
Rationale and Objectives
Aim of the study was to compare between volumetric and unidimensional approaches for treatment response monitoring in a nude rat model of experimental bone metastases. For the volumetric approach, an automated segmentation algorithm of osteolytic lesions was introduced and compared to manual volumetry.
Material and Methods
Nude rats bearing osteolytic metastases were treated with zoledronate and sunitinib and compared to controls. Treatment response was assessed longitudinally in vivo using flat-panel volumetric computed tomography at days 30, 35, 45, and 55 after tumor cell inoculation. The mean sizes and volumes of osteolytic lesions were determined according to response evaluation criteria in solid tumors (RECIST) and by automated and manual volumetry (software: MITK [The Medical Imaging Interaction Toolkit, Heidelberg, Germany] and VIRTUOS, Heidelberg, Germany).
Results
In contrary to RECIST, the manual volumetric approach indicated a significant decrease in osteolytic lesion volume in response to treatment. The presented automatic segmentation algorithm for treatment monitoring identified bone metastases adequately and assessed changes in the osteolytic lesion volume over time according to manual volumetry.
Conclusions
In an animal model, volumetric treatment response assessment of osteolytic bone metastases is superior to unidimensional measurements, and automated volumetric segmentation may be a valuable alternative to manual volume determination.
Bone is the most common site of metastasis for breast and prostate cancer. Bone pain, pathologic fractures, and immobility are clinical complications of bone metastasis which can profoundly impair quality of life for long-term survivors . Treatment options for inhibiting breast cancer bone metastases are currently including the systemic treatment options bisphosphonates, chemotherapy, and hormone therapy. Furthermore, novel therapeutic approaches for metastatic breast cancer enclose antiangiogenic treatments .
Treatment response assessment of bone metastases is complicated because of the complex morphology of skeletal lesions and the slow turnover of bone matrix on therapy . Beside magnetic resonance imaging (MRI) for evaluation of bone marrow involvement of metastasis, computed tomography (CT) is commonly used in clinical practice to determine morphologic osseous changes after application of treatment. The commonly used classification system for therapy monitoring in solid tumors is the response evaluation criteria in solid tumors (RECIST) that is based on unidimensional measurement of primary tumors and metastases as determined by the largest lesion diameter . Bone metastases, however, have been considered as “immeasurable” in the initial version of these guidelines because of the complex morphology . In the revised RECIST guidelines (version 1.1), some additions have been made defining osteolytic or mixed lesions with identifiable soft tissue masses as measurable lesions by CT and MRI . Thus, measuring unidimensional diameters of the soft tissue component of skeletal metastases is the current standard for response evaluation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Animal Model and Treatment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Data Analysis
Response evaluation criteria in solid tumors
Get Radiology Tree app to read full this article<
Manual volumetry
Get Radiology Tree app to read full this article<
Automated software tool for the analysis of osteolytic lesions
Get Radiology Tree app to read full this article<
Statistical analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histologic Staining
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Therapy Response
RECIST (Manual Measurement Unidimensional)
Get Radiology Tree app to read full this article<
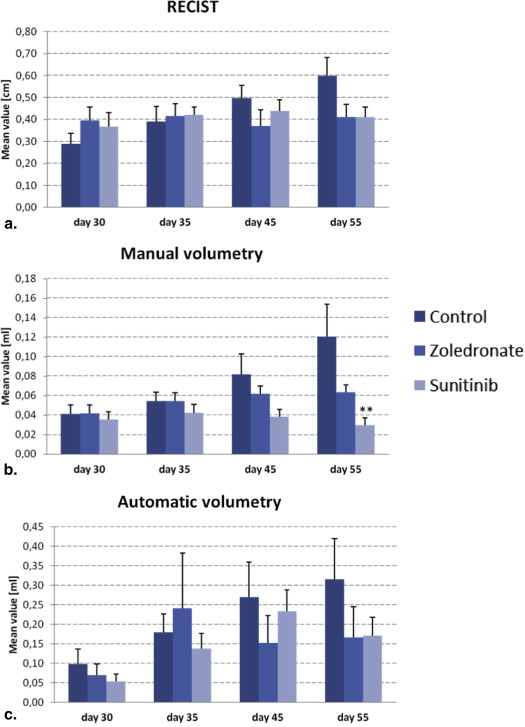
Table 1
Study Results
Day 30 Day 35 Day 45 Day 55 RECIST (cm) Control 0.29 ± 0.05 0.39 ± 0.07 0.50 ± 0.06 0.60 ± 0.09 Zoledronate 0.40 ± 0.06 0.42 ± 0.05 0.37 ± 0.07 0.41 ± 0.06 Sunitinib 0.37 ± 0.07 0.42 ± 0.04 0.44 ± 0.05 0.41 ± 0.05 Manual (mL) Control 0.04 ± 0.01 0.05 ± 0.01 0.08 ± 0.02 0.12 ± 0.04 Zoledronate 0.04 ± 0.01 0.05 ± 0.02 0.06 ± 0.02 0.06 ± 0.02 Sunitinib 0.04 ± 0.01 0.04 ± 0.01 0.04 ± 0.01 0.03 ± 0.01** Automatic (mL) Control 0.09 ± 0.04 0.18 ± 0.05 0.27 ± 0.09 0.32 ± 0.1 Zoledronate 0.07 ± 0.03 0.24 ± 0.14 0.15 ± 0.07 0.17 ± 0.08 Sunitinib 0.05 ± 0.02 0.14 ± 0.04 0.23 ± 0.05 0.17 ± 0.05
For in vivo experiments, all mean values from day 30, 35, 45, and 55 are given in absolute numbers ± standard error. Numbers for manual volumetry were reported previously .
Asterisks denote a significant difference between groups (** P < .01).
Get Radiology Tree app to read full this article<
Manual volumetry
Get Radiology Tree app to read full this article<
Automated volumetry
Get Radiology Tree app to read full this article<
Histology
Get Radiology Tree app to read full this article<
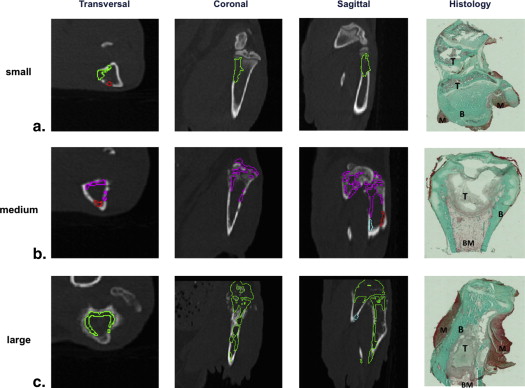
Get Radiology Tree app to read full this article<
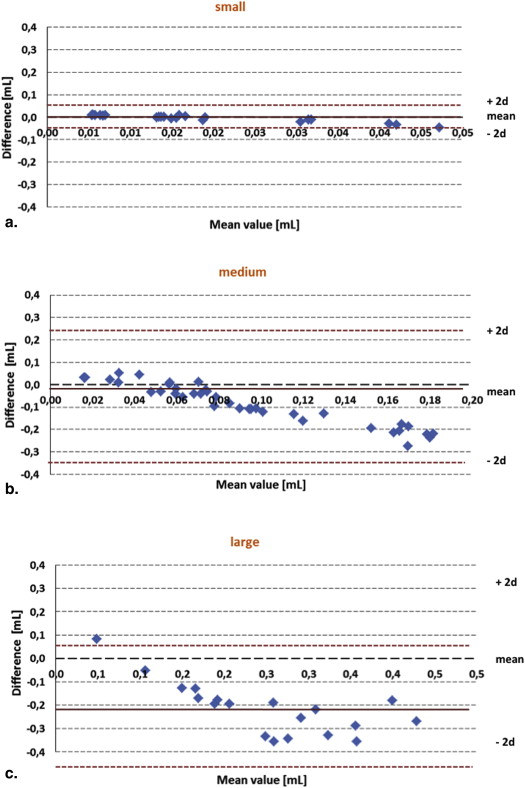
Comparison Between Manual and Automated Segmentation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison Between Manual and Automated Segmentation (Bland–Altman Analysis)
Volume Mean Manual Mean Automatic Mean Difference Deviation Factor Small 0.02 0.05 0.03 2.2 Medium 0.05 0.18 0.12 3.4 Large 0.12 0.31 0.21 2.7 Mean Value 0.06 0.17 0.36 2.8
The mean values for manual and automatic segmentation, as well as the mean difference and deviation factor for the techniques, are given for small (0.008–0.029 mL), medium (0.03–0.078 mL), and large (0.079–0.309 mL) bone Metastases.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Coleman R.E.: Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev 2001; 27: pp. 165-176.
2. Bäuerle T., Merz M., Komljenovic D., et. al.: Drug-induced vessel remodeling in bone metastases as assessed by dynamic contrast enhanced magnetic resonance imaging and vessel size imaging: a longitudinal in vivo study. Clin Cancer Res 2010; 16: pp. 3215-3225.
3. Burstein H.J., Elias A.D., Rugo H.S., et. al.: Phase II study of sunitinib malate, an oral multitargeted tyrosine kinase inhibitor, in patients with metastatic breast cancer previously treated with an anthracycline and a taxane. J Clin Oncol 2008; 26: pp. 1810-1816.
4. Bäuerle T., Semmler W.: Imaging response to systemic therapy for bone metastases. Eur Radiol 2009; 19: pp. 2495-2507.
5. Miller A.B., Hoogstraten B., Staquet M., et. al.: Reporting results of cancer treatment. Cancer 1981; 47: pp. 207-214.
6. Therasse P., Arbuck S.G., Eisenhauer E.A., et. al.: New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000; 92: pp. 205-216.
7. Eisenhauer E.A., Therasse P., Bogaerts J., et. al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: pp. 228-247.
8. Heussel C.P., Meier S., Wittelsberger S., et. al.: Follow-up CT measurement of liver malignoma according to RECIST and WHO vs. volumetry. Rofo 2007; 179: pp. 958-964.
9. Yankelevitz D.F., Reeves A.P., Kostis W.J., et. al.: Small pulmonary nodules: volumetrically determined growth rates based on CT evaluation. Radiology 2000; 217: pp. 251-256.
10. Fabel M., von Tengg-Kobligk H., Giesel F.L., et. al.: Semi-automated volumetric analysis of lymph node metastases in patients with malignant melanoma stage III/IV–a feasibility study. Eur Radiol 2008; 18: pp. 1114-1122.
11. Gao L., Heath D.G., Kuszyk B.S., et. al.: Automatic liver segmentation technique for three-dimensional visualization of CT data. Radiology 1996; 201: pp. 359-364.
12. Bäuerle T., Adwan H., Kiessling F., et. al.: Characterization of a rat model with site-specific bone metastasis induced by MDA-MB-231 breast cancer cells and its application to the effects of an antibody against bone sialoprotein. Int J Cancer 2005; 115: pp. 177-186.
13. Fränzle A., Bretschi M., Bäuerle T., et. al.: A quantification strategy for missing bone mass in case of osteolytic bone lesions. Med Phys 2013; 40: pp. 123501.
14. Bendl R.: Virtual therapy simulation. New technologies in radiation oncology.2006.Springer VerlagBerlin Heidelberg New Yorkpp. 179-186.
15. Erasmus J.J., Gladish G.W., Broemeling L., et. al.: Interobserver and intraobserver variability in measurement of non-small-cell carcinoma lung lesions: implications for assessment of tumor response. J Clin Oncol 2003; 21: pp. 2574-2582.
16. Thiesse P., Ollivier L., Di Stefano-Louineau D., et. al.: Response rate accuracy in oncology trials: reasons for interobserver variability. Groupe Francais d’Immunotherapie of the Federation Nationale des Centres de Lutte Contre le Cancer. J Clin Oncol 1997; 15: pp. 3507-3514.
17. Zhao B., Schwartz L.H., Moskowitz C.S., et. al.: Lung cancer: computerized quantification of tumor response initial results. Radiology 2006; 241: pp. 892-898.
18. Marten K., Auer F., Schmidt S., et. al.: Automated CT volumetry of pulmonary metastases: the effect of a reduced growth threshold and target lesion number on the reliability of therapy response assessment using RECIST criteria. Eur Radiol 2007; 17: pp. 2561-2571.
19. Vogel M.N., Vonthein R., Schmucker S., et. al.: Automated pulmonary nodule volumetry with an optimized algorithm. Accuracy at different slice thicknesses compared to unidimensional and bidimensional measurements. Rofo 2008; 180: pp. 791-797.
20. Ratain M.J., Eckhardt S.G.: Phase II studies of modern drugs directed against new targets: if you are fazed, too, then resist RECIST. J Clin Oncol 2004; 22: pp. 4442-4445.
21. Bretschi M., Merz M., Komljenovic D., et. al.: Cilengitide inhibits metastatic bone colonization in a nude rat model. Oncol Rep 2011; 26: pp. 843-851.
22. Merz M., Komljenovic D., Semmler , et. al.: Quantitative contrast-enhanced ultrasound for imaging antiangiogenic treatment response in experimental osteolytic breast cancer bone metastases. Invest Radiol 2012; 47: pp. 422-429.
23. Bäuerle T., Bartling S., Berger M., et. al.: Imaging anti-angiogenic treatment response with DCE-VCT, DCE-MRI and DWI in an animal model of breast cancer bone metastasis. Eur J Radiol 2010; 73: pp. 280-287.
24. Nakayama Y., Li Q., Katsuragawa S., et. al.: Automated hepatic volumetry for living related liver transplantation at multisection CT. Radiology 2006; 240: pp. 743-748.