
Rationale and Objectives
The study aimed to evaluate the association of a coronary interarterial course (IAC) with adverse outcomes in adults and to assess the benefit of coronary artery bypass grafting (CABG) in this population.
Materials and Methods
A retrospective review identified 172 adults over 40 years of age with an anomalous coronary artery origin from the opposite coronary sinus, including 79 patients with an IAC. Hard outcomes (myocardial infarction or cardiac death) and soft outcomes (persistent angina) were evaluated, with a mean follow-up time of 5 years.
Results
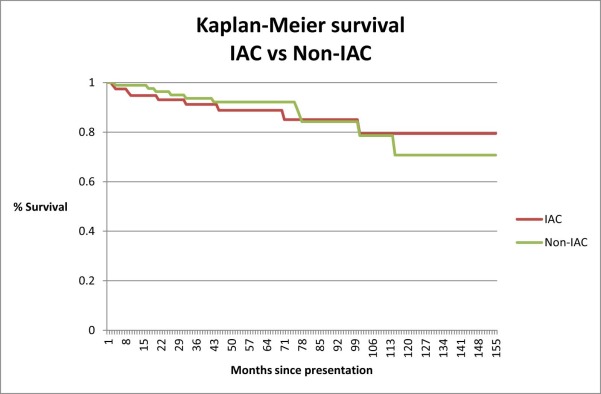
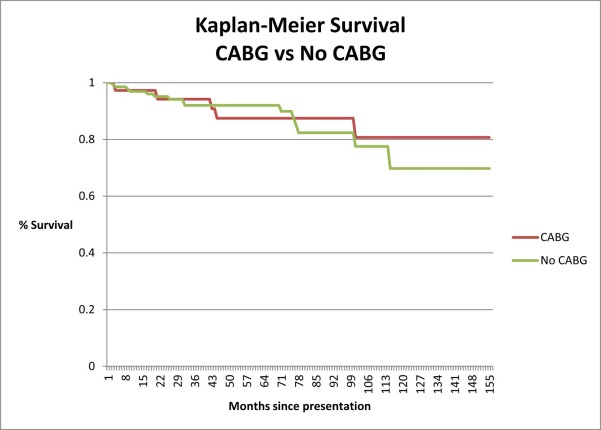
Although the frequency of coronary artery disease (CAD) was lower among patients with an IAC (43% vs 59%; P < 0.05), the frequency of CABG was higher among those with an IAC (21/79 = 26% vs 16/93 = 17%; P = 0.15). Hard outcomes were equally frequent among IAC patients (12/79 = 15%) compared to those without an IAC (16/93 = 17%) ( P = 0.7), and among patients with a right IAC (11/68 = 16%) compared to those with a left IAC (1/11 = 9%) ( P = 0.56). Among patients with an IAC, the frequency of hard outcomes was similar with CABG (4/21 = 19%) versus without CABG (8/59 = 14%) ( P = 0.55); the frequency of soft events was also similar with CABG (9/21 = 43%) versus without CABG (18/59 = 31%) ( P = 0.3). On multivariate analysis, the extent of coronary disease was the only significant predictor of hard or soft outcome (the presence of IAC, CABG, and left vs right IAC were not significant; P > 0.3).
Conclusions
The frequency of hard and soft outcomes among adult patients with anomalous coronary arteries is not significantly related to the presence of an IAC. No benefit was documented from the CABG treatment of an IAC in the absence of CAD.
Introduction
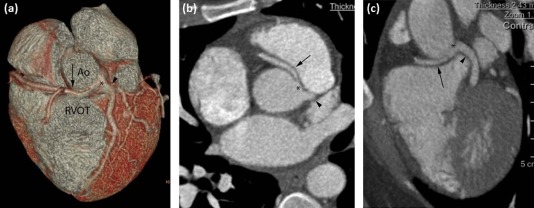
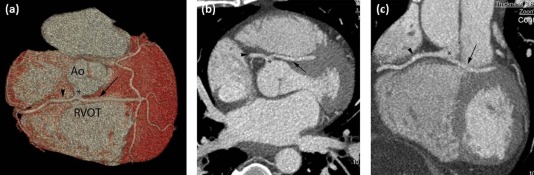
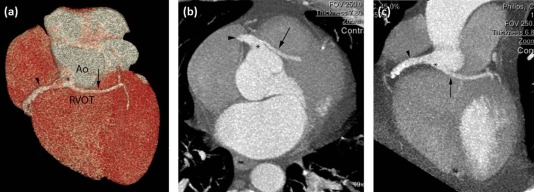
The incidence of anomalies of the coronary arteries is low, comprising up to 1.3% of the population in angiographic studies. Of these, less than half involve anomalous origins of the coronary arteries arising from the opposite coronary sinus (ACAOS). The most common anomalous coronary artery is a circumflex artery arising from the right coronary sinus or with a common origin with the right coronary artery (RCA). An anomalous circumflex artery always follows a “benign” course posterior to the aortic root. The more clinically significant anomalies include an anomalous RCA arising from the left coronary sinus, which is more common than an anomalous left main coronary artery (LMCA) arising from the right coronary sinus. Anomalous right and left main coronary arteries may follow either a “benign” course around the aorta and pulmonary artery, or a “malignant” interarterial course (IAC) between the aorta and pulmonary artery .
An anomalous coronary artery with an IAC is a recognized cause of sudden death in the pediatric population and young adults . Since the introduction of noninvasive coronary imaging with coronary computed tomography angiography (cCTA), these anomalies have been increasingly found in the adult population presenting to emergency rooms and doctor offices with symptoms of chest pain .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Information for All ACAOS Patients with or without an IAC
All IAC No IAC ( n = 172) ( n = 79) ( n = 93) Demographics Age in years 63.8 ± 12.1 63.5 ± 12.4 64.1 ± 11.8 Male/Female 95/77 38/41 57/36 %Male 55.2 48.1 61.3 Anomalous artery Left main (LMCA) 22 (12.8%) 11 (13.9%) 11 (11.8%) Right (RCA) 79 (45.9%) 68 (86.1%) 11 (11.8%) Circumflex 71 (41.3%) 0 71 (76.3%) No. of patients with 0/1/2/3 diseased vessels 86/28/27/31 45/9/12/13 41/19/15/18 No. of patients with disease in anomalous vessel 60 (34.9%) 28 (35.4%) 32 (34.4%) Follow-up Average follow-up time (months) 59.3 ± 38.1 54.4 ± 39.2 63.5 ± 36.8 Number bypassed 37 (21.5%) 21 (26.6%) 16 (17.2%) Soft outcomes 52 (30.2%) 26 (32.9%) 26 (28.0%) Hard outcomes 28 (16.3%) 12 (15.2%) 16 (17.2%) Death (all cause) 20 (11.6%) 9 (11.4%) 11 (11.8%)
ACAOS, anomalous origin of the coronary artery arising from the opposite coronary sinus; IAC, interarterial course; LMCA, left main coronary artery; RCA, right coronary artery.
Table 2
Patient Information for ACAOS Patient Who Underwent Coronary Artery Bypass Grafting with or without an IAC
All IAC No IAC ( n = 37) ( n = 21) ( n = 16) Demographics Age in years 69.0 ± 13.4 66.8 ± 15.3 71.9 ± 9.9 Male/Female 26/11 13/8 13/3 %Male 70.3 61.9 81.3 Anomalous artery Left main (LMCA) 4 (10.8%) 4 (19.0%) 0 Right (RCA) 17 (45.9%) 17 (81.0%) 0 Circumflex 16 (43.2%) 0 16 (100%) No. of patients with 0/1/2/3 diseased vessels 8/2/9/18 8/1/4/8 0/1/5/10 No. of patients with disease in anomalous vessel 23 (62.2%) 11 (52.4%) 12 (75.0%) Follow-up Average follow-up time (months) 78.4 ± 39.9 79.1 ± 40.5 77.4 ± 40.4 Soft outcomes 15 (40.5%) 9 (42.9%) 6 (37.5%) Hard outcomes 7 (18.9%) 4 (19.0%) 3 (18.8%) Death (all cause) 5 (13.5%) 3 (14.3%) 2 (12.5%)
ACAOS, anomalous origin of the coronary artery arising from the opposite coronary sinus; IAC, interarterial course; LMCA, left main coronary artery; RCA, right coronary artery.
Table 3
Patient Information for All ACAOS Patients Managed Medically with or without an IAC
All IAC No IAC ( n = 135) ( n = 58) ( n = 77) Demographics Age in years 62.3 ± 11.4 62.4 ± 11.2 62.5 ± 11.6 Male/Female 69/66 25/33 44/33 %Male 51.1 43.1 57.1 Anomalous artery Left main (LMCA) 18 (13.3%) 7 (12.1%) 11 (14.3%) (all 7 septal variants) Right (RCA) 62 (45.9%) 51 (87.9%) 11 (14.3%) Circumflex 55 (40.7%) 0 55 (71.4%) No. of patients with 0/1/2/3 diseased vessels 77/26/18/14 37/8/8/5 40/18/10/9 No. of patients with disease in anomalous vessel 37 (27.4%) 17 (29.3%) 20 (26.0%) Follow-up Average follow-up time (months) 54.1 ± 36.0 45.4 ± 35.0 60.6 ± 35.6 Soft outcomes 37 (27.4%) 17 (29.3%) 20 (26.0%) Hard outcomes 21 (15.6%) 8 (13.8%) 13 (16.9%) Death (all cause) 15 (11.1%) 6 (10.3%) 9 (11.7%)
ACAOS, anomalous origin of the coronary artery arising from the opposite coronary sinus; IAC, interarterial course; LMCA, left main coronary artery; RCA, right coronary artery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Logistic Regression Analysis for Hard Outcomes Alone Using Single Variable and Multivariate Analysis
Odds Ratio Standard Error 95% Confidence Interval_P_ Value Single variable Extent of disease 1.67 0.29 1.19–2.34 0.003 IAC 0.86 0.36 0.38–1.95 0.72 Right IAC 0.99 0.42 0.43–2.26 0.98 Left IAC 0.50 0.53 0.06–4.04 0.51 CABG 1.27 0.61 0.49–3.26 0.62 Multivariate Extent of disease 1.82 0.36 1.23–2.68 0.002 IAC 0.99 0.43 0.42–2.31 0.98 CABG 0.59 0.33 0.20–1.76 0.34
CABG, coronary artery bypass grafting; IAC, interarterial course.
Table 5
Logistic Regression Analysis for Both Hard and Soft Outcomes Combined Using Single Variable and Multivariate Analysis
Odds Ratio Standard Error 95% Confidence Interval_P_ Value Single variable Extent of disease 1.37 0.19 1.04–1.80 0.02 IAC 1.26 0.42 0.65–2.43 0.48 Right IAC 1.48 0.50 0.77–2.86 0.24 Left IAC 0.49 0.39 0.10–2.37 0.38 CABG 1.81 0.70 0.85–3.85 0.13 Multivariate Extent of disease 1.34 0.21 0.99–1.83 0.06 IAC 1.33 0.46 0.68–2.61 0.41 CABG 1.21 0.53 0.51–2.87 0.66
CABG, coronary artery bypass grafting; IAC, interarterial course.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Yamanaka O., Hobbs R.E.: Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990; 21: pp. 28-40.
2. Maron B.J., Doerer J.J., Haas T.S., et. al.: Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009; 119: pp. 1085-1092.
3. Lorenz E.C., Mookadam F., Mookadam M., et. al.: A systematic overview of anomalous coronary anatomy and an examination of the association with sudden cardiac death. Rev Cardiovasc Med 2006; 7: pp. 205-213.
4. Maron B.J., Epstein S.E., Roberts W.C.: Causes of sudden death in competitive athletes. J Am Coll Cardiol 1986; 7: pp. 204-214.
5. Burke A.P., Farb A., Virmani R., et. al.: Sports-related and non-sports-related sudden cardiac death in young adults. Am Heart J 1991; 121: pp. 568-575.
6. Budoff M.J., Ahmed V., Gul K.M., et. al.: Coronary anomalies by cardiac computed tomographic angiography. Clin Cardiol 2006; 29: pp. 489-493.
7. Pursnani A., Jacobs J.E., Saremi F., et. al.: Coronary CTA assessment of coronary anomalies. 2012; 6: pp. 48-59.
8. Frescura C., Basso C., Thiene G., et. al.: Anomalous origin of coronary arteries and risk of sudden death: a study based on an autopsy population of congenital heart disease. Hum Pathol 1998; 29: pp. 689-695.
9. Taylor A.J., Rogan K.M., Virmani R.: Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992; 20: pp. 640-647.
10. Maron B.J.: Triggers for sudden cardiac death in the athlete. Cardiol Clin 1996; 14: pp. 195-210.
11. Frommelt P.C., Sheridan D.C., Berger S., et. al.: Ten-year experience with surgical unroofing of anomalous aortic origin of a coronary artery from the opposite sinus with an interarterial course. J Thorac Cardiovasc Surg 2011; 142: pp. 1046-1051.
12. Shin H.J., Shin Y.R., Jung J.W., et. al.: Neo-ostium creation for anomalous aortic origin of the coronary artery. Ann Thorac Surg 2015; 99: pp. 1830-1832.
13. Hillis L.D., Smith P.K., Anderson J.L., et. al.: ACCF/AHA guideline for coronary artery bypass graft surgery: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011; 124: pp. 652-735.
14. Khan A., Menown I.A., Graham A., et. al.: Anomalous left main coronary artery: not always a simple surgical reimplantation. Cardiology and Therapy 2015; 4: pp. 77-82.
15. Angelini P., Walmsley R.P., Libreros A., et. al.: Symptomatic anomalous origination of the left coronary artery from the opposite sinus of Valsalva: clinical presentations, diagnosis, and surgical repair. Tex Heart Inst J 2006; 33: pp. 171-179.
16. Davies J.E., Burkhart H.M., Dearani J.A., et. al.: Surgical management of anomalous aortic origin of a coronary artery. Ann Thorac Surg 2009; 88: pp. 844-847. discussion 847-848
17. Reddy R.C., Takahashi M., Beckles D.L., et. al.: Anomalous right coronary artery from the left sinus: a minimally invasive approach. Eur J Cardiothorac Surg 2012; 41: pp. 287-290.
18. Marler A.T., Malik J.A., Slim A.M.: Anomalous left main coronary artery: case series of different courses and literature review. Case Rep Vasc Med 2013; 2013: pp. 380952.
19. Krasuski R.A., Magyar D., Hart S., et. al.: Long-term outcome and impact of surgery on adults with coronary arteries originating from the opposite coronary cusp. Circulation 2011; 123: pp. 154-162.
20. Stojanovska J., Garg A., Patel S., et. al.: Congenital and hereditary causes of sudden cardiac death in young adults: diagnosis, differential diagnosis, and risk stratification. Radiographics 2013; 33: pp. 1977-2001.
21. Opolski M.P., Pregowski J., Kruk M., et. al.: Prevalence and characteristics of coronary anomalies originating from the opposite sinus of Valsalva in 8,522 patients referred for coronary computed tomography angiography. Am J Cardiol 2013; 111: pp. 1361-1367.
22. Lee H.J., Hong Y.J., Kim H.Y., et. al.: Anomalous origin of the right coronary artery from the left coronary sinus with an interarterial course: subtypes and clinical importance. Radiology 2012; 262: pp. 101-108.
23. Ishikawa T., Brandt P.W.T.: Anomalous origin of the left main coronary artery from the right anterior aortic sinus: angiographic definition of anomalous course. Am J Cardiol 1985; 55: pp. 770-776.
24. Roberts W.C., Dicicco B.S., Waller B.F., et. al.: Origin of the left main from the right coronary artery or from the right aortic sinus with intramyocardial tunneling to the left side of the heart via the ventricular septum. The case against clinical significance of myocardial bridge or coronary tunnel. Am Heart J 1982; 104: pp. 303-305.
25. Serota H., Barth I.I.I.C.W., Seuc C.A., et. al.: Rapid identification of the course of anomalous coronary arteries in adults: the “dot and eye” method. Am J Cardiol 1990; 65: pp. 891-898.
26. Mirchandani S., Phoon C.K.L.: Management of anomalous coronary arteries from the contralateral sinus. Int J Cardiol 2005; 102: pp. 383-389.
27. Click R.L., Holmes D.R., Vlietstra R.E., et. al.: Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival—a report from the Coronary Artery Surgery Study. J Am Coll Cardiol 1989; 13: pp. 531-537.