
In medicine, an eponym is a word—typically referring to an anatomic structure, disease, or syndrome—that is derived from a person’s name. Medical eponyms are ubiquitous and numerous. They are also at times controversial. Eponyms reflect medicine’s rich and colorful history and can be useful for concisely conveying complex concepts. Familiarity with eponyms facilitates correct usage and accurate communication. In this article, 22 eponyms used to describe anatomic structures of the head and neck are discussed. For each structure, the author first provides a biographical account of the individual for whom the structure is named. An anatomic description and brief discussion of the structure’s clinical relevance follow.
Introduction
During the interpretation of cross-sectional studies of the temporal bone, sinuses, skull base, and neck, the radiologist assesses dozens of eponymous anatomic structures, while possibly knowing nothing of the individuals for whom the structures are named. As our understanding of the anatomy of the head and neck and our imaging capabilities continue to improve with the passage of time, we also become more distantly removed from and frequently less familiar with the lives of those historic individuals whose prior work has helped build the foundation of modern medical science. Eponyms honor some of these individuals, most of whom led fascinating lives.
Although the reasons for which eponyms remain controversial are well documented , eponyms remain commonplace as a means to concisely convey complex concepts. Additionally, eponyms can add color to what at times is a dry science. Familiarity with eponyms facilitates correct usage and accurate communication.
Several articles have previously been published in the radiology literature on musculoskeletal , gastrointestinal , cardiothoracic , and vascular eponyms , and earlier work has discussed eponymous diseases of the head and neck . Although a recently published article has given attention to eponymous neuroanatomic structures of the brain, cerebral vasculature, and calvarium , no previous work specifically intended for radiologists has focused on eponymous anatomic structures of the head and neck.
In this article, 22 eponyms used to describe anatomic structures of the head and neck are discussed. For each structure, the author first provides a biographical account of the individual for whom the structure is named. An anatomic description and brief discussion of the structure’s clinical relevance follow.
Temporal Bone
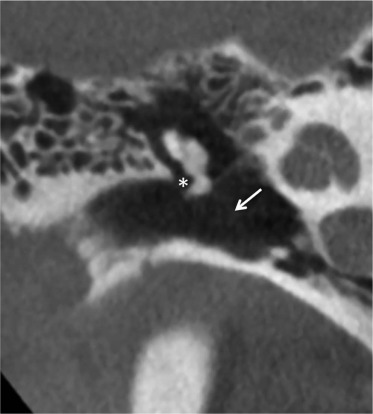
Arnold’s Nerve
Friedrich Arnold (1803–1890) was born in Edenkoben in the German state of Rhine-Palatinate and studied medicine at Heidelberg from 1821 to 1825 . Upon graduation, Arnold accepted a position at the Heidelberg Institute of Anatomy , where he stayed until accepting an appointment at the University of Zurich in 1834 . Arnold subsequently held faculty positions in Freiburg and Tubingen before ultimately returning to Heidelberg as full professor of anatomy and physiology in 1852, where he stayed until his retirement in 1873 . Considered one of the greatest and most accurate anatomic dissectors of his time , Arnold was the first to describe the auricular branch of the vagus nerve , the petrous temporal bone canal through which the nerve passes, and the otic ganglion, all of which bear his name . Arnold died in Heidelberg at age 87 .
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Bill’s Bar
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Fallopian Canal
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
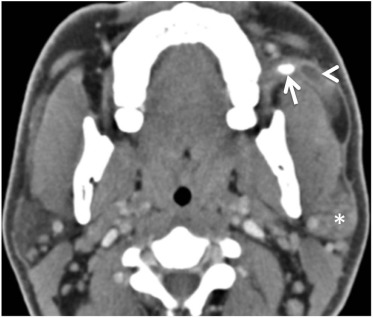
Jacobson’s Nerve
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Prussak’s Space
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Shrapnell’s Membrane
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
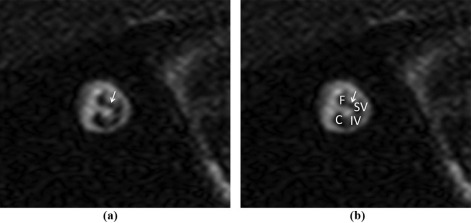
Nervus Intermedius of Wrisberg
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Upper Aerodigestive Tract and Salivary Glands
Eustachian Tubes
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
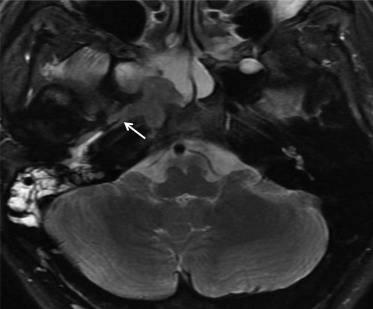
Fossa of Rosenmüller
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Node of Rouvière
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Stensen’s Duct
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Waldeyer’s Ring
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Wharton’s Duct
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Central Skull Base
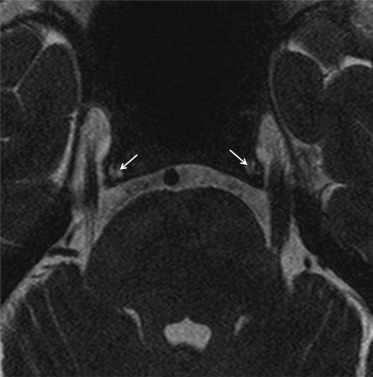
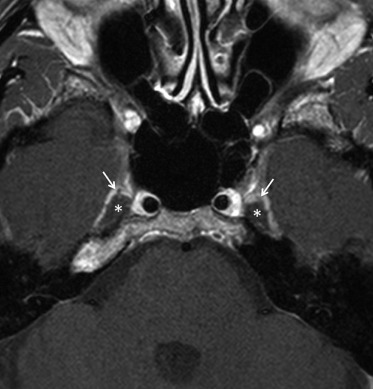
Dorello’s Canal
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Gasserian Ganglion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Meckel’s Cave
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
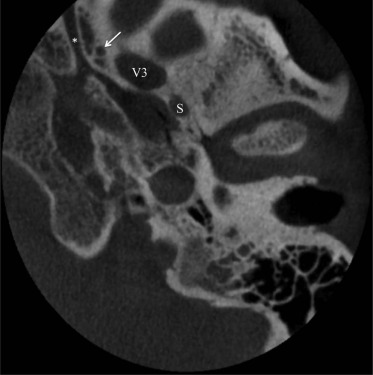
Foramen of Vesalius
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Vidian Canal
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Sinus
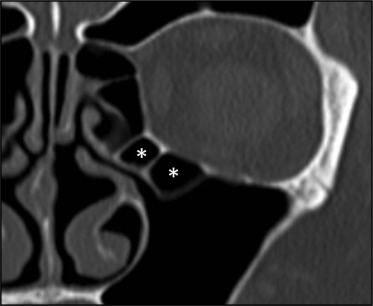
Haller Cell
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Onodi Cell
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Thyroid
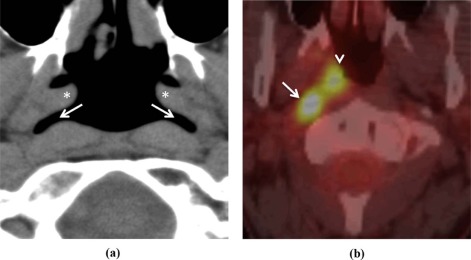
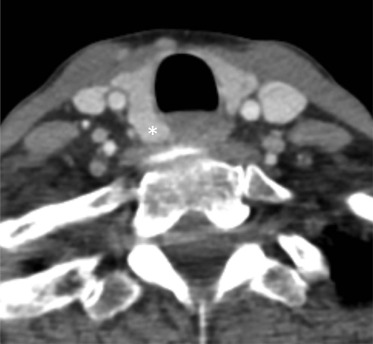
Zuckerkandl’s Tubercle
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Orbit
Annulus of Zinn
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Woywodt A., Matteson E.: Should eponyms be abandoned? Yes. BMJ 2007; 335: pp. 424.
2. Whitworth J.A.: Should eponyms be abandoned? No. BMJ 2007; 335: pp. 425.
3. Harper P.S.: Naming of syndromes and unethical activities: the case of Hallervorden and Spatz. Lancet 1996; 348: pp. 1224-1225.
4. Woywodt A., Haubitz M., Haller H., et. al.: Wegener’s granulomatosis. Lancet 2006; 367: pp. 1362-1366.
5. Wallace D.J., Weisman M.: Should a war criminal be rewarded with eponymous distinction?: the double life of Hans Reiter (1881–1969). J Clin Rheumatol 2000; 6: pp. 49-54.
6. Bunch P.M., Zamani A.A.: Anatomic eponyms in neuroradiology: brain, cerebral vasculature, and calvarium. Acad Radiol 2016; 23: pp. 730-742.
7. Viteri Jusué A., Eguidazu Elosua J.M., Castillo de Juan J., et. al.: Eponyms in musculoskeletal radiology: stories of bones, persons, and civilizations. Radiología 2014; 56: pp. 463-471.
8. Hwang S., Schneider R.: Eponyms of tumors and tumor-like lesions in the musculoskeletal system: who were the people and what are the lesions? Pictorial review. AJR Am J Roentgenol 2010; 195: pp. S50-S61. Quiz S62
9. Hunter T.B., Peltier L.F., Lund P.J.: Radiologic history exhibit. Musculoskeletal eponyms: who are those guys?. Radiographics 2000; 20: pp. 819-836.
10. Kanne J.P., Rohrmann C.A., Lichtenstein J.E.: Eponyms in radiology of the digestive tract: historical perspectives and imaging appearances. Part I. Pharynx, esophagus, stomach, and intestine. Radiographics 2006; 26: pp. 129-142.
11. Kanne J.P., Rohrmann C.A., Lichtenstein J.E.: Eponyms in radiology of the digestive tract: historical perspectives and imaging appearances. Part 2. Liver, biliary system, pancreas, peritoneum, and systemic disease. Radiographics 2006; 26: pp. 465-480.
12. Mohammed T.-L.H., Saettele M.R., Saettele T., et. al.: Eponyms in cardiothoracic radiology: part I. Neoplasms. Curr Probl Diagn Radiol 2014; 43: pp. 91-98.
13. Mohammed T.-L.H., Saettele M.R., Saettele T., et. al.: Eponyms in cardiothoracic radiology—part II: vascular. Curr Probl Diagn Radiol 2014; 43: pp. 219-226.
14. Mohammed T.-L.H., Saettele M.R., Saettele T., et. al.: Eponyms in cardiothoracic radiology: part III—interstitium. Curr Probl Diagn Radiol 2014; 43: pp. 285-293.
15. DiPoce J., Jimenez G., Weintraub J.: Historical perspective: eponyms of vascular radiology. Radiographics 2014; 34: pp. 1120-1140.
16. Hoang J.K., Eastwood J.D., Glastonbury C.M.: What’s in a name? Eponyms in head and neck imaging. Clin Radiol 2010; 65: pp. 237-245.
17. Lekakis G.K.: Philipp Friedrich Arnold, Ludvig Levin Jacobson and their contribution to head and neck anatomy. J Laryngol Otol 2003; 117: pp. 28-31.
18. Lustig L.R., Jackler R.K., Mandelcorn R.: The history of otology through its eponyms I: anatomy. Am J Otol 1998; 19: pp. 371-389.
19. Arnold F.: Icones nervorum capitis.1834.Sumptibus auctorisHeidelberg
20. Som P.M., Smoker W.R., Reidenberg J.S., et. al.: Embryology and anatomy of the neck.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 2117-2163.
21. Gupta D., Verma S., Vishwakarma S.K.: Anatomic basis of Arnold’s ear-cough reflex. Surg Radiol Anat 1986; 8: pp. 217-220.
22. Swartz J.D., Kang M.D.: Trauma to the temporal bone.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1167-1182.
23. Juliano A.F., Maya M.M., Lo W.W., et. al.: Temporal bone tumors and cerebellopontine angle lesions.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1263-1408.
24. Chen R.C., Khorsandi A.S., Shatzkes D.R., et. al.: The radiology of referred otalgia. AJNR Am J Neuroradiol 2009; 30: pp. 1817-1823.
25. Tekdemir I., Aslan A., Elhan A.: A clinico-anatomic study of the auricular branch of the vagus nerve and Arnold’s ear-cough reflex. Surg Radiol Anat 1998; 20: pp. 253-257.
26. Berliner K.I.: In memoriam: William F. House, D.D.S., M.D., the “father of neurotology” 1923–2012. Otol Neurotol 2013; 34: pp. 386-387.
27. Martin D.: Dr. William F. House, inventor of pioneering ear-implant device, dies at 89.2012.
28. Gopen Q., Yang I.: Skull base. Fundam Otol Pediatr Adult Pract 2013; pp. 205-236. Jaypee Brothers, New Delhi
29. Woo E.: Dr. William F. House dies at 89; championed cochlear implant.2012.
30. Eisenberg L.S.: The contributions of William F. House to the field of implantable auditory devices. Hear Res 2015; 322: pp. 52-56.
31. House W.F.: Transtemporal bone microsurgical removal of acoustic neuromas. Report of cases. Arch Otolaryngol 1964; 80: pp. 617-667.
32. Juliano A.F., Ginat D.T., Moonis G.: Imaging review of the temporal bone: part I. Anatomy and inflammatory and neoplastic processes. Radiology 2013; 269: pp. 17-33.
33. Mortazavi M.M., Latif B., Verma K., et. al.: The fallopian canal: a comprehensive review and proposal of a new classification. Childs Nerv Syst 2014; 30: pp. 387-395.
34. Mortazavi M.M., Adeeb N., Latif B., et. al.: Gabriele Fallopio (1523–1562) and his contributions to the development of medicine and anatomy. Childs Nerv Syst 2013; 29: pp. 877-880.
35. Macchi V., Porzionato A., Morra A., et. al.: Gabriel Fallopius (1523–1562) and the facial canal. Clin Anat 2014; 27: pp. 4-9.
36. Fallopio G.: Observationes anatomicae.1561.M.A. UlmusVenice
37. Skadorwa T., Maślanka M., Ciszek B.: The morphology and morphometry of the fetal fallopian canal: a microtomographic study. Surg Radiol Anat 2015; 37: pp. 677-684.
38. Barnes G., Liang J.N., Michaels L., et. al.: Development of the fallopian canal in humans: a morphologic and radiologic study. Otol Neurotol 2001; 22: pp. 931-937.
39. Perez B., Campos M.E., Rivero J., et. al.: Incidence of dehiscences in the fallopian canal. Int J Pediatr Otorhinolaryngol 1997; 40: pp. 51-60.
40. Di Martino E., Sellhaus B., Haensel J., et. al.: Fallopian canal dehiscences: a survey of clinical and anatomical findings. Eur Arch Otorhinolaryngol 2005; 262: pp. 120-126.
41. Kefalidis G., Riga M., Argyropoulou P., et. al.: Is the width of the labyrinthine portion of the fallopian tube implicated in the pathophysiology of Bell’s palsy?: a prospective clinical study using computed tomography. Laryngoscope 2010; 120: pp. 1203-1207.
42. Jacobson L., Trotier D., Døving K.B.: Anatomical description of a new organ in the nose of domesticated animals by Ludvig Jacobson (1813). Chem Senses 1998; 23: pp. 743-754.
43. Fehrenbach M.J., Herring S.W., Thomas P.: Illustrated anatomy of the head and neck.3rd ed.2007.Saunders ElsevierSt. Louis, Mo
44. Goravalingappa R.: Cochlear implant electrode insertion: Jacobson’s nerve, a useful anatomical landmark. Indian J Otolaryngol Head Neck Surg 2002; 54: pp. 70-73.
45. Tekdemir I., Aslan A., Tüccar E., et. al.: An anatomical study of the tympanic branch of the glossopharyngeal nerve (nerve of Jacobson). Ann Anat 1998; 180: pp. 349-352.
46. Todd N.W.: Jacobson’s nerve clues to the round window niche. Cochlear Implants Int 2009; 10: pp. 63-69.
47. Effler L.: The space of Prussak.Effler L.Eponyms anat.1935.McManus-Troup Co.Toledo, OH:pp. 228-230.
48. Palva T., Ramsay H., Böhling T.: Prussak’s space revisited. Am J Otol 1996; 17: pp. 512-520.
49. Prussak A.: Zur Anatomie des menschlichen Trommelfells. Arch Ohrenheilkd 1867; 3: pp. 255-280.
50. Marchioni D., Alicandri-Ciufelli M., Grammatica A., et. al.: Lateral endoscopic approach to epitympanic diaphragm and Prussak’s space: a dissection study. Surg Radiol Anat 2010; 32: pp. 843-852.
51. Baráth K., Huber A.M., Stämpfli P., et. al.: Neuroradiology of cholesteatomas. AJNR Am J Neuroradiol 2011; 32: pp. 221-229.
52. Jackler R.K.: The surgical anatomy of cholesteatoma. Otolaryngol Clin North Am 1989; 22: pp. 883-896.
53. McGovern F.H.: The elusive Henry Jones Shrapnell. Laryngoscope 1983; 93: pp. 903-905.
54. Shrapnell H.: On the form and structure of the membrana tympani. Lond Med Gaz 1832; X: pp. 120-124.
55. Curtin H.D., Gupta R., Bergeron R.T.: Embryology, anatomy, and imaging of the temporal bone.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1053-1096.
56. Luers J.C., Hüttenbrink K.-B.: Surgical anatomy and pathology of the middle ear. J Anat 2016; 228: pp. 338-353.
57. Tubbs R.S., Padmalayam D., Shoja M.M., et. al.: Heinrich August Wrisberg (1736–1808): physician and anatomist. Clin Anat 2014; 27: pp. 10-13.
58. Wrisberg H.: Observationes anatomicae de quinto pare nervorum encephali.1777.Johann Christian DieterichGöttingen
59. Alcaraz N., King W.A., Wackym P.A.: Endoscopy during neurotomy of the nervus intermedius for geniculate neuralgia. Otolaryngol Head Neck Surg 1999; 121: pp. 334-335.
60. Lobko P.I., Khil’kevich S.I.: The intermediate nerve system. Morfol St Petersburg Russ 1992; 102: pp. 42-50.
61. Alfieri A., Strauss C., Prell J., et. al.: History of the nervus intermedius of Wrisberg. Ann Anat 2010; 192: pp. 139-144.
62. Ashram Y.A., Jackler R.K., Pitts L.H., et. al.: Intraoperative electrophysiologic identification of the nervus intermedius. Otol Neurotol 2005; 26: pp. 274-279.
63. Alfieri A., Rampp S., Strauss C., et. al.: The relationship between nervus intermedius anatomy, ultrastructure, electrophysiology, and clinical function. Usefulness in cerebellopontine microsurgery. Acta Neurochir (Wien) 2014; 156: pp. 403-408.
64. Burmeister H.P., Baltzer P.A., Dietzel M., et. al.: Identification of the nervus intermedius using 3T MR imaging. AJNR Am J Neuroradiol 2011; 32: pp. 460-464.
65. Mezzogiorno A., Mezzogiorno V.: Bartolomeo Eustachio: a pioneer in morphological studies of the kidney. Am J Nephrol 1999; 19: pp. 193-198.
66. Hilloowala R.: Bartolomeo Eustachio: his influence on Albinus and the anatomical models at La Specola, Florence. J Hist Med Allied Sci 1986; 41: pp. 442-462.
67. Eustachio B.: Epistola de auditus organis.1563.
68. Codellas P.S.: Alcmaeon of Croton: his life, work, and fragments. Proc R Soc Med 1932; 25: pp. 1041-1046.
69. Effler L.: The tubes of eustachius.Effler L.Eponyms anat.1935.McManus-Troup Co.Toledo, OH:pp. 77-79.
70. Swartz J.D., Hagiwara M.: Inflammatory disease of the temporal bone.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1183-1230.
71. Smoker W.R., Som P.M.: Anatomy and imaging of the oral cavity and pharynx.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1617-1642.
72. Sato H., Kurata K., Yen Y.H., et. al.: Extension of nasopharyngeal carcinoma and otitis media with effusion. Arch Otolaryngol Head Neck Surg 1988; 114: pp. 866-867.
73. Amene C., Cosetti M., Ambekar S., et. al.: Johann Christian Rosenmüller (1771–1820): a historical perspective on the man behind the fossa. J Neurol Surg B Skull Base 2013; 74: pp. 187-193.
74. Rosenmüller J.C.: Handbuch der Anatomie: nach Lebers Umriss der Zergliederungskunst zum Gebrauch der Vorlesungen.1808.KoehlerLeipzig
75. Gunn G.B., Debnam J.M., Fuller C.D., et. al.: The impact of radiographic retropharyngeal adenopathy in oropharyngeal cancer. Cancer 2013; 119: pp. 3162-3169.
76. Loh L.E., Chee T.S., John A.B.: The anatomy of the Fossa of Rosenmuller—its possible influence on the detection of occult nasopharyngeal carcinoma. Singapore Med J 1991; 32: pp. 154-155.
77. Wiegerinck J.I., Somford M.P., Hoornenborg D., et. al.: Eponyms of the Kager triangle. J Bone Joint Surg Am 2012; 94: pp. e67.
78. Rouvière H.: Anatomie des lymphatiques de l’homme.1932.Masson & CieParis
79. Tang L., Li L., Mao Y., et. al.: Retropharyngeal lymph node metastasis in nasopharyngeal carcinoma detected by magnetic resonance imaging: prognostic value and staging categories. Cancer 2008; 113: pp. 347-354.
80. Chua D.T., Sham J.S., Kwong D.L., et. al.: Retropharyngeal lymphadenopathy in patients with nasopharyngeal carcinoma: a computed tomography-based study. Cancer 1997; 79: pp. 869-877.
81. Li Y.-Z., Xie C.-M., Wu Y.-P., et. al.: Nasopharyngeal carcinoma patients with retropharyngeal lymph node metastases: a minimum axial diameter of 6 mm is a more accurate prognostic predictor than 5 mm. AJR Am J Roentgenol 2015; 204: pp. 20-23.
82. Som P.M., Brandwein-Gensler M.S.: Lymph nodes of the neck.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 2287-2384.
83. Zhang G.-Y., Liu L.-Z., Wei W.-H., et. al.: Radiologic criteria of retropharyngeal lymph node metastasis in nasopharyngeal carcinoma treated with radiation therapy. Radiology 2010; 255: pp. 605-612.
84. Perrini P., Lanzino G., Parenti G.F.: Niels Stensen (1638–1686): scientist, neuroanatomist, and saint. Neurosurgery 2010; 67: pp. 3-9. discussion 9
85. Kermit H.: Niels Stensen: the scientist who was beatified.2003.Antony Rowe Ltd.Eastbourne, East Sussex
86. Fazio S.B., Emerick K.: Salivary gland stones.2015.
87. Snell R.S.: The head and neck.Clinical anatomy.2004.Lippincott Williams & WilkinsPhiladelphia:pp. 719-922.
88. Huoh K.C., Eisele D.W.: Etiologic factors in sialolithiasis. Otolaryngol Head Neck Surg 2011; 145: pp. 935-939.
89. Thompson L.D.R.: Salivary duct carcinoma. Ear Nose Throat J 2012; 91: pp. 359.
90. Winkelmann A.: Wilhelm von Waldeyer-Hartz (1836–1921): an anatomist who left his mark. Clin Anat 2007; 20: pp. 231-234.
91. Waldeyer W.: Ueber den lymphatischen Apparat des Pharynx. Dtsch Med Wochenschr 1884; 10: pp. 313.
92. Virchow H.: Die Hände von Wilhelm von Waldeyer-Hartz. Z Anat Entwicklungsgesch 1923; 68: pp. 1-18.
93. Regauer S.: Nasopharynx and Waldeyer’s ring.Cardesa A.Slootweg P.Pathol. Head Neck 17 Tables.2006.SpringerBerlin; Heidelberg; New York:pp. 171-195.
94. Friedman E., Robson C., Hudgins P.A.: Pediatric airway disease.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 1811-1904.
95. Speert H.: Obstetric-gynecologic eponyms; Thomas Wharton and the jelly of the umbilical cord. Obstet Gynecol 1956; 8: pp. 380-382.
96. Som P.M., Brandwein-Gensler M.S.: Anatomy and pathology of the salivary glands.Som P.M.Curtin H.D.Head neck imaging.2011.MosbySt. Louis:pp. 2449-2610.
97. Felisati D., Sperati G.: Gradenigo’s syndrome and Dorello’s canal. Acta Otorhinolaryngol Ital 2009; 29: pp. 169-172.
98. Ambekar S., Sonig A., Nanda A.: Dorello’s canal and Gruber’s ligament: historical perspective. J Neurol Surg B Skull Base 2012; 73: pp. 430-433.
99. Dorello P.: Considerazioni sopra la causa della paralisi transitoria dell’ abducente nelle flogosi dell’ orecchio medio.Ferreri G.Atti della Clinica Oto-Rino-Laringoiatrica.1905.pp. 209-217. Roma
100. Gradenigo G.: Über die paralyse des nervus abducens bei otitis. Arch Ohrenheilk 1907; 774: pp. 149-187.
101. Reddy R.K., Reddy R.K., Jyung R.W., et. al.: Gruber, Gradenigo, Dorello, and Vail: key personalities in the historical evolution and modern-day understanding of Dorello’s canal. J Neurosurg 2015; 124: pp. 224-233.
102. Umansky F., Elidan J., Valarezo A.: Dorello’s canal: a microanatomical study. J Neurosurg 1991; 75: pp. 294-298.
103. Lee K.Y., Kim S.M., Kim D.I.: Isolated bilateral abducens nerve palsy due to carotid cavernous dural arteriovenous fistula. Yonsei Med J 1998; 39: pp. 283-286.
104. Galetta S.L., Smith J.L.: Chronic isolated sixth nerve palsies. Arch Neurol 1989; 46: pp. 79-82.
105. Sonig A., Thakur J., Grass M., et. al.: Antonius Balthazar Raymundus Hirsch and the peregrination of “gasserian ganglion”. J Neurosurg 2013; 119: pp. 778-784.
106. Hirsch A., Gasser J.: Paris quinti nervorum encephali disquisitio anatomica.1765.
107. Gonella M.C., Fischbein N.J., So Y.T.: Disorders of the trigeminal system. Semin Neurol 2009; 29: pp. 36-44.
108. Downs D.M., Damiano T.R., Rubinstein D.: Gasserian ganglion: appearance on contrast-enhanced MR. AJNR Am J Neuroradiol 1996; 17: pp. 237-241.
109. Yousry I., Moriggl B., Schmid U.D., et. al.: Trigeminal ganglion and its divisions: detailed anatomic MR imaging with contrast-enhanced 3D constructive interference in the steady state sequences. AJNR Am J Neuroradiol 2005; 26: pp. 1128-1135.
110. Verjans G.M.G.M., Hintzen R.Q., van Dun J.M., et. al.: Selective retention of herpes simplex virus-specific T cells in latently infected human trigeminal ganglia. Proc Natl Acad Sci USA 2007; 104: pp. 3496-3501.
111. Sanders M., Henny C.P.: Results of selective percutaneous controlled radiofrequency lesion for treatment of trigeminal neuralgia in 240 patients. Clin J Pain 1992; 8: pp. 23-27.
112. Janjua R.M., Schultka R., Goebbel L., et. al.: The legacy of Johann Friedrich Meckel the Elder (1724–1774): a 4-generation dynasty of anatomists. Neurosurgery 2010; 66: pp. 758-770. discussion 770–771
113. Meckel J.: Dissertatio inauguralis medica anatomico physiologica de Quinto Pare Nervorum Cerebri. A..1748.VandenhoeckGöttingen, Germany
114. Sabancı P.A., Batay F., Civelek E., et. al.: Meckel’s cave. World Neurosurg 2011; 76: pp. 335-341. discussion 266–267
115. Sheth S., Branstetter B.F., Escott E.J.: Appearance of normal cranial nerves on steady-state free precession MR images. Radiographics 2009; 29: pp. 1045-1055.
116. Beck D.W., Menezes A.H.: Lesions in Meckel’s cave: variable presentation and pathology. J Neurosurg 1987; 67: pp. 684-689.
117. Kamel H.A., Toland J.: Trigeminal nerve anatomy: illustrated using examples of abnormalities. AJR Am J Roentgenol 2001; 176: pp. 247-251.
118. McIntyre N.: Andreas Vesalius (1514-84). J Med Biogr 2007; 15: pp. 96.
119. Sherzoi H.: Andreas Vesalius (1514–1567). J Invest Surg 1999; 12: pp. 131-132.
120. Shinohara A.L., de Souza Melo C.G., Silveira E.M.V., et. al.: Incidence, morphology and morphometry of the foramen of Vesalius: complementary study for a safer planning and execution of the trigeminal rhizotomy technique. Surg Radiol Anat 2010; 32: pp. 159-164.
121. Rossi A.C., Freire A.R., Prado F.B., et. al.: Morphological characteristics of foramen of Vesalius and its relationship with clinical implications. J Morphol Sci 2010; 27: pp. 26-29.
122. Vitek J.J.: Accessory meningeal artery: an anatomic misnomer. AJNR Am J Neuroradiol 1989; 10: pp. 569-573.
123. Tubbs R.S., Salter E.G.: Vidius Vidius (Guido Guidi): 1509–1569. Neurosurgery 2006; 59: pp. 201-203. discussion 201–203
124. Brockbank W.: The man who was Vidius. Ann R Coll Surg Engl 1956; 19: pp. 269-295.
125. Vescan A.D., Snyderman C.H., Carrau R.L., et. al.: Vidian canal: analysis and relationship to the internal carotid artery. Laryngoscope 2007; 117: pp. 1338-1342.
126. Mafee M., Som P.M.: Embryology, anatomy, and imaging of the eye and orbit.Som P.M.Curtin H.D.Head neck imaging.2011.pp. 527-589.
127. Osborn A.G.: The vidian artery: normal and pathologic anatomy. Radiology 1980; 136: pp. 373-378.
128. Ma Y., Tan G., Zhao Z., et. al.: Therapeutic effectiveness of endoscopic vidian neurectomy for the treatment of vasomotor rhinitis. Acta Otolaryngol 2014; 134: pp. 260-267.
129. Lloyd G., Howard D., Phelps P., et. al.: Juvenile angiofibroma: the lessons of 20 years of modern imaging. J Laryngol Otol 1999; 113: pp. 127-134.
130. Thakar A., Hota A., Bhalla A.S., et. al.: Overt and occult vidian canal involvement in juvenile angiofibroma and its possible impact on recurrence. Head Neck 2016; 38: pp. E421-E425.
131. Frixione E.: Albrecht von Haller (1708–1777). J Neurol 2006; 253: pp. 265-266.
132. Fye W.B.: Albrecht von Haller. Clin Cardiol 1995; 18: pp. 291-292.
133. Boerhaave H.: Praelectiones academicae in proprias institutiones rei medicae.1743.VandenhoeckGöttingen
134. Caversaccio M., Boschung U., Mudry A.: Historical review of Haller’s cells. Ann Anat 2011; 193: pp. 185-190.
135. Peiper H.-J.: Albrecht von Haller. An illustrious ancestor. Chirurg 2008; 79: pp. 486-493.
136. Bolger W.E., Butzin C.A., Parsons D.S.: Paranasal sinus bony anatomic variations and mucosal abnormalities: CT analysis for endoscopic sinus surgery. Laryngoscope 1991; 101: pp. 56-64.
137. Basić N., Basić V., Jukić T., et. al.: Computed tomographic imaging to determine the frequency of anatomical variations in pneumatization of the ethmoid bone. Eur Arch Otorhinolaryngol 1999; 256: pp. 69-71.
138. Stammberger H.R., Kennedy D.W., Anatomic Terminology Group: Paranasal sinuses: anatomic terminology and nomenclature. Ann Otol Rhinol Laryngol Suppl 1995; 167: pp. 7-16.
139. Christmas D.A., Mirante J.P., Yanagisawa E.: Endoscopic view of the removal of an obstructing Haller’s cell. Ear Nose Throat J 2006; 85: pp. 360-361.
140. Adolph Onodi (Budapest). J Laryngol Otol 1920; 35: pp. 350.
141. Onodi A.: Die sehstoerungen und erblindung nasalen ursprunges, bedingt durch erkrankungen der hinteren nebenhoehlen. Z Augenheilkd 1904; 12: pp. 23-46.
142. Vértes L.: Remembering Dr. Adolf Onodi, professor of rhinolaryngology, member of the Hungarian Academy of Sciences. Orv Hetil 2001; 142: pp. 739-743.
143. Tomovic S., Esmaeili A., Chan N.J., et. al.: High-resolution computed tomography analysis of the prevalence of Onodi cells. Laryngoscope 2012; 122: pp. 1470-1473.
144. Leunig A., Betz C.S., Sommer B., et. al.: [Anatomic variations of the sinuses; multiplanar CT-analysis in 641 patients]. Laryngorhinootologie 2008; 87: pp. 482-489.
145. Cherla D.V., Tomovic S., Liu J.K., et. al.: The central Onodi cell: a previously unreported anatomic variation. Allergy Rhinol Provid RI 2013; 4: pp. e49-e51.
146. Nickerson J.P., Lane A.P., Subramanian P.S., et. al.: Onodi cell mucocele causing acute vision loss: radiological and surgical correlation. Clin Neuroradiol 2011; 21: pp. 245-248.
147. Shoja M.M., Tubbs R.S., Loukas M., et. al.: Emil Zuckerkandl (1849–1910): anatomist and pathologist. Ann Anat 2008; 190: pp. 33-36.
148. Zuckerkandl E.: Nebst bermerkungen uber die epithkorperchen des menschen. Anat Hefte 1902; 61: pp. 61.
149. Schultheiss D.: Gustav Klimt and the field of medicine. Painting of the medical faculty—relationship with the Zuckerkandl family. Urologe A 2007; 46: pp. 1005-1010.
150. Sheahan P., Murphy M.S.: Thyroid tubercle of Zuckerkandl: importance in thyroid surgery. Laryngoscope 2011; 121: pp. 2335-2337.
151. Pelizzo M.R., Toniato A., Gemo G.: Zuckerkandl’s tuberculum: an arrow pointing to the recurrent laryngeal nerve (constant anatomical landmark). J Am Coll Surg 1998; 187: pp. 333-336.
152. Gauger P.G., Delbridge L.W., Thompson N.W., et. al.: Incidence and importance of the tubercle of Zuckerkandl in thyroid surgery. Eur J Surg 2001; 167: pp. 249-254.
153. Lee T.C., Selvarajan S.K., Curtin H., et. al.: Zuckerkandl tubercle of the thyroid: a common imaging finding that may mimic pathology. AJNR Am J Neuroradiol 2012; 33: pp. 1134-1138.
154. Simonsz H.J.: Johann Gottfried Zinn. Strabismus 2004; 12: pp. 125.
155. Zampieri F., Marrone D., Zanatta A.: Should the annular tendon of the eye be named “annulus of Zinn” or “of Valsalva”. Acta Ophthalmol (Copenh) 2015; 93: pp. 97-99.
156. Zinn J.: Descriptio anatomica oculi humani iconibus illustrata.1755.Abraham VandenhoeckGöttingen
157. Streng B., Ruprecht K.W., Wittern R.: Johann Gottfried Zinn—a Franconian anatomist and botanist. Klin Monbl Augenheilkd 1991; 199: pp. 57-61.