
Rationale and Objectives
The study aimed to determine whether the addition of the Fleischner Society guidelines to chest computed tomography (CT) reports identifying incidental pulmonary nodules affects follow-up care.
Patients and Methods
Beginning in 2008, a template containing the Fleischner Society guidelines was added at the interpreting radiologist’s discretion to chest CT reports describing incidental solid pulmonary nodules at our institution. The records of all medical centers in Olmsted county were used to capture the complete medical history of local patients >35 years old diagnosed with a pulmonary nodule from April 1, 2008 to October 1, 2011. Patients with a history of cancer or previously diagnosed nodule, or who died before follow-up, were excluded. Patients were categorized according to whether they did (“template group”) or did not (“control group”) have the template added. Nodule size and smoking history were used to determine recommended follow-up care. Differences in follow-up were compared between groups using Pearson’s chi-square test.
Results
A total of 510 patients (276 in the template group, 234 in the control group) were included in the study. Only 198 patients (39%) received their recommended follow-up care. Template group patients were significantly more likely to receive recommended follow-up care compared to control group patients (45% vs 31%, P = .0014). Most patients whose management did not adhere to Fleischner Society guidelines did not receive a recommended follow-up chest CT (210 out of 312, 67%).
Conclusions
The addition of the Fleischner Society guidelines to chest CT reports significantly increases the likelihood of receiving recommended follow-up care for patients with incidental pulmonary nodules. Additional education is needed to improve appropriate guideline utilization by radiologists and adherence by ordering providers.
Introduction
Lung cancer accounts for approximately 27% of all cancer deaths and is the leading cause of cancer death among both men and women in the United States . The American Cancer Society estimates 221,200 new cases of lung cancer and 158,040 deaths from lung cancer in 2015 . Patients with stage IA lung cancer have a 5-year survival rate greater than 60%; however, survival rates rapidly decline as the stage of disease increases.
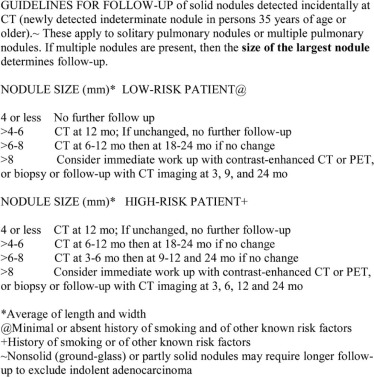
With increasing utilization and improving resolution of computed tomography (CT), growing numbers of noncalcified solid pulmonary nodules are detected. In response to the need for follow-up management of these incidentally found nodules, the Fleischner Society devised a set of evidence-based recommendations in 2005 . These recommendations classify patients at least 35 years old into low- and high-risk groups depending on smoking history, family history of lung cancer, or exposure to asbestos, radon, or uranium. Despite publication of such guidelines, follow-up of solid pulmonary nodules has still been suboptimal. Eisenberg et al. reported only 79% of radiologists were aware of and only 59% of radiology practices employed such guidelines .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patients and Methods
Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Retrieval
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Defining Adherence to Fleischner Guidelines
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
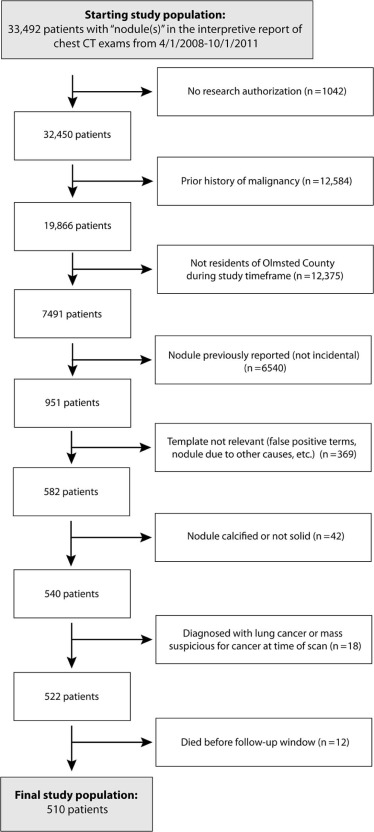
Table 1
Study Demographics
Template Group Control Group_P_ Value_N_ 276 234 Age at CT scan 60(49–72) 64(51–75).0512 Age groups .27 35–49 75(27%) 51(22%) 50–64 86(31%) 71(30%) ≥65 115(42%) 112(48%) Year of scan(median, IQR) 2010(2009–2010) 2009(2008–2010)<.0001 Female sex 135(49%) 121(52%) .53 Past or current smoker(high risk) 143(52%) 124(53%) .79 Solitary nodule reported(vs multiple) 128(46%) 99(42%) .36 Largest nodule size reported .14 ≤4 mm 141(51%) 143(61%) >4–6 mm 86(31%) 55(24%) >6–8 mm 31(11%) 24(10%) >8 mm 18(6.5%) 12(5.1%) CT report read by thoracic radiologist(vs other subspecialty) 182(66%) 82(35%)<.0001 CT scan ordering provider specialty \* .0072 Primary care 95(34%) 58(25%) ED 68(25%) 86(37%) Pulmonary 29(11%) 16(6.8%) Other specialty 84(30%) 74(32%)
CT, computed tomography; IQR, interquartile range; ED, emergency department.
Bolded values indicate significant differences between groups.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Effect of Template on Adherence to Fleischner Guidelines
Template Group Control Group Odds Ratio (95% CI) \* P Value_N_ 276 234 Guidelines followed All patients 125(45%) 73(31%) 1.83(1.27–2.63).0014 By largest reported nodule ≤4 mm 74/141(53%) 59/143(41%) 1.57(0.98–2.51) .07 >4–6 mm 28/86(33%) 6/55(11%) 3.94(1.51–10.3).0043 >6–8 mm 14/31(45%) 3/24(13%) 5.76(1.42–23.4).0172 >8 mm 9/18(50%) 5/12(42%) 1.40(0.32–6.11) .72 By patient risk High risk 53/143(37%) 15/124(12%) 4.28(2.26–8.10)<.0001 Low risk 72/133(54%) 58/110(53%) 1.06(0.64–1.76) .90 By number of nodules reported Solitary nodule 53/128(41%) 32/99(32%) 1.48(0.85–2.56) .16 Multiple nodules 72/148(49%) 41/135(30%) 2.17(1.33–3.54).0017 By patient age 35–49 30/75(40%) 14/51(27%) 1.76(0.82–3.80) .18 50–64 39/86(45%) 24/71(34%) 1.63(0.35–3.11) .19 ≥65 56/115(49%) 35/112(31%) 2.09(1.21–3.59).0099 By initial CT examination ordering provider specialty Primary care 38/95(40%) 27/58(47%) 0.77(0.40–1.48) .50 ED 26/68(38%) 21/65(24%) 1.92(0.96–3.83) .08 Pulmonary 17/29(59%) 5/16(31%) 3.12(0.86–11.3) .12 Other specialty 44/84(52%) 20/74(27%) 2.97(1.52–5.79).0019
CI, confidence interval; CT, computed tomography; ED, emergency department.
Bolded values indicate significant differences between groups.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Types of Nonadherence to Fleischner Guidelines
Template Group Control Group_P_ Value All patients with nonadherent follow-up 151 161.0400 Chest CT not ordered when recommended 100(66%) 110(68%) Chest CT ordered when not recommended 23(15%) 11(6.8%) Chest CT ordered too soon 10(6.6%) 22(14%) Chest CT ordered too late 17(11%) 15(9.3%) Biopsy/PET ordered when not recommended 1(0.7%) 3(1.9%) Largest nodule ≤4 mm 67 84.0137 Chest CT not ordered when recommended 37(55%) 53(63%) Chest CT ordered when not recommended 23(34%) 11(13%) Chest CT ordered too soon 3(4.5%) 12(14%) Chest CT ordered too late 4(6.0%) 7(8.3%) Biopsy/PET ordered when not recommended 0 1(1.2%) Largest nodule >4–6 mm 58 49 .42 Chest CT not ordered when recommended 41(71%) 35(71%) Chest CT ordered when not recommended 0 0 Chest CT ordered too soon 7(12%) 9(18%) Chest CT ordered too late 9(16%) 4(8.2%) Biopsy/PET ordered when not recommended 1(1.7%) 1(2.0%) Largest nodule >6–8 mm 17 21 .52 Chest CT not ordered when recommended 15(88%) 15(71%) Chest CT ordered when not recommended 0 0 Chest CT ordered too soon 0 1(4.8%) Chest CT ordered too late 2(12%) 4(19%) Biopsy/PET ordered when not recommended 0 1(4.8%) Largest nodule >8 mm 9 7 .48 Chest CT not ordered when recommended 7(77%) 7(100%) Chest CT ordered when not recommended 0 0 Chest CT ordered too soon 0 0 Chest CT ordered too late 2(22%) 0 Biopsy/PET ordered when not recommended 0 0
CT, computed tomography; PET, positron emission tomography.
Bolded values indicate significant differences between groups.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Guideline Adherence by Initial Chest CT Examination Ordering Provider Specialty
Primary Care \* ED Pulmonary Other Specialties \* All patients ( n ) 153 154 45 158 Unique ordering providers( n ) 89 37 27 127 Adhered to guidelines(% of all patients) 65(42%) 47(31%) 22(49%) 64(41%) No imaging ordered as recommended(% of adhered) 35(54%) 21(45%) 14(64%) 41(64%) Imaging ordered as recommended 30(46%) 26(55%) 8(36%) 23(36%) Did not adhere to guidelines 88 107 23 94 CT not ordered when recommended(% of nonadhered) 54(61%) 76(71%) 16(70%) 64(68%) CT ordered when not recommended 11(13%) 10(9.4%) 2(8.7%) 11(12%) CT ordered too soon 6(6.8%) 9(8.4%) 3(13%) 11(12%) CT ordered too late 14(16%) 9(8.4%) 2(8.7%) 7(7.5%) Biopsy or PET/CT ordered when not recommended 3(3.4%) 0 0 1(1.1%)
CT, computed tomography; ED, emergency department; PET, positron emission tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Figure S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. American Cancer Society : American Cancer Society: cancer facts and figures 2015.2015.American Cancer Society http://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf
2. MacMahon H., Austin J.H., Gamsu G., et. al.: Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology 2005; 237: pp. 395-400.
3. Eisenberg R.L., Bankier A.A., Boiselle P.M.: Compliance with Fleischner Society guidelines for management of small lung nodules: a survey of 834 radiologists. Radiology 2010; 255: pp. 218-224.
4. Rocca W.A., Yawn B.P., St Sauver J.L., et. al.: History of the Rochester Epidemiology Project: half a century of medical records linkage in a US population. Mayo Clin Proc 2012; 87: pp. 1202-1213.
5. St Sauver J.L., Grossardt B.R., Yawn B.P., et. al.: Data resource profile: the Rochester Epidemiology Project (REP) medical records-linkage system. Int J Epidemiol 2012; 41: pp. 1614-1624.
6. St Sauver J.L., Grossardt B.R., Yawn B.P., et. al.: Use of a medical records linkage system to enumerate a dynamic population over time: the Rochester Epidemiology Project. Am J Epidemiol 2011; 173: pp. 1059-1068.
7. Elias R.M., Sykes A.M., Knudsen J.M., et. al.: Impact of a standardized recommendation and electronic prompts on follow-up of indeterminate pulmonary nodules found on computed tomography. J Pulmonar Respirat Med 2012; 2: pp. 113.
8. Woloshin S., Schwartz L.M., Dann E., et. al.: Using radiology reports to encourage evidence-based practice in the evaluation of small, incidentally detected pulmonary nodules. A preliminary study. Ann Am Thorac Soc 2014; 11: pp. 211-214.
9. Blagev D.P., Lloyd J.F., Conner K., et. al.: Follow-up of incidental pulmonary nodules and the radiology report. J Am Coll Radiol 2014; 11: pp. 378-383.
10. Lacson R., Prevedello L.M., Andriole K.P., et. al.: Factors associated with radiologists’ adherence to Fleischner Society guidelines for management of pulmonary nodules. J Am Coll Radiol 2012; 9: pp. 468-473.
11. Masciocchi M., Wagner B., Lloyd B.: Quality review: Fleischner criteria adherence by radiologists in a large community hospital. J Am Coll Radiol 2012; 9: pp. 336-339.
12. Ridge C.A., Hobbs B.D., Bukoye B.A., et. al.: Incidentally detected lung nodules: clinical predictors of adherence to Fleischner Society surveillance guidelines. J Comput Assist Tomogr 2014; 38: pp. 89-95.
13. Wiener R.S., Gould M.K., Slatore C.G., et. al.: Resource use and guideline concordance in evaluation of pulmonary nodules for cancer: too much and too little care. JAMA Intern Med 2014; 174: pp. 871-880.
14. Lu M.T., Rosman D.A., Wu C.C., et. al.: Radiologist point-of-care clinical decision support and adherence to guidelines for incidental lung nodules. J Am Coll Radiol 2016; 13: pp. 156-162.
15. Murphy D.R., Thomas E.J., Meyer A.N., et. al.: Development and validation of electronic health record-based triggers to detect delays in follow-up of abnormal lung imaging findings. Radiology 2015; 277: pp. 81-87.