
Rationale and Objective
In 2004, Harvard Medical School initiated a pilot program, the Cambridge Integrated Clerkship, in which students study the core third-year medical disciplines in a longitudinal yearlong experience. In this paper, the authors describe the design of the radiology portion of this program and compare outcomes to those of students in a traditional curriculum.
Materials and Methods
Students in the integrated curriculum were compared to students in traditional clerkships on the basis of Objective Structured Clinical Examination cases, final exams, fourth-year comprehensive exam scores, and choice of specialty.
Results
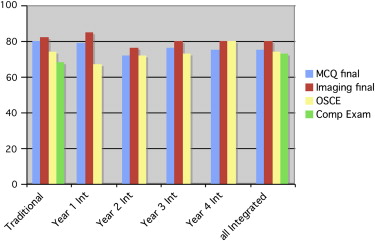
Scores on Objective Structured Clinical Examination cases and imaging final exams were not statistically different between the two groups, but Integrated Clerkship students had statistically lower scores on final exams. Integrated Clerkship students scored higher on the fourth-year radiology comprehensive exam than traditional students, but differences were not statistically significant. Choice of radiology as a specialty was not statistically different between the two groups.
Conclusions
Teaching radiology in an integrated yearlong curriculum is feasible, with a minimal drop in exam scores but no changes in other evaluative measures and no decrease in the choice of radiology as a specialty. The program may give students a better appreciation of the role of radiology in an ambulatory setting and in relationship to other specialties.
Changes in the US health care delivery system, with shortening of hospital stays and a shift toward ambulatory care, have had a negative impact on the educational environment for medical students during many clinical rotations . In the traditional hospital-based intensive-immersion model of clinical education, medical students have less time with patients and fewer substantial duties in patient care, with little emphasis on generalist or primary care skills . Some traditional clerkships have responded by increasing outpatient experiences or changing the proportion of time in acute care environments, but these changes may be difficult depending on the specific practice setting. In an attempt to rethink the way third-year medical students are trained, a pilot program was developed at a teaching hospital with extensive ambulatory sites, Cambridge Health Alliance, a teaching hospital of Harvard Medical School (HMS), that included a major shift away from hospital-based settings as well as integration over a yearlong period of all core disciplines, including radiology .
In this paper, we describe the methodology and evolution of the radiology component of the Cambridge Integrated Clerkship. Preliminary results comparing student outcomes on summative radiology examinations are presented, as well as information on residency selection by students in the traditional clerkship compared to the Integrated Clerkship over the past 4 years. Future plans for the program are also presented, along with a discussion of the limitations of this approach.
Materials and methods
Initial Clerkship Design
Get Radiology Tree app to read full this article<
Table 1
Patients Followed by Students in the Cambridge Integrated Clerkship, Year 4, by Discipline
Student Medicine Neurology Obstetrics/Gynecology Pediatrics Psychiatry Surgery Total ∗ Visits † 1 24 8 7 8 15 12 74 540 2 17 5 10 17 20 5 74 432 3 12 11 10 4 8 4 49 411 4 22 19 8 17 8 18 92 666 5 11 1 3 3 0 2 20 125 6 17 6 6 25 5 8 67 529 7 19 9 9 8 24 7 76 579 8 4 7 5 15 7 11 49 337 9 9 9 9 20 15 9 71 523 10 20 9 5 18 11 13 76 482 11 18 1 10 8 11 14 62 414 Average 15.7 7.7 7.5 13 11.3 9.4 64.5 459
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Introductory Radiology Topics in the Cambridge Integrated Clerkship, Years 1 to 4
Variable Year 1 Year 2 Year 3 Year 4 Total number of sessions 5 5 4 2 Total number of hours 15 14 5 2 Topic list 1. Introduction to chest radiography, plain films 1. Chest radiography, plain films 1. Course organization, chest radiography 1. Course organization, overview of radiology 2. Introduction to CT, KUB 2. KUB, CT, IR 2. CT, MR 2. Basics of image interpretation, terminology 3. Brain and spinal MR and CT 3. Neuroimaging 3. Ultrasound 4. Ultrasound, nuclear medicine 4. Ultrasound, nuclear medicine, abdominal imaging 4. Other areas 5. MSK imaging, trauma, systems and safety 5. MSK imaging, safety
CT, computed tomography; IR, interventional radiology; KUB, kidneys, ureter, and bladder; MR, magnetic resonance; MSK, musculoskeletal.
Table 3
Comparison of Tutorial Topics, Years 1 and 4, in the Cambridge Integrated Clerkship, with Indication of Those That Included Radiology
Variable Year 1 Year 4 Total number of tutorials 43 41 Tutorials with radiology 30 (70%) 29 (71%) Topic list 1. Introduction to small-group learning (smoking cessation) ∗ 1. Understanding clinical research 2. Well child/newborn ∗ 2. Introduction to small-group teaching ∗ 3. Pregnancy ∗ 3. Pediatrics, prevention ∗ 4. Jaundice ∗ 4. Geriatrics 5. Joint pain ∗ 5. Prenatal care ∗ 6. Fever ∗ 6. Adolescence 7. Glomerular disease ∗ 7. Personality disorders 8. Shortness of breath ∗ 8. Lower extremity edema ∗ 9. Somatic symptoms 9. Acute abdominal pain ∗ 10. Confusion 10. Confusion ∗ 11. Headache ∗ 11. Pediatric fever ∗ 12. Low back pain ∗ 12. Pelvic pain ∗ 13. Abnormal vaginal bleeding ∗ 13. Unexplained somatic symptoms 14. Pelvic pain ∗ 14. Shortness of breath ∗ 15. Breast lump ∗ 15. Abnormal uterine bleeding ∗ 16. Lower extremity edema ∗ 16. Headache ∗ 17. Chest pain ∗ 17. Chest pain ∗ 18. Sadness, hopelessness 18. Breast lump ∗ 19. Acute renal failure ∗ 19. Sadness 20. Alcoholism ∗ 20. Pregnancy and its complications ∗ 21. Substance abuse 21. Anxiety, including PTSD 22. Asthma ∗ 22. Fluid and electrolytes 23. COPD ∗ 23. Alcoholism and substance abuse 24. Congestive heart failure ∗ 24. Schizophrenia 25. Pediatric CHF ∗ 25. Diabetes mellitus 26. Depression, anxiety 26. Hypertension ∗ 27. Type 1 diabetes, diabetes in pregnancy ∗ 27. Congestive heart failure ∗ 28. Type 2 diabetes, obesity ∗ 28. HIV ∗ 29. Acid-base balance 29. Colon cancer ∗ 30. Acute abdomen ∗ 30. Pediatric asthma ∗ 31. HIV ∗ 31. Pediatric leukemia 32. Hypertension ∗ 32. Obesity 33. TIA/CVA ∗ 33. Low back pain ∗ 34. Movement disorders 34. Seizure disorders ∗ 35. Schizophrenia 35. Stroke ∗ 36. Potassium balance and management 36. Liver and gallbladder disease ∗ 37. Shock ∗ 37. Renal disease ∗ 38. Anemia ∗ 38. Student directed (4) ∗ 39. Renal function, salt and water management 40. Adolescent behavior 41. Student-led tutorials (3) ∗
CHF, congestive heart failure; chronic obstructive pulmonary disease; CVA, cerebrovascular accident; HIV, human immunodeficiency virus; PTSD, posttraumatic stress disorder; TIA, transient ischemic attack.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Changes in Clerkship Design in Subsequent Years
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison to Traditional Clerkship
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 4
Comparison of the Amount of Time to Teach Radiology per Student, Traditional Clerkship Versus Cambridge Integrated Clerkship
Clerkship Duration of Course (wk) Total Didactic Sessions (h) per Student Total Observation Sessions (h) Total Contact Hours per Year Difference Traditional ∗ 4 40 (60) L 8 (24) 85 1 (1) C Integrated † 49 49 (74) R 2 (6) 114 +34% 30 (30) T 4 (2) O 2 (2) C
C, case report consultation; L, lectures; O, Objective Structured Clinical Examination sessions; R, radiology rounds; T, tutorial.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 5
Comparison of Final Exam Scores, OSCE Scores, and Comprehensive Exam Scores, Traditional Clerkship Versus Cambridge Integrated Clerkship
Variable Cumulated Traditional ‡ Year 1 Integrated Year 2 Integrated Year 3 Integrated Year 4 Integrated Cumulated Integrated ∗ Number of students 205 8 8 11 11 38 Final MCQ exam score 81 ± 7.6, 98/57 79 ± 6.6, 84/64 (.53) 72 ± 5.8, 80/63 (.003) 76 ± 3.7, 82/70 (.001) 75 ± 7, 88/68 (.015) 75 ± 6.1, 88/63 (.00001) Final imaging exam score 82 ± 7.8, 100/60 85 ± 9.3, 98/72 (.34) 76 ± 7.7, 89/67 (.054) 80 ± 6.3, 89/67 (.32) 80 ± 5.2, 89/71 (.16) 80 ± 7.5, 98/67 (.15) OSCE cases † 74 ± 8, 94/54 68 ± 7.9, 82/61 (.05) 72 ± 9.2, 83/57 (.46) 73 ± 6.5, 81/60 (.6) 80 ± 7.7, 88/59 (.05) 74 ± 8.7, 88/57 (.64) Comprehensive exam, radiology § 68 ± 18.5, 100/5 N/A N/A N/A N/A 72 ± 20.3, 100/10 (.37)
MCQ, multiple-choice-question; N/A, not available; OSCE, Objective Structured Clinical Examination.
Data are expressed as mean ± standard deviation, maximum/minimum ( P value). P values compare each year of Integrated Clerkship students and the cumulated total of Integrated Clerkship students with the cumulated traditional clerkship students.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Irby D.M.: Educational continuity in clinical clerkships. N Engl J Med 2007; 356: pp. 856-857.
2. Watson R.T.: Rediscovering the medical school. Acad Med 2003; 78: pp. 659-665.
3. Christakis D.A., Feudtner C.: Temporary matters. The ethical consequences of transient social relationships in medical training. JAMA 1997; 278: pp. 739-743.
4. Whitcomb M.E.: Redesigning clinical education: A major challenge for academic health centers. Acad Med 2005; 80: pp. 615-616.
5. Rivo M.L.: With conviction, commitment and creativity: promoting generalism and the preparation of the generalist physician. Acad Med 2001; 76: pp. S3-S4.
6. Hirsh D., Gutterson W., Batalden M., et. al.: The Harvard Medical School Cambridge Integrated Clerkship. J Gen Intern Med 2006; 21: pp. 180.
7. Ogur B., Hirsh D., Krupat E., Bor D.: The Harvard Medical School-Cambridge Integrated Clerkship: an innovative model of clinical education. Acad Med 2007; 82: pp. 397-404.
8. Hirsh D.A., Ogur B.R., Thibault G.E., Cox M.: Continuity as an organizing principle for clinical education reform. N Engl J Med 2007; 356: pp. 858-866.
9. Cohen P.A., Hirsh D.A., Ogur B.R., Elvin D.M., Antam A.M., Bor D.H.: A novel year-long learner centered tutorial for third-year medical students. J Gen Intern Med 2005; 20: pp. S26-S27.
10. Elvin D.M., Hirsh D.A., Ogur B.R., Cohen P.A., Bor D.H.: Teaching translation: formally incorporating basic science into a third-year medical school curriculum reinforces lessons learned. J Gen Intern Med 2005; 20: pp. S38.
11. Dornan T.: Osler, Flexner, apprenticeship and “the new medical education.”. J R Soc Med 2005; 98: pp. 91-95.
12. Cooke M., Irby D.M., Sullivan W., Ludmerer K.M.: American medical education 100 years after the Flexner report. N Engl J Med 2006; 355: pp. 1339-1344.
13. Flexner A.: Medical education in the United States and Canada. From the Carnegie Foundation for the Advancement of Teaching, bulletin number four,1910. Bull World Health Organ 2002; 80: pp. 594-602.
14. Taylor D., Miflin B.: Problem-based learning: where are we now?. Med Teach 2008; 30: pp. 742-763.
15. Thurley P., Dennick R.: Problem-based learning and radiology. Clin Radiol 2008; 63: pp. 623-628.
16. Jones R.W.: Problem-based learning: description, advantages, disadvantages, scenarios and facilitation. Anaesth Intensive Care 2006; 34: pp. 485-488.
17. Gunderman R., Wood B.: Trusting the student: learner-centered education. J Am Coll Radiol 2004; 1: pp. 897-900.
18. Glick T.H., Moore G.T.: Time to learn: the outlook for renewal of patient-centered education in the digital age. Med Educ 2001; 35: pp. 505-509.
19. Hoffman K.G., Donaldson J.F.: Contextual tensions of the clinical environment and their influence on teaching and learning. Med Educ 2004; 38: pp. 448-454.
20. Shore W.B., Irvine C.: The Interdisciplinary Generalist Curriculum Project at the University of California, San Francisco. Acad Med 2001; 76: pp. S109-S111.
21. Commonwealth Fund: 2003.Commonwealth FundNew York
22. Institute of Medicine: 2003.Institute of MedicineWashington, DC
23. Hansen L.A., Talley R.C.: South Dakota’s third-year program of integrated clerkships in ambulatory-care settings. Acad Med 1992; 67: pp. 817-819.
24. Halaas G.W.: The Rural Physician Associate Program: successful outcomes in primary care and rural practice. Rural Remote Health 2005; 5: pp. 453.
25. Lewin L.O., Papp K.K., Hodder S.L., et. al.: Performance of third-year primary-care-track students in an integrated curriculum at Case Western Reserve University. Acad Med 1999; 74: pp. S82-S89.
26. Mihalynuk T., Bates J., Page G., Fraser J.: Student learning experiences in a longitudinal clerkship programme. Med Educ 2008; 42: pp. 729-732.
27. Schauer R.W., Schieve D.: Performance of medical students in a nontraditional rural clinical program, 1998-1999. Acad Med 2006; 81: pp. 603-607.
28. Oswald N., Alderson T., Jones S.: Evaluating primary care as a base for medical education: the report of the Cambridge community-based clinical course. Med Educ 2001; 35: pp. 782-788.
29. Worley P., Silagy C., Prideaux D., Newble D., Jones A.: The parallel rural community curriculum: an integrated clinical curriculum based in rural general practice. Med Educ 2000; 34: pp. 558-565.
30. Rabinowitz H.K., Babbott D., Bastacky S., et. al.: Innovative approaches to educating medical students for practice in a changing health care environment: the National UME-21 project. Acad Med 2001; 76: pp. 587-597.
31. Blue A.V., Griffith C.H., Stratton T.D., et. al.: Evaluation of students’ learning in an interdisciplinary medicine-surgery clerkship. Acad Med 1998; 73: pp. 806-808.
32. Pipas C.F., Peltier D.A., Fall L.H., et. al.: Collaborating to integrate curriculum in primary care medical education: successes and challenges from three US medical schools. Fam Med 2004; 36: pp. S126-S132.
33. Roberts L.W., Franchini G., Fielder K.: An integrated psychiatry-neurology clerkship within a problem-based learning curriculum. Acad Med 1997; 72: pp. 423-424.
34. Lowitt N.R.: Assessment of an integrated curriculum in radiology. Acad Med 2002; 77: pp. 933.
35. Chew F.S.: Distributed radiology clerkship for the core clinical year of medical school. Acad Med 2002; 77: pp. 1162-1163.
36. Muller J.H., Jain S., et. al.: Lessons learned about integrating a medical school curriculum: perceptions of students, faculty and curriculum leaders. Med Educ 2008; 42: pp. 778-785.
37. Worley P., Prideaux D., Strasser R., Magarey A., March R.: Empirical evidence for symbiotic medical education: a comparative analysis of community- and tertiary-based programmes. Med Educ 2006; 40: pp. 109-116.
38. Kohli E., Ptak J., Smith R., et. al.: Variability in the Hawthorne effect with regard to hand hygiene performance in high- and low-performing inpatient care units. Infect Control Hosp Epidemiol 2009; 30: pp. 222-225.