
Rationale and Objectives
Annual breast magnetic resonance imaging (MRI) is recommended to screen high-risk populations for breast cancer, although costs are significant. This study assesses the performance of an abbreviated MRI protocol as a resource-efficient approach for screening patients at high-risk of breast cancer, and assesses whether the abbreviated protocol alters the assigned Breast Imaging Reporting and Data System (BI-RADS) category.
Materials and Methods
This is a prospective paired cohort study performed in an academic ambulatory setting. MRI images of women at high risk of breast cancer were reviewed using an abbreviated MRI protocol, followed by an immediate review of additional sequences included in a full diagnostic protocol. BI-RADS assessments, including all changes and interpretation times, were recorded for both the abbreviated and full protocol reviews. Cancer detection rate, positive predictive value 3 (PPV3), sensitivity, and specificity were calculated.
Results
A total of 1052 MRI cases were reviewed. The cancer detection rate was 13.3 per 1000 with a PPV3 of 30.4% based on the full protocol. Review of sequences included in the full protocol resulted in a change in the final BI-RADS assessments in 3.4% of the cases, the majority of which did not change clinical management with respect to biopsy. The sensitivity and specificity of the abbreviated and full protocols were not significantly different.
Conclusions
This pilot study of an abbreviated MRI protocol demonstrates effective performance in cancer detection. BI-RADS assessments were rarely altered with the additional information afforded by the full protocol. The abbreviated protocol holds promise for resource-efficient breast cancer screening in high-risk women.
Introduction
Breast cancer is the most common cancer in women and a significant (or leading) cause of mortality in the United States, with an estimated 40,000 women dying of breast cancer in 2015. The Surveillance, Epidemiology, and End Results program recorded 783,000 life years lost due to breast cancer in 2012, with an average of 19 life years lost per death . High-risk women are even more likely to be impacted by disease-specific mortality; therefore, efforts have been made to supplement routine mammographic screening with additional imaging in this population. “High risk” is defined by the American College of Radiology appropriateness criteria as women with a BRCA gene mutation; a history of chest irradiation between the ages of 10 and 30; genetic syndromes that increase the risk of breast cancer; or an estimated 20% or greater lifetime risk of breast cancer based on family or personal history, history of atypia, or a combination thereof .
Screening mammography leads to early cancer detection and improved survival. The use of mammography alone has been shown to detect approximately 7.6 per 1000 cancers in asymptomatic high-risk women. However, mammographic sensitivity is not ideal and can be as low as 30%–48% in women with dense breast tissue .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Study Design
Get Radiology Tree app to read full this article<
Patient Population
Get Radiology Tree app to read full this article<
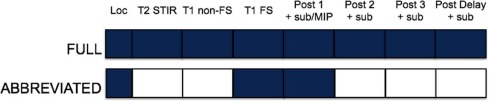
Abbreviated and Full-breast MRI Protocols
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Breast MRI Interpretation
Get Radiology Tree app to read full this article<
Data Collection and Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Screening Breast MRI Indications
Get Radiology Tree app to read full this article<
Additional Time for the Full Protocol
Get Radiology Tree app to read full this article<
CDR and Positive Predictive Value
Get Radiology Tree app to read full this article<
TABLE 1
Histology of Malignant Biopsies ( n = 14)
Histology Number Size (mm) \* Elston Grade † Invasive ductal carcinoma 8 14 2 6 2 8 2 7 1 4 3 10 3 13 3 6 2 Invasive lobular carcinoma 1 10 2 Invasive mammary carcinoma 2 11 2 17 2 Sarcomatoid carcinoma 1 13 3 Ductal carcinoma in situ 2 6 1 25 3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Histology of Benign Biopsies ( n = 35)
Histology Number Benign breast tissue, not otherwise specified 11 Fibroadenoma 10 Fibrocystic change 5 Postsurgical change or fat necrosis 3 Pseudoangiomatous stromal hyperplasia 3 Micropapilloma 2 Hemangioma 1
Get Radiology Tree app to read full this article<
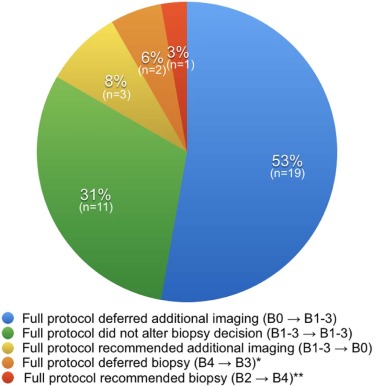
BI-RADS Changes Between the Abbreviated and Full Protocols
Get Radiology Tree app to read full this article<
TABLE 3
Distribution of BI-RADS Assessments ( n = 1052)
 Open full size image
Open full size image
BI-RADS, Breast Imaging Reporting and Data System.
“B” designates BI-RADS assessment category. BI-RADS assessments were grouped into categories that recommended biopsy (B4 and B5), did not recommend biopsy (B1, B2, and B3), or recommended additional imaging (B0). The BI-RADS assessment did not change between the abbreviated and full protocols for shaded cases.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
False-negative Rate, Sensitivity, and Specificity
Get Radiology Tree app to read full this article<
TABLE 4
Diagnostic Indices for Cases with 1-Year Follow-up \*
Abbreviated Protocol ( n = 651) Cancer No Cancer Positive result 9 18 Negative result 2 622
% 95% Confidence Interval Sensitivity 81.8 47.8–96.8 Specificity 97.2 95.5–98.3
Full Protocol ( n = 660) Cancer No Cancer Positive result 9 17 Negative result 2 632
% 95% Confidence Interval Sensitivity 81.8 47.8–96.8 Specificity 97.4 95.8–98.4
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Howlander N., Noone A., Krapcho M., et. al.: SEER cancer statistics review, 1975–2012.2015.National Cancer InstituteBethesda, MD
2. American College of Radiology : Appropriateness criteria. Available at: https://acsearch.acr.org/list Accessed June 18, 2016
3. Kelly K.M., Dean J., Comulada W.S., et. al.: Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol 2010; 20: pp. 734-742.
4. Berg W.A., Blume J.D., Cormack J.B., et. al.: Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA 2008; 299: pp. 2151-2163.
5. Berg W.A., Zhang Z., Lehrer D., et. al.: Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012; 307: pp. 1394-1404.
6. O’Connor M., Rhodes D., Hruska C.: Molecular breast imaging. Expert Rev Anticancer Ther 2009; 9: pp. 1073-1080.
7. Rhodes D.J., Hruska C.B., Conners A.L., et. al.: Journal club: molecular breast imaging at reduced radiation dose for supplemental screening in mammographically dense breasts. AJR Am J Roentgenol 2015; 204: pp. 241-251.
8. Rhodes D.J., Hruska C.B., Phillips S.W., et. al.: Dedicated dual-head gamma imaging for breast cancer screening in women with mammographically dense breasts. Radiology 2011; 258: pp. 106-118.
9. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
10. Kuhl C.K., Schrading S., Strobel K., et. al.: Abbreviated breast magnetic resonance imaging (MRI): first postcontrast subtracted images and maximum-intensity projection-a novel approach to breast cancer screening with MRI. J Clin Oncol 2014; 32: pp. 2304-2310.
11. Grimm L.J., Soo M.S., Yoon S., et. al.: Abbreviated screening protocol for breast MRI: a feasibility study. Acad Radiol 2015; 22: pp. 1157-1162.
12. Mango V.L., Morris E.A., David Dershaw D., et. al.: Abbreviated protocol for breast MRI: are multiple sequences needed for cancer detection?. Eur J Radiol 2015; 84: pp. 65-70.
13. Harvey S.C., Di Carlo P.A., Lee B., et. al.: An abbreviated protocol for high-risk screening breast MRI saves time and resources. J Am Coll Radiol 2016; 4: pp. 374-380.
14. Niell B.L., Gavenonis S.C., Motazedi T., et. al.: Auditing a breast MRI practice: performance measures for screening and diagnostic breast MRI. J Am Coll Radiol 2014; 11: pp. 883-889.