
Rationale and Objectives
The torcular herophili, or “confluence of the sinuses,” shows various configurations with other venous sinuses, as revealed by angiography. The aims of this study were to evaluate anatomic variations of this confluence and to assess their clinical relevance using three-dimensional (3D) computed tomographic (CT) venography.
Materials and Methods
The torcular herophili and its relevant venous sinuses were analyzed using 3D CT venography in 120 adults, consisting of 76 patients who were proven to have aneurysms and 44 patients who were proven to have no vascular malformations or aneurysms after the examinations. Three-dimensional CT venography was performed following the arterial phase of 3D CT angiography without any additional injection of contrast material. Three-dimensional volume-rendered venous images were reconstructed on a workstation and reviewed.
Results
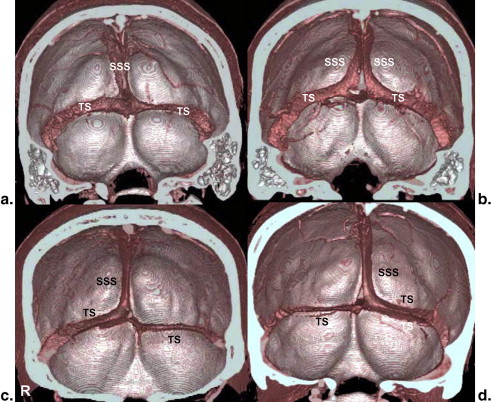
The superior sagittal sinus (SSS) drained into the transverse sinus (TS) in four patterns: the SSS reached the centrally located confluence, where it divided into the bilateral TS (20.0%); the SSS was prematurely duplicated into the right and left limbs and drained into the same side TS (26.7%); the SSS drained exclusively into the right TS (44.2%); or the SSS drained exclusively into the left TS (9.2%). The draining pattern of the straight sinus was also classified into four types. The right TS was larger than the left TS. The right TS were higher compared to the left TS. Persistent occipital sinuses were recognized in 57.5% of the subjects. Finally, persistent falcial sinuses were seen in 2.5% of the subjects. A septum in the SSS and complicated venous channels in the confluence were each seen in only one case.
Conclusion
Three-dimensional CT venography is useful as a noninvasive method to evaluate the confluence and its relevant dural sinuses and can provide useful information for surgical intervention.
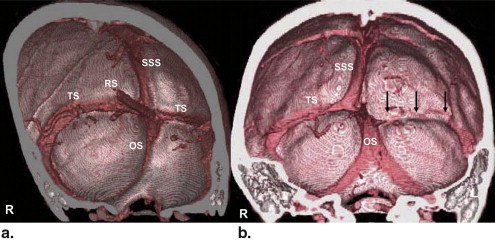
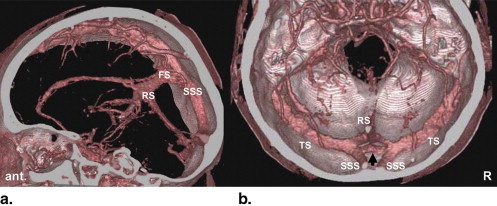
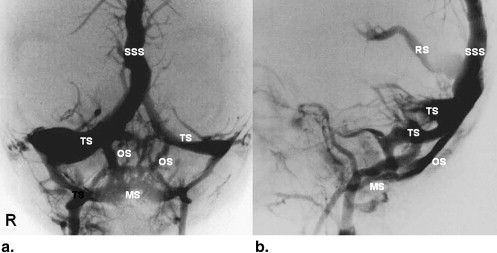
The torcular herophili, or the “confluence of the sinuses,” is defined as the dilated posterior end of the superior sagittal sinus (SSS), situated to one side (usually the right) of the internal occipital protuberance, where it turns to become a transverse sinus (TS). In this region, the straight sinus (sinus rectus [RS]) drains into the various points, and the occipital sinus (OS) occasionally joins and/or begins . The confluence and its convergent sinuses show various configurations as revealed by angiography.
Although many anatomic and cadaveric studies have investigated the confluence , its radiologic analysis in clinical cases has been rarely published, because selective cerebral angiography does not give a full picture of its configurations . For example, the medial portion of the TS is filled only on vertebral angiography and not on selective internal carotid angiography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Classification of Drainage Pattern of the SSS Into the TS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Classification of Drainage Pattern of the RS Into the TS
Get Radiology Tree app to read full this article<
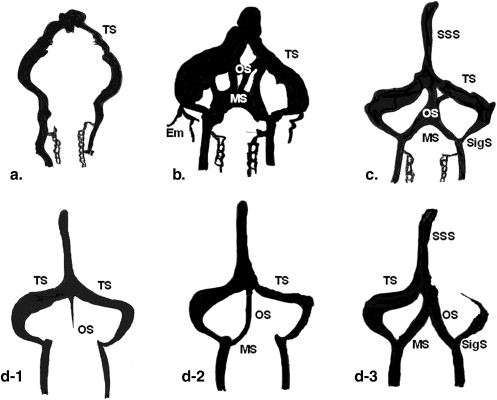
![Figure 2, Classification of the four types of drainage pattern of the straight sinus (sinus rectus [RS]) into the transverse sinus (TS). (a) The RS reaching the centrally located confluence, then dividing to the bilateral TS (Rc type): 63.3%. (b) The RS prematurely duplicating into the right and left limbs, then each draining into the same side TS (Rd type): 15.0%. (c) The RS predominantly draining into the right TS (Rr type): 10.0%. (d) The RS predominantly draining into the left TS (Rl type): 11.7%.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/AnatomicalEvaluationoftheDuralSinusesintheRegionoftheTorcularHerophiliUsingThreeDimensionalCTVenography/1_1s20S1076633210002473.jpg)
Get Radiology Tree app to read full this article<
Comparison in Size Between the Bilateral TS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison in Height Between the Bilateral TS
Get Radiology Tree app to read full this article<
Persistence of the OS and Its Configuration
Get Radiology Tree app to read full this article<
Other Anatomic Variations of Dural Venous Sinuses Near the Confluence
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Classification of the Drainage Pattern of the SSS Into the TS
Get Radiology Tree app to read full this article<
Table 1
Continuity of the SSS with the TS as Shown in Previous Studies
Study Total Subjects Sc (%) Sd (%) Sr (%) Sl (%) Henrici and Kikuchi (1903) 35 11.4 43 28.6 14.3 Edwards (1931) ∗ 50 12 48 22 14 Woodhall (1936) 100 9 52 30 9 Susa (1950) 120 10.8 25.8 52.6 10.8 Makiura (1953) 40 42.5 27.5 25 5 Browning (1953) 100 36 40 18 6 Kaplan et al (1972) ∗ 215 16 10 33 8 Bisaria (1985) ∗ 110 48 10 18 8 Ishizaka (1985) ∗ 52 37 23 17 15 Fukusumi et al (2002) 200 15 26 49 10 Singh et al (2004) 160 35 14 41 10 Present study 120 20.8 26.6 44.2 9.2
Sc, the SSS reaches the centrally located confluence, then divides into the bilateral TS; Sd, the SSS prematurely duplicates into the right and left channels, then drains into the same side TS; Sr, the SSS predominantly drains into the right TS; Sl, the SSS predominantly drains into the left TS; SSS, superior sagittal sinus; TS, transverse sinus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Classification of Drainage Pattern of the RS Into the TS
Get Radiology Tree app to read full this article<
Table 2
Continuity of the RS with the TS as Shown in Previous Studies
Study Total Subjects Rc (%) Rd (%) Rr (%) Rl (%) Knott (1882) 44 27 0 14 59 Henrici and Kikuchi (1903) 35 11.4 80 0 8.6 Susa (1950) 120 23.3 33.3 19.2 24.2 Makiura (1953) 40 42.5 25 10 22.5 Takeshige (1969) 168 33 39 5 13 Fukusumi et al (2002) 200 40.5 31 20 8.5 Present study 120 63.3 15 10 11.7
Rc, the RS reaches the centrally located confluence, then divides into the bilateral TS; Rd, the RS prematurely duplicates into the right and left limbs, then each drains into the same side TS; Rr, the RS predominantly drains into the right TS; Rl, the RS predominantly drains into the left TS; RS, straight sinus; TS, transverse sinus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison in Size Between the Bilateral TS
Get Radiology Tree app to read full this article<
Table 3
Dominance of the Right or Left Transverse Sinus as Shown in Previous Studies
Study Total Subjects R > L R = L R < L Edwards (1931) 50 50.0 8.0 42.0 Gibbs and Gibbs (1934) 25 52.0 20.0 29.0 Woodhall (1936) 100 39.0 48.0 13.0 Susa (1950) 120 68.0 16.0 16.0 Browning (1953) 100 51.0 20.0 29.0 Kaplan et al (1972) 215 62.0 15.0 23.0 Ishizaka (1985) 52 52.0 19.2 28.8 Goto and Koda (2000) 132 67.4 20.5 12.1 Fukusumi et al (2002) 200 68.5 10.0 21.5 Present study 120 63.3 21.7 15.0
R > L, with right dominance; R = L, with no dominance; R < L, with left dominance.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Comparison in Height Between the Bilateral TS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Persistent OS and Their Configuration
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Significance
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Gabella G.: Cardiovascular system.Williams P.L.Gray’s anatomy.1995.Churchill LivingstoneNew York:pp. 1583.
2. Bisaria K.K.: Anatomic variations of venous sinuses in the region of the torcular herophili. J Neurosurg 1985; 62: pp. 90-95.
3. Browning H.: The confluence of dural venous sinuses. Am J Anat 1953; 93: pp. 307-329.
4. Edwards E.A.: Anatomic variation of cranial venous sinuses. Their relation to the effect of jugular compression in lumbar manimetric test. Arch Neurol Psychiatr 1931; 26: pp. 801-814.
5. Gibbs E.L., Gibbs F.A.: The cross section areas of the vessels that form the torcular and the manner in which flow is distributed to the right and to the left lateral sinus. Ana Rec 1934; 59: pp. 419-426.
6. Goto N., Koda M.: Blood vessels in the central nervous system [in Japanese].Sato T.Akita K.Anatomical variations in Japanese.2000.University of Tokyo PressTokyo, Japan:pp. 401-429.
7. Henrici C., Kikuchi J.: Die Varianten der okzipitalen Sinusverbindungen (Confluence sinuum) und ihre klinische Bedeutung. Z Ohrenh 1903; 42: pp. 351-361.
8. Ishizaka H.: Anatomical study of the torcular herophili [in Japanese]. Neurol Med Chir (Tokyo) 1985; 25: pp. 873-880.
9. Kaplan H.A., Browder J., Knightly J.J., et. al.: Variations of the cerebral dural sinuses at the torcular herophili. Importance in radical neck dissection. Am J Surg 1972; 124: pp. 456-461.
10. Knott J.F.: On the cerebral sinuses and their variations. J Anat Phys 1882; 16: pp. 27-42.
11. Makiura F.: Variations of the confluence [in Japanese]. Acta Anat 1953; 28: pp. 87-88.
12. Singh M., Nagashima M., Inoue Y.: Anatomical variations of occipital bone impression for dural venous sinuses around the torcular Herophili. With special reference to the consideration of clinical significance. Surg Radiol Anat 2004; 26: pp. 480-487.
13. Susa Y.: Patterns of the torcular herophili, measurement of sinus lumen and histology of sinus wall [in Japanese]. J Nippon Medical School 1950; 27: pp. 247-263.
14. Takeshige Y.: Die Bedeutung des Venensystems fur die Hamodynamik des Hirnstammes. Anat Anz Bd 1969; 125: pp. 166-192.
15. Woodhall B.: Variations of cranial venous sinuses in the region of the torcular herophili. Arch Surg 1936; 33: pp. 297-314.
16. Dora F., Zileli T.: Common variations of the lateral and occipital sinuses at the confluens sinuum. Neuroradiology 1980; 20: pp. 23-27.
17. Fukusumi A., TanakaT Koh S, et. al.: Anatomical variations of the torcular herophili evaluated with MR venography [in Japanese]. Jpn J Clin Radiol 2002; 47: pp. 625-631.
18. Kobayashi K., Matsui O., Suzuki M., et. al.: Anatomical study of confluence of the sinuses with contrast-enhanced magnetic resonance venography. Neuroradiology 2006; 48: pp. 307-311.
19. Rollins N., Ison C., Booth T., et. al.: MR venography in the pediatric patient. AJNR Am J Neuroradiol 2005; 26: pp. 50-55.
20. Matsumoto M., Kodama N., Sakuma J., et. al.: 3D-CT arteriography and 3D-CT venography: the separate demonstration of arterial-phase and venous phase on 3D-CT angiography in a single procedure. AJNR Am J Neuroradiol 2005; 26: pp. 635-641.
21. Suzuki Y., Ikeda H., Shimadu M., et. al.: Variations of the basal vein: identification using three-dimensional CT angiography. AJNR Am J Neuroradiol 2001; 22: pp. 670-676.
22. Okudera T., Huang Y.P., Yokota A., et. al.: Development of posterior fossa dural sinuses, emissary veins, and jugular bulb: morphological and radiologic study. AJNR Am J Neuroradiol 1994; 15: pp. 1871-1883.
23. Okudera T., Huang Y.P., Yokota A., et. al.: Developmental radiology of posterior fossa dural sinuses in the human fetus: with special reference to physiological enlargement of transverse and occipital sinuses, formation of emissary veins, and development of superior jugular bulb from jugular sinuses.Hakuba A.Surgery of the intracranial venous system.1996.Springer-VerlagTokyo, Japan:pp. 192-203.
24. Okudera T., Ohta T., Huang Y.P.: Embryology of the cranial venous system with particular reference to the dural venous sinuses related to the torcular.Kapp J.P.Schmidek H.H.The cerebral venous system and its disorders.1998.Grune & StrattonOrlando, FL:pp. 93-107.
25. Padget D.H.: The development of cranial venous system in man. From the view point of comparative anatomy. Contrib Embryol 1957; 247: pp. 81-138.
26. Streeter G.L.: The development of the venous sinuses of the dura mater in the human embryo. Am J Anat 1915; 18: pp. 145-178.
27. Masaki S.: Studies on the development of the dural sinuses of the human fetus [in Japanese]. Fukuoka Acta Medica 1959; 50: pp. 2769-2788.
28. LeMay M.: Left-right dissymmetry, handedness. AJNR Am J Neuroradiol 1992; 13: pp. 493-504.
29. Hochberg F.H., LeMay M.: Angiographic correlates of handedness. Neurology 1975; 25: pp. 218-222.
30. Das A.C., Hasen M.: The occipital sinus. J Neurosurg 1970; 33: pp. 307-311.
31. Kobayashi K., Suzuki M., Ueda F., et. al.: Anatomical study of occipital sinus using contrast-enhanced magnetic resonance venography. Neuroradiology 2006; 48: pp. 373-379.
32. Zouaoui A., Hidden G.: Cerebral venous sinuses: anatomical variants or thrombosis?. Acta Anat 1988; 133: pp. 318-324.
33. Ohata K., Moududul H., Morino M., et. al.: Occlusion of the sigmoid sinus after surgery via the presigmoidal-transpetrosal approach. J Neurosurg 1998; 89: pp. 575-584.