
Rationale and Objectives
We sought to assess retrospectively the added value of coronal reformations from isotropic voxels obtained with 64-slice multidetector row computed tomography (CT) of the acute abdomen.
Materials and Methods
This retrospective study was approved by the institutional review board and informed consent was waived. Multidetector helical 64-section CT (section thickness, 0.6 mm; pitch 1.75; table speed 35 mm/sec) was performed in 100 patients (60 women and 40 men; age range, 9∓85 years; mean age, 45.2 years) with acute nontraumatic abdominal pain who had been referred from the emergency department. Axial images were reconstructed with 5-mm-thick sections at 5-mm intervals. The second data set was reformatted coronally, with 3-mm-thick sections at 3-mm intervals. Four independent, blinded readers with various level of training interpreted first the axial scans alone and then followed immediately by the coronal scans. Confidence in the visualization of anatomy and pathology was scored on a 5-point scale. The final diagnosis was determined by surgical and pathologic reports and by clinical follow-up in those who did not undergo surgery.
Results
Based upon the individual patient’s clinical history and other comorbid factors, 92 patients received intravenous contrast and 90 patients received oral contrast. In 45 patients, no CT abnormalities were detected for an explanation of the abdominal pain. Mean sensitivity and specificity of axial CT alone were 92.5% and 91%, respectively. No significant differences in sensitivity and specificity were observed for the use of combined axial and coronal images. For the most inexperienced reader, the coronal reformations were helpful in 95% of cases, while for the most experienced reader, the coronal reformations were helpful in 35% of the cases. The coronal images were deemed helpful in an average of 62.3% of the cases for the four readers. However, diagnosing subtle pathology in the abdominal wall was difficult on coronal reformations alone. Overall, coronal reformations improved diagnostic confidence and interobserver agreement over axial images alone for visualization of normal abdominal structures and in the diagnosis of abdominal pathology.
Conclusion
Axial and coronal reformations of 64-section multidetector row CT have equal sensitivity and specificity for the diagnosis of acute abdominal pathology. However, coronal reformations improved the diagnostic confidence for all readers but most significantly for the least experienced. Therefore, radiology departments with residents should consider routinely generating coronal images in patients with acute abdominal pain.
A wide variety of potential life-threatening medical and surgical diseases can cause acute abdominal pain; thus, the management of patients with acute abdominal syndrome requires an accurate and rapid diagnosis to reduce morbidity and mortality and to direct proper management.
Spiral computed tomography (CT) has become the investigation of choice in the imaging evaluation of patients with acute abdominal pain because it is rapid, cost-effective and provides a global perspective of abdominal structures. Numerous studies indicate that CT provides useful diagnostic information in the evaluation of patients with acute abdominal pain ( ). The increased availability of multidetector row CT (MDCT) in emergency departments results in near universal utilization.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patients and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Image Quality
Get Radiology Tree app to read full this article<

Table 1
Mean Confidence Score for the Detection of Different Organ Systems for Four Readers
Scan Liver Gallbladder Pancreas Adrenal Glands Kidney Spleen Small Intestines Colon Urinary Bladder Genital Organs Vessels Lymph Nodes Skeleton Transverse Alone 4.77 4.02 4.60 4.56 4.79 4.80 4.48 4.54 4.26 4.02 4.80 4.70 4.91 Transverse and coronal 4.78 4.02 4.52 4.62 4.76 4.80 4.50 4.61 4.28 4.03 4.79 4.72 4.88P value ⁎ .861 .910 <.01 <.05 .065 .561 .491 .01 .236 .451 .589 .617 .154
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Abnormalities Detected at CT
Get Radiology Tree app to read full this article<
Table 2
Principal Findings on CT Scans. (Number of Patients)
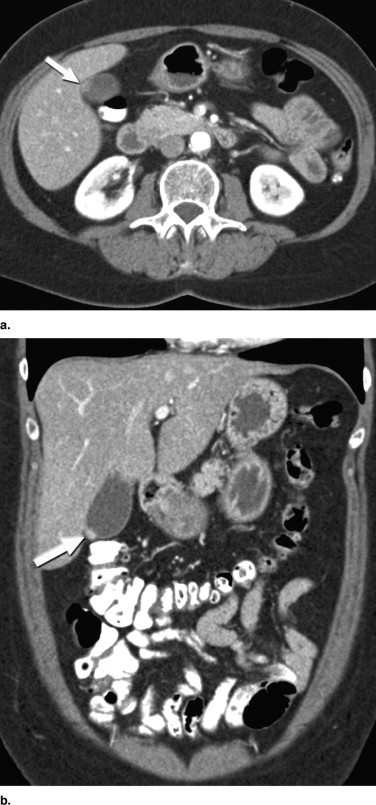
Normal findings 30 No acute pathology 15 Cholecystitis/cholelithiasis 4 Abscess 7 Pancreatic cancer 2 Gallbladder cancer 1 Acute/chronic pancreatitis 5 Hydronephrosis/calculi 4 Small bowel ileus/intussusception 2 Small bowel inflammation 3 Colonic inflammation 7 Diverticulosis 3 Appendicitis 3 Renal cancer 1 Drain malposition 2 Hydrosalpinx 1 Pneumonia 2 Lung metastasis of a carcinoma of unknown primary CUP 1 Ovarian vein thrombosis 1 Ascites/peritoneal dialysis fluid 2 Esophageal hernia 2 Lymphadenopathy 2 Vertebral body fractures 1
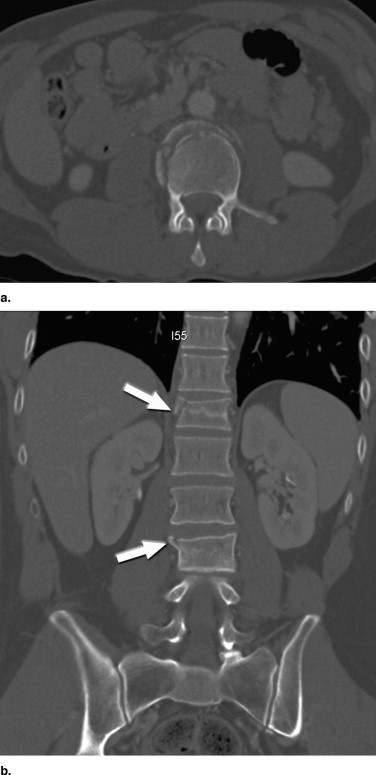
Table 3
Sensitivity and Specificity Values for the Diagnosis of Pathologies
Transverse Scans Alone Combined Transverse and Coronal Scans Reader Sensitivity (%) Specificity(%) AUC Sensitivity (%) Specificity (%) AUC 1 (Radiologist) 94 91 0.947 94 90 0.916 2 (Senior medical student) 93 90 0.927 92 91 0.971 3 (Resident, second year) 91 91 0.964 91 91 0.985 4 (Resident, fourth year) 92 91 0.951 93 91 0.934
There were no significant differences in sensitivity and specificity between transverse scans alone and combined transverse and coronal scans for any reader.
Get Radiology Tree app to read full this article<
Reader Agreement
Get Radiology Tree app to read full this article<
Table 4
Reader Agreement for the Diagnosis of Abdominal Pathology
Reader Combinations Axial Scans Alone Combined Axial and Coronal Scans Readers 1 and 2 0.80 0.83 Readers 2 and 3 0.73 0.78 Readers 1 and 3 0.70 0.77 Readers 3 and 4 0.72 0.84 Readers 1 and 4 0.76 0.81 Readers 2 and 4 0.74 0.79
Numbers are the mean weighted κ statistics. The differences between image sets were statistically significant ( P = 0.023).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Mean Confidence Scores for the Detection of Abdominal Pathology
Confidence Score Transverse Scans Alone Transverse Plus Coronal Scans R1 R2 R3 R4 Mean R1 R2 R3 R4 Mean 1 0 0 0 0 0 0 1 0 0 0 2 1 1 2 2 2 1 0 4 3 2 3 3 6 12 10 8 3 2 13 10 7 4 29 41 34 56 40 15 33 32 53 33 5 67 52 48 29 49 81 64 48 31 56
Data are given as number of patients. The differences based on the mean of the four readers were significant ( P < 0.001). Post-hoc (Dunn’s) R1 is R3 and R4 ( P < 0.05).
Get Radiology Tree app to read full this article<
Added Value of Coronal Images
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Bolog N., Popiel A., Oancea I., Mangrau A., Beuran M., Nicolau E.: Multidetector row spiral CT (MDCT) in bowel related non-traumatic abdominal emergencies. J Gastroenterol 2003; 12: pp. 319-324.
2. Frauenfelder T., Wildermuth S., Marincek B., Boehm T.: Nontraumatic emergent abdominal vascular conditions: Advantages of multidetector row CT and three-dimensional imaging. Radiographics 2004; 24: pp. 481-496.
3. Leschka S., Alkadhi H., Wildermuth S., Marincek B.: Multidetector computed tomography of acute abdomen. Eur Radiol 2005; 15: pp. 2435-2447.
4. Wong K., Paulson E.K., Nelson R.C.: Breath-hold three-dimensional CT of the liver with multidetector row helical CT. Radiology 2001; 219: pp. 75-79.
5. Marincek B.: Nontraumatic abdominal emergencies: Acute abdominal pain: Diagnostic strategies. Eur Radiol 2002; 12: pp. 2136-2150.
6. Ahn S.H., Mayo-Smith W.W., Murphy B.L., Reinert S.E., Cronan J.J.: Acute nontraumatic abdominal pain in adult patients: Abdominal radiography compared with CT evaluation. Radiology 2002; 225: pp. 159-164.
7. Gupta H., Dupuy D.E.: Advances in imaging of the acute abdomen. Surg Clin North Am 1997; 77: pp. 1245-1263.
8. Johnson G.L., Johnson P.T., Fishman E.K.: CT evaluation of the acute abdomen: Bowel pathology spectrum of disease. Crit Rev Diagn Imaging 1996; 37: pp. 163-190.
9. Johnson G.L., Fishman E.K.: Using CT to evaluate the acute abdomen: Spectrum of urinary pathology. AJR Am J Roentgenol 1997; 168: pp. 273-276.
10. Rosen M.P., Sands D.Z., Longmaid H.E., Reynolds K.F., Wagner M., Raptopoulos V.: Impact of abdominal CT on the management of patients presenting to the emergency department with acute abdominal pain. AJR Am J Roentgenol 2000; 174: pp. 1391-1396.
11. Taourel P., Baron M.P., Pradel J., Fabre J.M., Seneterre E., Bruel J.M.: Acute abdomen of unknown origin: Impact of CT on diagnosis and management. Gastrointest Radiol 1992; 17: pp. 287-291.
12. Taourel P.G., Fabre J.M., Pradel J.A., Seneterre E.J., Megibow A.J., Bruel J.M.: Value of CT in the diagnosis and management of patients with suspected acute small-bowel obstruction. AJR Am J Roentgenol 1995; 165: pp. 1187-1192.
13. Rosen M.P., Siewert B., Sands D.Z., Bromberg R., Edlow J., Raptopoulos V.: Value of abdominal CT in the emergency department for patients with abdominal pain. Eur Radiol 2003; 13: pp. 418-424.
14. Rhea J.T., Halpern E.F., Ptak T., Lawrason J.N., Sacknoff R., Novelline R.A.: The status of appendiceal CT in an urban medical center 5 years after its introduction: Experience with 753 patients. AJR Am J Roentgenol 2005; 184: pp. 1802-1808.
15. Cahir J.G., Freeman A.H., Courtney H.M.: Multislice CT of the abdomen. Br J Radiol 2004; 77: pp. S64-S73.
16. Nikolaou K., Flohr T., Knez A., et. al.: Advances in cardiac CT imaging: 64-Slice scanner. Int J Cardiovasc Imaging 2004; 20: pp. 535-540.
17. Caoili E.M., Cohan R.H., Inampudi P., et. al.: MDCT urography of upper tract urothelial neoplasms. AJR Am J Roentgenol 2005; 184: pp. 1873-1881.
18. Faria S.C., Tamm E.P., DuBrow R., et. al.: Use of thin-section, multidetector row helical CT images for coronal oblique reformations for optimal visualization of structures in the hepatoduodenal ligament. Abdom Imaging 2004; 29: pp. 231-238.
19. Gong J.S., Xu J.M.: Role of curved planar reformations using multidetector spiral CT in diagnosis of pancreatic and peripancreatic diseases. World J Gastroenterol 2004; 10: pp. 1943-1947.
20. Johnson P.T., Heath D.G., Hofmann L.V., Horton K.M., Fishman E.K.: Multidetector-row computed tomography with three-dimensional volume rendering of pancreatic cancer: A complete preoperative staging tool using computed tomography angiography and volume-rendered cholangiopancreatography. J Comput Assist Tomogr 2003; 27: pp. 347-353.
21. Kang H.K., Jeong Y.Y., Choi J.H., et. al.: Three-dimensional multidetector row CT portal venography in the evaluation of portosystemic collateral vessels in liver cirrhosis. Radiographics 2002; 22: pp. 1053-1061.
22. Prokesch R.W., Chow L.C., Beaulieu C.F., et. al.: Local staging of pancreatic carcinoma with multidetector row CT: Use of curved planar reformations initial experience. Radiology 2002; 225: pp. 759-765.
23. Caoili E.M., Cohan R.H., Korobkin M., et. al.: Urinary tract abnormalities: Initial experience with multidetector row CT urography. Radiology 2002; 222: pp. 353-360.
24. Caoili E.M., Paulson E.K.: CT of small-bowel obstruction: Another perspective using multiplanar reformations. AJR Am J Roentgenol 2000; 174: pp. 993-998.
25. Furukawa A., Yamasaki M., Furuichi K., et. al.: Helical CT in the diagnosis of small bowel obstruction. Radiographics 2001; 21: pp. 341-355.
26. Aufort S., Charra L., Lesnik A., Bruel J.M., Taourel P.: Multidetector CT of bowel obstruction: Value of post-processing. Eur Radiol 2005; 15: pp. 2323-2329.
27. Taourel P., Kessler N., Lesnik A., Pujol J., Morcos L., Bruel J.M.: Helical CT of large bowel obstruction. Abdom Imaging 2003; 28: pp. 267-275.
28. Jaffe TA Martin L.C., Thomas J., Adamson A.R., DeLong D.M., Paulson E.K.: Small-bowel obstruction: Coronal reformations from isotropic voxels at 16-section multidetector row CT. Radiology 2005; 238: pp. 135-142.
29. Paulson E.K., Harris J.P., Jaffe T.A., Haugan P.A., Nelson R.C.: Acute appendicitis: Added diagnostic value of coronal reformations from isotropic voxels at multidetector row CT. Radiology 2005; 235: pp. 879-885.