
Rationale and Objectives
Research on communication between radiologists and women undergoing screening and diagnostic mammography is limited. We describe community radiologists’ communication practices with patients regarding screening and diagnostic mammogram results and factors associated with frequency of communication.
Materials and Methods
We received surveys from 257 radiologists (70% of those eligible) about the extent to which they talk to women as part of their health care visit for either screening or diagnostic mammograms, whether this occurs if the exam assessment is positive or negative, and how they use estimates of patient risk to convey information about an abnormal exam where the specific finding of cancer is not yet known. We also assessed characteristics of the radiologists to identify associations with more or less frequent communication at the time of the mammogram.
Results
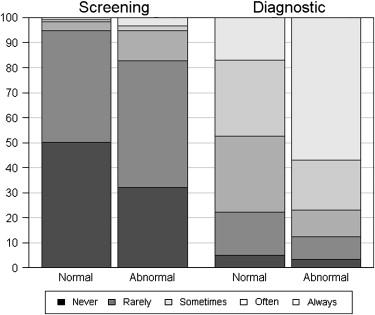
Two hundred and forty-three radiologists provided complete data (95%). Very few (<6%) reported routinely communicating with women when screening mammograms were either normal or abnormal. Fewer than half (47%) routinely communicated with women when their diagnostic mammograms were normal, whereas 77% often or always communicated with women when their diagnostic exams were abnormal. For positive diagnostic exams, female radiologists were more likely to be frequent communicators compared to males (87.1%–72.8%; P = .02) and those who spend 40%–79% of their time in breast imaging (94.6%) were more likely to be frequent communicators compared to those who spend less time (67.2%–78.9%; P = .02). Most radiologists convey risk information using general rather than numeric statements (57.7% vs. 28.5%).
Conclusions
Radiologists are most likely to convey information about diagnostic mammographic findings when results are abnormal. Most radiologists convey risk information using general rather than numeric statements.
Communication is a key aspect of quality health care, because it fosters trust in the physician-patient relationship . Several studies have focused on patient communication in health care in general and in cancer care in general. Overall, there is consensus that physician-patient communication could be improved . For example, patients often leave health care visits confused about the need for further workup and the therapeutic value of what was done at their last procedure . Another study found that a high degree of physician-initiated communication is associated with patients’ perception of having a treatment choice, and higher satisfaction with their cancer care in the 3–6 months after breast surgery .
Though this body of literature is expanding, much less is known about the communication that occurs between radiologists and women undergoing mammography. This is in part due to the fact that the person directly interacting with the patient to obtain the exam is the radiologic technologist rather than the radiologist, but evidence regarding the anxiety women experience when undergoing mammography underscores the need for effective communication. In fact, some research indicates that women experience significant dissatisfaction with the communication they have with radiologists , with one study showing that poor communication between physicians and patients at the time of the mammogram reduced adherence to follow-up examinations . Important limitations exist with the studies conducted on this issue to date, which include assessments done only at academic medical centers and communication that occurs between trainees and patients .
Get Radiology Tree app to read full this article<
Methods
Study Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Radiologist Characteristics
Characteristics_n_ (%) Total 243 (100.0) Demographics Sex Male 173 (71.2) Female 70 (28.8) Practice type Primary affiliation with academic medical center No 196 (81.7) Adjunct 22 (9.2) Primary 22 (9.2) Breast imaging experience Fellowship training No 222 (91.4) Yes 21 (8.6) Years of mammography interpretation <10 51 (21.1) 10–19 89 (36.8) ≥20 102 (42.1) Percent of time spent in breast imaging <20% 61 (25.8) 20%–39% 62 (26.3) 40%–79% 37 (15.7) 80%–100% 76 (32.2) Communication styles Screening exams When Screening exam is normal Infrequent communicator (never/rarely/sometimes) 239 (98.4) Frequent communicator (often/always) 4 (1.6) When screening exam is abnormal Infrequent communicator (never/rarely/sometimes) 230 (94.7) Frequent communicator (often/always) 13 (5.3) Diagnostic exams When diagnostic exam is normal Infrequent communicator (never/rarely/sometimes) 128 (52.7) Frequent communicator (often/always) 115 (47.3) When diagnostic exam is abnormal Infrequent communicator (never/rarely/sometimes) 56 (23.0) Frequent communicator (often/always) 187 (77.0) When discussing positive mammography exams with a patient would you use: Numbers and statistics such as “your chances of having cancer is less than 2%” Never 50 (21.3) Rarely 67 (28.5) Sometimes 51 (21.7) Often 66 (28.1) Always 1 (0.4) General statements such as “your chance of having cancer is extremely low” Never 10 (4.2) Rarely 20 (8.4) Sometimes 71 (29.7) Often 120 (50.2) Always 18 (7.5) Confident in my understanding of numbers and statistics when presenting information on mammography with patients Not at all confident 2 (0.8) Not very confident 9 (3.7) Neutral 41 (16.9) Confident 156 (64.2) Very confident 35 (14.4)
Missing data: Practice type is missing 3 responses; years interpreting mammography is missing 1 response; percent of time spent in breast imaging is missing 7 responses; use of statistics when talking about positive mammograms is missing 8 responses; and use of general statements when talking about positive mammograms is missing 4 responses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Characteristics of Radiologists who Report Being Frequent (vs. Infrequent) Communicators According to Screening and Diagnostic Mammograms and their Interpretations
Screening Exams Diagnostic Exams Normal Abnormal Normal Abnormal_n_ % Frequent Communicators % Frequent Communicators % Frequent Communicators % Frequent Communicators Total 243 1.6 5.3 47.3 77.0 Sex Male 173 1.2 5.2 44.572.8 Female 70 2.9 5.7 54.387.1 Primary affiliation with academic medical center No 196 2.0 6.1 45.9 77.0 Adjunct 22 0.0 0.0 63.6 77.3 Primary 22 0.0 0.0 45.5 77.3 Fellowship training No 222 1.4 5.0 46.4 75.7 Yes 21 4.8 9.5 57.1 90.5 Years of mammography interpretation <10 51 3.9 0.029.4 72.5 10–19 89 1.1 4.550.6 76.4 ≥20 102 1.0 8.853.9 80.4 Percent of time spent in breast imaging <20% 61 0.0 0.0 45.967.2 20%–39% 62 3.2 4.8 46.875.8 40%–79% 37 2.7 2.7 48.694.6 80%–100% 76 1.3 9.2 48.778.9 Confident in understanding numbers and statistics No (not confident to neutral) 52 0.0 1.9 51.9 73.1 Yes (confident to very confident) 191 2.1 6.3 46.1 78.0
Bold indicates a statistically significant difference ( P value < .05) using a chi-square score test from a logistic regression model for the binary outcome of being a frequent communicator.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Communication Content According to Level of Communication of Abnormal Diagnostic Exams and Confidence in Use of Statistics
n and % who are Confident in use of Statistics_n_ and % who are Frequent Communicators of Abnormal Diagnostic Exams_n_ and % who are Frequent Communicators of Abnormal Diagnostic Exams Among those not Confident in use of Statistics Among those Confident in use of Statistics Total n__n (%)n (%)n (%)n (%) Total 243 191 (78.6) 187 (77.0) 38 (73.1) 149 (78.0) When discussing positive mammography exams with a patient would you use: Numbers and statistics such as “your chances of having cancer is less than 2%” Never 50 38 (76.0)30 ( 60.0) 8 (66.7) 22 (57.9) Rarely/sometimes 118 88 (74.6) 96 (81.4) 23 (76.7) 73 (83.0) Often/always 6760 ( 89.6) 59 (88.1) 6 (85.7) 53 (88.3) General statements such as “your chance of having cancer is extremely low”, n (%) Never 10 9 (90.0)2 ( 20.0) 0 (0.0) 2 (22.2) Rarely/sometimes 91 74 (81.3) 72 (79.1) 12 (70.6) 60 (81.1) Often/always 138 105 (76.1) 112 (81.2) 26 (78.8) 86 (81.9)
Missing data: using numbers and statistics, such as “your chance of having cancer is less than 2%” is missing 8 responses. Using general statements such as “your chance of having cancer is extremely low” is missing 4 responses.
Bold indicates a statistically significant difference ( P value < .05) between the responses in a given category and all other categories.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Teutsch C.: Patient-doctor communication. Med Clin North Am 2003; 87: pp. 1115-1145.
2. Lee S.J., Back A.L., Block S.D., et. al.: Enhancing physician-patient communication. Hematology 2002; 464: pp. 83.
3. Simon S.R., Lee T.H., Goldman L., et. al.: Communication problems for patients hospitalized with chest pain. J Gen Intern Med 1998; 13: pp. 836-838.
4. Feldman D.S., Novack D.H., Gracely E.: Effects of managed care on physician-patient relationships, quality of care, and the ethical practice of medicine: a physician survey. Arch Intern Med 1998; 158: pp. 1626-1632.
5. Knopp R., Rosenzweig S., Bernstein E., et. al.: Physician-patient communication in the emergency department, part 1. Acad Emerg Med 1996; 3: pp. 1065-1069.
6. Thorne S.E., Bultz B.D., Baile W.F., SCRN Communication Team: Is there a cost to poor communication in cancer care? A critical review of the literature. Psycho-oncology 2005; 14: pp. 875-884.
7. Schofield P.E., Butow P.N.: Towards better communication in cancer care: a framework for developing evidence-based interventions. Patient Ed Counsel 2004; 55: 32–29
8. Beckman H.B., Frankel R.M.: Training practitioners to communicate effectively in cancer care: it is the relationship that counts. Patient Education & Counseling 2003; 50: pp. 85-89.
9. Kahana E., Kahana B.: Patient proactivity enhancing doctor-patient-family communication in cancer prevention and care among the aged. Patient Ed Counsel 2003; 50: pp. 67-73.
10. Fallowfield L., Jenkins V.: Effective communication skills are the key to good cancer care. Eur J Cancer 1999; 35: pp. 1592-1597.
11. Liang W., Burnett C.B., Rowland J.H., et. al.: Communication between physicians and older women with localized breast cancer: implications for treatment and patient satisfaction. J Clin Oncol 2002; 20: pp. 1008-1016.
12. Padgett D.K., Yedidia M.J., Kerner J., et. al.: The emotional consequences of false positive mammography: African-American women’s reactions in their own words. Women Health 2001; 33: pp. 1-14.
13. Allen J.D., Shelton R.C., Harden E., et. al.: Follow-up of abnormal screening mammograms among low-income ethnically diverse women. Findings from a qualitative study. Patient Ed Counsel 2008; 72: pp. 283-292.
14. Peralman D.N., Rakowski W., Clark M.A., et. al.: Why do women’s attitudes toward mammography change over time? Implications for physician-patient communication. Cancer Epidemiol Biomark Prev 1997; 6: pp. 451-457.
15. Sasson J.P., Zand T., Lown B.A.: Communication in the diagnostic mammography suite: Implications for practice and training. Acad Radiol 2008; 15: pp. 417-424.
16. Carney P.A., Geller B.M., Moffett H., et. al.: Current medico-legal and confidentiality issues in large multi-center research programs. Am J Epidemiol 2000; 152: pp. 371-378.
17. Miglioretti D.L., Smith-Bindman R., Abraham L.A., et. al.: Radiologist characteristics associated with interpretive performance of diagnostic mammography. JNCI 2007; 99: pp. 1854-1863.
18. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/BIRADSAtlas/BIRADSAtlasexcerptedtext/BIRADSMammographyFourthEdition.aspx
19. Priyanath A., Feinglass J., Dolan N.C., et. al.: Patient satisfaction with the communication of mammographic results before and after the Mammographic Quality Standards Reauthorization Act of 1998. AJR Am J Roentgenol 2002; 178: pp. 451-456.
20. Lindfors K.K., O’Connor J., Acredolo C.R., et. al.: Short-interval follow-up mammography versus immediate core biopsy of benign breast lesions: assessment of patient stress. AJR Am J Roentgenol 1998; 171: pp. 55-58.
21. Levin K., Braeuning P., O’Malley M., et. al.: Communicating results of diagnostic mammography: what do patients think?. Acad Radiol 2000; 7: pp. 1069-1076.
22. Schrieiber M., Leonard M., Rieniets C.: Disclosure of imaging findings to patients directly by radiologists: survey of patient’s preferences. AJR Am J Roentgenol 1995; 165: pp. 467-469.
23. Raza S., Rosen M., Chlorny K., et. al.: Patient expectations and costs of immediate reporting of screening mammography. AJR Am J Roentgenol 2001; 177: pp. 579-583.
24. Carney P.A., Abraham L.A., Miglioretti D.L., et. al.: Factors associated with imaging and procedural events used to detect breast cancer following screening mammography. AJR Am J Roentgenol 2007; 188: pp. 385-392.
25. Hopwood P., Howell A., Lalloo F., et. al.: Do women understand the odds? Risk perceptions and recall of high risk information in women with a family history of breast cancer. Commun Genet 2003; 6: 314–223
26. Nekhlyudov L., Partridge A.: Breast cancer risk communication: challenges and future research directions: workshop report. Cancer Causes Contr 2003; 14: pp. 235-239.
27. Royak-Schaler R., Klubunde C.G., Greene W.F., et. al.: Communicating breast cancer risk: patient perceptions of provider discussions. Medscape Women’s Health 2002; 7: pp. 2.