
Rationale and Objectives
To evaluate multidetector computed tomography (MDCT) for detecting the early changes and dynamic evolution of acute mesenteric ischemia (AMI) induced by the ligation of superior mesenteric vein (SMV) in an experimental porcine model.
Materials and Methods
Twelve pigs were randomly assigned to three experimental groups, and one control group with three pigs in each group. After laparotomy, the SMV was separated and ligated in nine pigs and separated without ligation in three controls. MDCT pre- and postcontrast with arterial, venous, and delayed phase scans, and CT angiography reconstructions of mesenteric vessels were carried out at preoperation, 6 hours, 12 hours, and 18 hours after ligation. The findings of mesenteric vessels, bowel, abdominal cavity at pre- and postoperation, and dynamic evolution were correlated with pathology.
Results
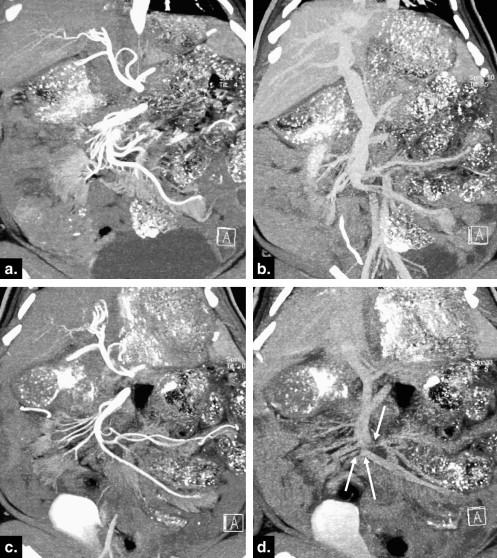
AMI-induced pathological changes were identified in all nine experimental pigs. MDCT angiography clearly delineated main trunk of the SMV, peripheral major and minor tributaries up to brushy vasa recta, and the location and shape of ligations. The early ischemic findings were bowel wall thickening, mesenteric edema, ascites, and pronounced bowel enhancement. Superior mesenteric artery and its major branches appeared spasm with poor filling and delayed and prolonged visualization. SMV and its tributaries were poorly delineated with delayed opacification. We also saw thinning of bowel wall, dilatating bowel with fluid, aggravating mesenteric edema and ascites, and poor enhanced bowel over time.
Conclusion
MDCT detects early changes of mesenteric ischemia and its evolution after ligation of porcine SMV, and may find application in early diagnosis of human venous occlusive AMI.
Mesenteric venous thrombosis (MVT) remains a lethal disease. It usually results in acute mesenteric ischemia (AMI) and even necrosis if not promptly treated. The 30-day mortality is 20%–27% . Because of variations in clinical manifestations, courses, and prognosis from different etiology of MVT, it is hard to diagnose acute MVT at an early stage. Improvements in noninvasive imaging techniques, especially multidetector computed tomography (MDCT), may lead to a more favorable outcome of acute MVT . Identifying patients earlier in their clinical courses can not only avoid intestinal necrosis and unnecessary surgery, but also prompt nonoperative management such as interventional therapy, and hence reduce mortality. According to Zhang et al , mortality rate reached up to 39% in patients with acute MVT who underwent surgical therapy, whereas nonoperative management or interventional therapy markedly reduced hospital mortality.
It was shown that sensitivity and specificity of MDCT for MVT were both higher than 90% when MVT occurs in main trunk of superior mesenteric vein (SMV) or portal vein, whereas characteristic changes of AMI usually appeared at a late stage. The value of MDCT remains uncertain in the identification of the early AMI, or in MVT involving predominantly the small mesenteric veins. A retrospective study by Kumar et al suggested that 44% of MVT predominantly involved the small mesenteric veins, which was more difficult to diagnose early, more likely to develop bowel necrosis, and more frequently required surgery.
Get Radiology Tree app to read full this article<
Materials and methods
Animal Preparation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Data Analysis
Get Radiology Tree app to read full this article<
Pathological Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
CTA Manifestations of Normal SMV
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
CTA Findings of Mesenteric Ischemia
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Abnormal CT Findings of Bowel and Abdominal Cavity
Get Radiology Tree app to read full this article<
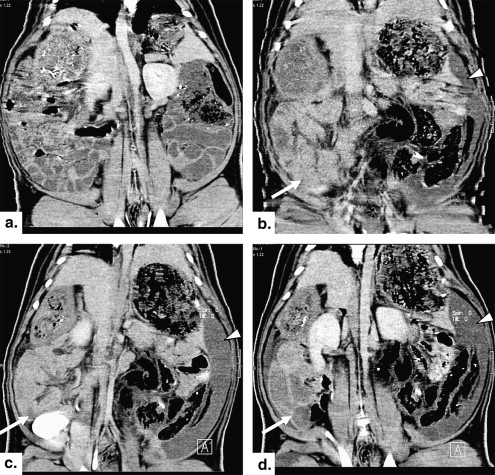
Table 1
Abnormal Computed Tomography Findings of Bowel and Abdominal Cavity and Dynamic Evolution
Abnormal Computed Tomography Findings 6 Hours
( n = 9) 12 Hours
( n = 6) 18 Hours
( n = 3) Controls
( n = 3) Thickening of bowel wall 9 (100%) ∗ 5 (83%) ∗ 1 (33%) 0 Thinning of bowel wall 0 (0) 1 (17%) 2 (67%) 0 Bowel dilatation with fluid 1 (11%) 2 (33.3%) 3 (100%) 0 Mesenteric edema 9 (100%) ∗ 6 (100%) ∗ 3 (100%) 0 Ascites 8 (89%) ∗ 6 (100%) ∗ 3 (100%) 0 Increased enhancement of bowel wall 9 (100%) ∗ 0 (0) 0 (0) 0 Reduced enhancement of bowel wall 0 (0) 6 (100%) ∗ 3 (100%) 0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pathologic Findings
Gross observation
Get Radiology Tree app to read full this article<
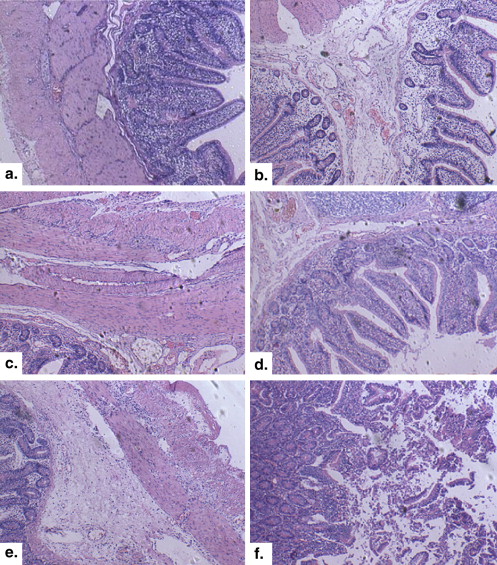
Histological findings
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Rhee R.Y., Gloviczki P., Mendonca C.T., et. al.: Mesenteric venous thrombosis: still a lethal disease in the 1990s. J Vasc Surg 1994; 20: pp. 688-697.
2. Morasch M.D., Ebaugh J.L., Chiou A.C., et. al.: Mesenteric venous thrombosis: a changing clinical entity. J Vasc Surg 2001; 34: pp. 680-684.
3. Grieshop R.J., Dalsing M.C., Cikrit D.F., et. al.: Acute mesenteric venous thrombosis. Revisited in a time of diagnostic clarity. Am Surg 1991; 57: pp. 573-578.
4. Acosta S., Alhadad A., Svensson P., et. al.: Epidemiology, risk and prognostic factors in mesenteric venous thrombosis. Br J Surg 2008; 95: pp. 1245-1251.
5. Bradbury M.S., Kavanagh P.V., Chen M.Y., et. al.: Noninvasive assessment of portomesenteric venous thrombosis: current concepts and imaging strategies. J Comput Assist Tomogr 2002; 26: pp. 392-404.
6. Wildermuth S., Leschka S., Alkadhi H., et. al.: Multislice CT in the pre and post interventional evaluation of mesenteric perfusion. Eur Radiol 2005; 15: pp. 1203-1210.
7. Zhang J., Duan Z.Q., Song Q.B., et. al.: Acute mesenteric venous thrombosis: a better outcome achieved through improved imaging techniques and a changed policy of clinical management. Eur J Vasc Endovsc Surg 2004; 28: pp. 329-334.
8. Aschoff A.J., Stuber G., Becker B.W., et. al.: Evaluation of acute mesenteric ischemia: accuracy of biphasic mesenteric multi-detector CT angiography. Abdom Imaging 2009; 34: pp. 345-357.
9. Kumar S., Kamath P.S.: Acute superior mesenteric venous thrombosis: one disease or two?. Am J Gastroenterol 2003; 98: pp. 1299-1304.
10. Shih M.P., Hagspiel K.D.: CTA and MRA in mesenteric ischemia: part 1, role in diagnosis and differential diagnosis. Am J Roentgenol 2007; 188: pp. 452-461.
11. Bradbury M.S., Kavanagh P.V., Bechtold R.E., et. al.: Mesenteric venous thrombosis: diagnosis and noninvasive imaging. RadioGraphics 2002; 22: pp. 527-541.
12. Polk H.C.: Experimental mesenteric venous occlusion III: diagnosis and treatment of induced mesenteric venous thrombosis. Ann Surg 1966; 163: pp. 432-444.
13. Friedenberg M.J., Polk H.C., McAlister W.H., et. al.: Superior mesenteric arteriography in experimental mesenteric venous thrombosi. Radiology 1965; 85: pp. 38-45.
14. Jackson B.B.: Venous occlusion of the terminal ileum: an experimental study. Surgery 1961; 50: pp. 322-327.
15. Kreft B.K., Strunk H., Flacke S., et. al.: Detection of thrombosis in the portal venous system: comparison of contrast-enhanced MR angiography with intraarterial digital subtraction angiography. Radiology 2000; 216: pp. 86-92.
16. Clark R.A., Gallant T.E.: Acute mesenteric ischemia: angiographic spectrum. Am J Roentgenol 1984; 142: pp. 555-562.
17. Romano S., Lassandro F., Scaglione M., et. al.: Ischemia and infarction of the small bowel and colon: spectrum of imaging findings. Abdom Imaging 2006; 31: pp. 277-292.
18. Chou C.K., Mak C.W., Tzeng W.S., et. al.: CT of small bowel ischemia. Abdom Imaging 2004; 29: pp. 18-22.
19. Kim J.Y., Ha H.K., Byun J.Y., et. al.: Intestinal infarction secondary to mesenteric venous thrombosis: CT-pathologic correlation. J Comput Assist Tomogr 1993; 17: pp. 382-385.
20. Zhang X.M., Yang H.F., Huang X.H., et. al.: The experimental study on bowel ischemia in closed loop obstruction by using multi-phase spiral CT. Chin J Radiol 2005; 39: pp. 755-760.