
Modern imaging methods have been transformative in improving medical care. Cross-sectional imaging has largely eliminated the need for invasive “exploratory” surgery and is widely used to triage acutely ill patients. However, how to best use medical imaging with ongoing concerns related to overall costs and radiation risks remains controversial. Imaging saves lives, but overuse of imaging can add unnecessary costs to the health system and add to the radiation burden of the population. In this article, the American College of Radiology Appropriateness Criteria (ACRAC) are reviewed, while the Massachusetts General Hospital experience with a computerized physician (provider) order entry system and other approaches to utilization management are discussed. There are strong evidence-based indicators of appropriateness for a substantial percentage of common imaging applications and where this is the case, decision support systems based on ACRAC or other criteria can and should be used. Standardize health care delivery and elimination of wasteful practice variation can be achieved without the art of medicine being ignored or devalued.
Modern imaging methods have been transformative in improving medical care. Cross-sectional imaging with magnetic resonance imaging (MRI) and computed tomography (CT) has largely eliminated the need for invasive “exploratory” surgery and is widely used to triage acutely ill patients with resultant measurable positive impacts on morbidity, mortality, and costs . The introduction of breast cancer screening with mammography has been associated with reduced mortality from breast cancer. Imaging is now the guiding hand of medical practice in innumerable settings. Nonetheless, controversy still reigns over the correct utilization of medical imaging with ongoing concerns related, most importantly, to overall costs and radiation risks.
Finding the correct balance between the rising use of medical imaging and its costs and risks is a central question facing the health system at a policy level but also facing providers on a day-to-day patient-by-patient level. In short, imaging saves lives, but overuse of imaging can add unnecessary costs to the health system and add to the radiation burden of the population.
Four questions appear fundamental to achieving an ideal balance in imaging utilization and should be addressed before any imaging examination is undertaken. 1) Does this patient need an imaging examination in the first place? More specifically, is an imaging examination likely to generate medical information of value in caring for the patient? If the answer to the first question is negative, the additional considerations about imaging are moot. 2) If an imaging examination is felt indicated, exactly what should the examination be? 3) How should the examination be performed—what are the best modality and the best protocol?. And 4) Can the proposed imaging evaluation be performed with less ionizing radiation or no ionizing radiation? An additional important consideration is how to create practical approaches to addressing these questions that fit into and mesh with the work process or work flow of physicians and other providers that are neither disruptive to doctor–patient relationships nor excessively time consuming.
American College of Radiology Appropriateness Criteria (ACRAC)
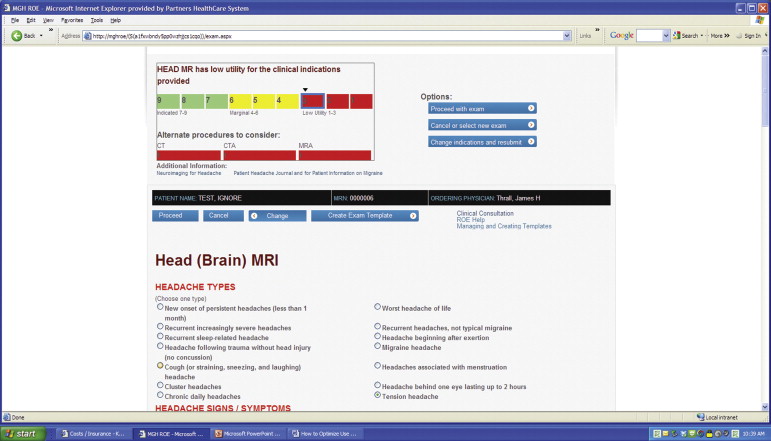
All the four key questions come back to the central concept of establishing criteria that address the relative appropriateness of use of imaging methods in different clinical settings. The ACRAC developed over the last 20 years define this linkage . The ACRAC are based on clinical scenarios of disease presentation where literature evidence and expert opinion are used to determine how likely it is that a particular imaging examination will yield medically meaningful information for a given indication or set of indications. The ACRAC use a scoring or scaling system from 1 (low likelihood of providing useful information) to 9 (high likelihood of providing useful information).
A more complete description and listing of the ACRAC are available on the ACR Web site. In brief, there are now ACRAC available for diagnostic, interventional, and radiation oncology topics. For diagnostic imaging, there are 197 topics, or clinical presentation scenarios, with over 900 variants . Each scenario variant has been assigned both an appropriateness score and an indication of the relative amount of radiation associated with the examination. The ACRAC are updated on an ongoing basis. There are expert teams for each part of the body that include radiologists and nonradiologists.
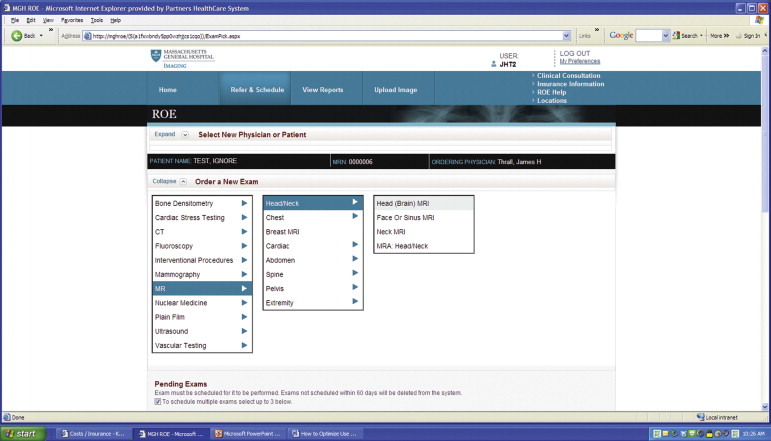
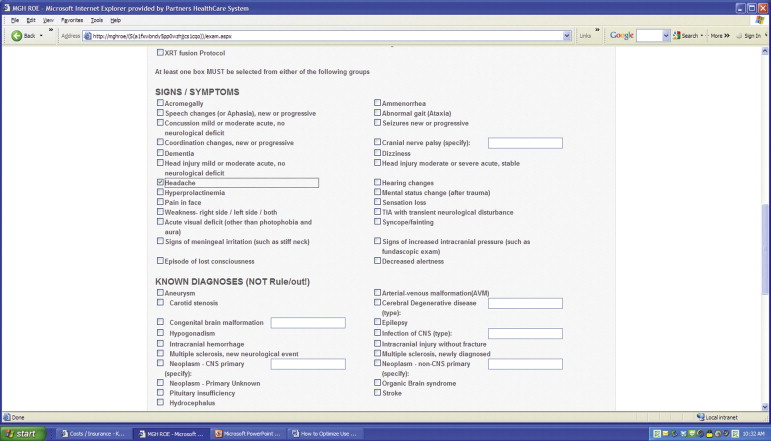
Computerized physician order entry
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Other approaches to utilization management
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Battle J.C., Hahn P.F., Thrall J.H., et. al.: Patients imaged early during admission demonstrate reduced length of hospital stay: a retrospective cohort study of patients undergoing cross-sectional imaging. J Am Coll Radiol 2010 Apr; 7: pp. 269-276.
2. Abujudeh H.H., Kaewlai R., McMahon P.M., et. al.: Abdominopelvic CT increases diagnostic certainty and guides management decisions: a prospective investigation of 584 patients in a large academic medical center. AJR Am J Roentgenol 2011 Feb; 196: pp. 238-243.
3. Rao P.M., Rhea J.T., Novelline R.A., et. al.: Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Engl J Med 1998; 338: pp. 141-146.
4. Cascade P.N.: Setting appropriateness guidelines for radiology. Radiology 1994; 192: pp. 50A-54A.
5. Cascade P.N.: The American College of Radiology. ACR Appropriateness Criteria Project. Radiology 2000; 214: pp. 3-46.
6. American College of Radiology. About the ACR Appropriateness Criteria. Available at http// www.acr.org/Quality-Safety/Appropriateness-Criteria/AboutAC . Accessed February 12, 2014.
7. Sistrom C.L., Dang P.A., Weilburg J.B., et. al.: Effect of computerized order entry with integrated decision support on the growth of outpatient procedure volumes: seven-year time series analysis. Radiology 2009 Apr; 251: pp. 147-155.
8. Vartanians V.M., Sustrom C.L., Weilburg J.B., et. al.: Increasing the appropriateness of outpatient imaging: effects of a barrier to ordering low-yield examinations. Radiology 2010; 255: pp. 842-849.
9. Hendee W.R., Becker G.J., Borgstede J.P., et. al.: Addressing overutilization in medical imaging. Radiology 2010 Oct; 257: pp. 240-245.