
Rationale and Objectives
This study aimed to determine the value of dual-energy thoracic radiography in the diagnosis of pneumothorax considering the reader’s experience.
Materials and Methods
Forty patients with a suspected pneumothorax, imaged with dual-energy chest radiographs, were divided into two groups: those with pneumothorax as the final diagnosis ( n = 19) and those without ( n = 21). The images were analyzed by 36 readers (5 interns, 16 residents, 15 senior physicians) for the presence or absence of pneumothorax during three readout sessions at 2-week intervals: standard images alone (session 1), dual-energy images with bone subtraction alone (session 2), and a combination of the two (session 3).
Results
The number of correct responses increased 13.3% between sessions 1 and 2 ( P < .001) and 9.4% between sessions 1 and 3 ( P < .001). The mean sensitivity for pneumothorax detection was higher in sessions 2 (82%) and 3 (79%) compared to session 1 (70%). There was no statistically significant difference in specificity between the sessions. The number of correct responses for small volume pneumothoraces was higher in sessions 2 (10.6 ± 1.8) and 3 (10.1 ± 2.0) than in session 1 (8.9 ± 2.3), with a statistically significant difference between sessions 1 and 2 ( P = .002) and between sessions 1 and 3 ( P = .048).
Conclusion
Bone subtracted dual-energy thoracic radiographs improve the detection sensitivity of pneumothorax, including in cases of small pneumothoraces, regardless of the reader’s level or expertise.
Introduction
Pneumothorax is a common condition, affecting an estimated 17 of 100,000 people in France and 34.8/100,000 in England . It requires precise and rapid diagnosis, and conventional radiography is usually the initial imaging method of choice. However, pneumothorax detection, particularly in cases of small pneumothoraces, may be difficult and sometimes requires the use of additional techniques, such as computed tomography (CT).
Dual-energy radiography is an expanding technique, thanks to an increase in the availability of flat panel detectors. Diagnostic improvement offered by this technique has been demonstrated in the detection of calcified and noncalcified lung nodules, and calcified thoracic lesions (mediastinal, pleural, or pulmonary) . Although no studies could be found in the literature analyzing the contribution of dual-energy digital radiography for the detection of pneumothorax, it seems that diagnostic performance could be improved by this technique because it can suppress bone structures of the thoracic wall, reducing superimposition and allowing a finer delimitation of lung contours.
Get Radiology Tree app to read full this article<
Materials and Methods
Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Radiographic Technique
Get Radiology Tree app to read full this article<
Reading and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Mean Number of Correct Answers by Stage and by Level of Expertise and Specialty
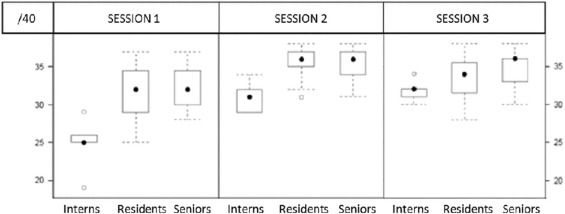
Session 1 Session 2 Session 3 Interns 24.8 ± 3.6 31.0 ± 2.1 31.8 ± 1.5 Residents 31.6 ± 3.5 35.5 ± 2.1 33.6 ± 2.7 Senior physicians 32.3 ± 2.8 35.8 ± 2.0 34.7 ± 2.1 Nonradiologists 32.1 ± 3.0 35.6 ± 2.2 34.2 ± 2.7 Radiologists 31.7 ± 3.4 35.8 ± 1.8 34.0 ± 2.3 Overall 30.9 ± 4.0 35.0 ± 2.6 33.8 ± 2.5
Data presented in mean ± standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Mean Sensitivity and Specificity by Level of Expertise and by Specialty by Stages
According to Level of Expertise Session 1 Session 2 Session 3 Interns 52%/71% 72%/83% 81%/78% Residents 72%/86% 84%/93% 78%/90% Senior physicians 73%/87% 84%/95% 80%/93%
According to Medical Specialty Session 1 Session 2 Session 3 Nonradiologists 73%/87% 82%/96% 76%/94% Radiologists 72%/85% 87%/92% 83%/87% Overall 70%/84% 82%/92% 79%/89%
Data presented as sensitivity/specificity in percentage.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Number of Correct Answers for Small-volume Pneumothorax (<20%)
Session 1 Session 2 Session 3 Interns 6.2 ± 1.5 8.8 ± 1.8 10.6 ± 1.1 Residents 9.1 ± 2.5 11.0 ± 1.9 9.9 ± 2.0 Senior physicians 9.5 ± 1.5 10.9 ± 1.3 10.3 ± 2.1 Nonradiologists 9.2 ± 1.8 10.6 ± 1.7 9.5 ± 1.9 Radiologists 9.5 ± 2.4 11.5 ± 1.3 10.8 ± 2.1 Mean 8.9 ± 2.3 10.6 ± 1.8 10.1 ± 2.0
Data presented in mean ± standard deviation.
TABLE 4
Mean Sensitivity and Specificity According to Level of Expertise and Stage Specialty for Small-volume Pneumothorax (<20%)
According to Level of Expertise Session 1 Session 2 Session 3 Interns 47%/71% 63%/83% 76%/78% Residents 71%/86% 79%/93% 71%/90% Senior physicians 75%/87% 78%/95% 73%/93%
According to Medical Specialty Session 1 Session 2 Session 3 Nonradiologists 72%/87% 75%/96% 68%/94% Radiologists 74%/85% 82%/92% 77%/87% Overall 69%/84% 76%/92% 72%/89%
Data for each cell include sensitivity/specificity.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Bobbio A., Dechartres A., Bouam S., et. al.: Spontaneous pneumothorax: epidemiology in France. Eur Respir J [Internet] 2014; 44: Available at: http://erj.ersjournals.com/content/44/Suppl_58/P4116.abstract
2. Gupta D., Hansell A., Nichols T., et. al.: Epidemiology of pneumothorax in England. Thorax 2000; 55: pp. 666-671.
3. Fraser R.G., Hickey N.M., Niklason L.T., et. al.: Calcification in pulmonary nodules: detection with dual-energy digital radiography. Radiology 1986; 160: pp. 595-601.
4. Fischbach F., Freund T., Röttgen R., et. al.: Dual-energy chest radiography with a flat-panel digital detector: revealing calcified chest abnormalities. Am J Roentgenol 2003; 181: pp. 1519-1524.
5. Ricke J., Fischbach F., Freund T., et. al.: Clinical results of CsI-detector-based dual-exposure dual energy in chest radiography. Eur Radiol 2003; 13: pp. 2577-2582.
6. Szucs-Farkas Z., Patak M.A., Yuksel-Hatz S., et. al.: Single-exposure dual-energy subtraction chest radiography: detection of pulmonary nodules and masses in clinical practice. Eur Radiol 2008; 18: pp. 24-31.
7. Manji F., Wang J., Norman G., et. al.: Comparison of dual energy subtraction chest radiography and traditional chest X-rays in the detection of pulmonary nodules. Quant Imaging Med Surg 2016; 6: pp. 1-5.
8. Thelle A., Gjerdevik M., Grydeland T., et. al.: Pneumothorax size measurements on digital chest radiographs: Intra- and inter-rater reliability. Eur J Radiol 2015; 84: pp. 2038-2043.
9. Kelly B.S., Rainford L.A., Darcy S.P., et. al.: The development of expertise in radiology: in chest radiograph interpretation, “expert” search pattern may predate “expert” levels of diagnostic accuracy for pneumothorax identification. Radiology 2016; 280: pp. 252-260.
10. Mehrotra P., Bosemani V., Cox J.: Do radiologists still need to report chest X rays?. Postgrad Med J 2009; 85: pp. 339.
11. Kaufman B., Dhar P., O’Neill D.K., et. al.: Chest radiograph interpretation skills of anesthesiologists. J Cardiothorac Vasc Anesth 2001; 15: pp. 680-683.
12. Eng J., Mysko W.K., Weller G.E.R., et. al.: Interpretation of emergency department radiographs. Am J Roentgenol 2000; 175: pp. 1233-1238.
13. Li F., Engelmann R., Pesce L.L., et. al.: Small lung cancers: improved detection by use of bone suppression imaging—comparison with dual-energy subtraction chest radiography. Radiology 2011; 261: pp. 937-949.
14. Schalekamp S., van Ginneken B., Meiss L., et. al.: Bone suppressed images improve radiologists’ detection performance for pulmonary nodules in chest radiographs. Eur J Radiol 2013; 82: pp. 2399-2405.
15. United States Nuclear Regulatory Commission (U.S.NRC) : Doses in our daily lives [Internet]. Available at: https://www.nrc.gov/about-nrc/radiation/around-us/doses-daily-lives.html#1
16. Institut de Radioprotection et de Sureté Nucléaire (IRSN) : Doses délivrées aux patients en scannographie et en radiologie conventionnelle [Internet]. Available at: http://www.irsn.fr/FR/expertise/rapports_expertise/Documents/radioprotection/IRSN-Rapport-dosimetrie-patient-2010-12.pdf
17. Institut de Radioprotection et de Sureté Nucléaire (IRSN) : Analyse des données relatives à la mise à jour des niveaux de références diagnostiques en radiologie et en médecine nucléaire [Internet]. Available at: http://www.irsn.fr/FR/expertise/rapports_expertise/Documents/radioprotection/IRSN_NRD-Bilan2013-2015-Diagnostic-Medical_201611.pdf