the National Institutes of Health (NIH Publication No. 86-23, revised 1996) and were approved by the Erasmus Medical Center Animal Care Committee.
Volunteers
Get Radiology Tree app to read full this article<
MRI Protocol
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Papillary Muscle Mass
Get Radiology Tree app to read full this article<
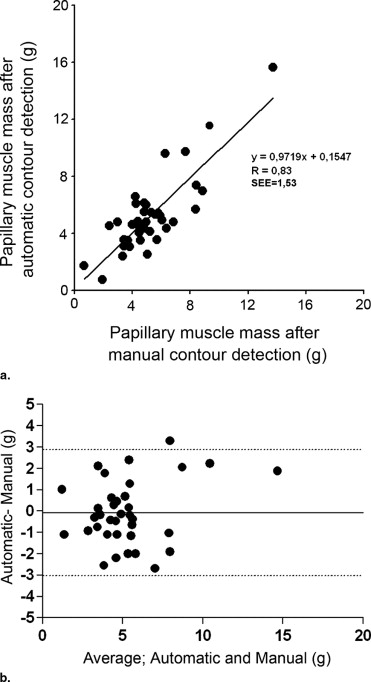
Table 1
Agreement Between Automatic and Manual Papillary Muscle Mass with Respect to Intra- and Interobserver Variabilities of Manual Contouring
Mass Automatic vs. Manual Intraobserver Variability Interobserver Variability Volunteer (g) 6.9 ± 3.0 0.1 ± 1.6 0.1 ± 1.0 −2.1 ± 1.7 Swine (g) 4.7 ± 1.8 −0.0 ± 1.5 −0.4 ± 1.3 0.6 ± 0.9 Volunteer + Swine (g) 5.3 ± 2.4 0.0 ± 1.5 0.2 ± 1.1 1.4 ± 1.6
The values are expressed as mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Total LV Mass
Get Radiology Tree app to read full this article<
Table 2
Left Ventricular (LV) Mass Measurements, Including and Excluding the Papillary (Pap) Muscles Compared to Ex-vivo Mass Measurements
Pigs ED Mass Pap− (g) ED Mass Pap+ (g) Mean ± SD 103.8 ± 18.2 99.2 ± 18.0 Correlation 0.93 0.92 R 2 0.85 0.84 Difference (g) −10.6 ± 7.1 −15.1 ± 7.4 Variability (%) 6% 7%P value <0.001 <0.001
ED: end-diastolic.
Mean ± standard deviation (SD) and mean difference ± SD of the difference between calculated LV mass and LV mass at autopsy are measured. Results of the paired t -test for comparison between calculated LV mass with ex-vivo LV mass (114.6 ± 16.1 g).
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Katz J., Milliken M.C., Stray-Gundersen J., et. al.: Estimation of human myocardial mass with MR imaging. Radiology 1988; 169: pp. 495-498.
2. Stratemeier E.J., Thompson R., Brady T.J., et. al.: Ejection fraction determination by MR imaging: Comparison with left ventricular angiography. Radiology 1986; 158: pp. 775-777.
3. Semelka R.C., Tomei E., Wagner S., et. al.: Normal left ventricular dimensions and function: Interstudy reproducibility of measurements with cine MR imaging. Radiology 1990; 174: pp. 763-768.
4. Semelka R.C., Tomei E., Wagner S., et. al.: Interstudy reproducibility of dimensional and functional measurements between cine magnetic resonance studies in the morphologically abnormal left ventricle. Am Heart J 1990; 119: pp. 1367-1373.
5. Bloomgarden D.C., Fayad Z.A., Ferrari V.A., Chin B., Sutton M.G., Axel L.: Global cardiac function using fast breath-hold MRI: Validation of new acquisition and analysis techniques. Magn Reson Med 1997; 37: pp. 683-692.
6. Lorenz C.H., Walker E.S., Morgan V.L., Klein S.S., Graham T.P.: Normal human right and left ventricular mass, systolic function, and gender differences by cine magnetic resonance imaging. J Cardiovasc Magn Reson 1999; 1: pp. 7-21.
7. Moon J.C., Lorenz C.H., Francis J.M., Smith G.C., Pennell D.J.: Breath-hold FLASH and FISP cardiovascular MR imaging: Left ventricular volume differences and reproducibility. Radiology 2002; 223: pp. 789-797.
8. van Geuns R.J., Baks T., Gronenschild E.H., et. al.: Automatic quantitative left ventricular analysis of cine MR images by using three-dimensional information for contour detection. Radiology 2006; 240: pp. 215-221.
9. Bland J.M., Altman D.G.: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1: pp. 307-310.
10. van der Geest R.J., Buller V.G., Jansen E., et. al.: Comparison between manual and semiautomated analysis of left ventricular volume parameters from short-axis MR images. J Comput Assist Tomogr 1997; 21: pp. 756-765.
11. Sievers B., Kirchberg S., Bakan A., Franken U., Trappe H.J.: Impact of papillary muscles in ventricular volume and ejection fraction assessment by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2004; 6: pp. 9-16.
12. Francois C.J., Fieno D.S., Shors S.M., Finn J.P.: Left ventricular mass: Manual and automatic segmentation of true FISP and FLASH cine MR images in dogs and pigs. Radiology 2004; 230: pp. 389-395.
13. Vogel-Claussen J., Finn J.P., Gomes A.S., et. al.: Left ventricular papillary muscle mass: Relationship to left ventricular mass and volumes by magnetic resonance imaging. J Comput Assist Tomogr 2006; 30: pp. 426-432.
14. Yamaoka O., Yabe T., Okada M., et. al.: Evaluation of left ventricular mass: Comparison of ultrafast computed tomography, magnetic resonance imaging, and contrast left ventriculography. Am Heart J 1993; 126: pp. 1372-1379.
15. Weinsaft J.W., Cham M.D., Janik M., et. al.: Left ventricular papillary muscles and trabeculae are significant determinants of cardiac MRI volumetric measurements: Effects on clinical standards in patients with advanced systolic dysfunction. Int J Cardiol 2007; 126: pp. 359-365.
16. Papavassiliu T., Kuhl H.P., Schroder M., et. al.: Effect of endocardial trabeculae on left ventricular measurements and measurement reproducibility at cardiovascular MR imaging. Radiology 2005; 236: pp. 57-64.