
Rationale and Objectives
To understand the reasons leading to potentially inappropriate management of imaging findings concerning for malignancy and identify optimal methods for communicating these findings to providers.
Materials and Methods
We identified all abdominal imaging examinations with findings of possible cancer performed on six randomly selected days in August to December 2013. Electronic medical records (EMR) of one patient group were reviewed 3 months after the index examination to determine whether management was appropriate (completed follow-up or documented reason for no follow-up) or potentially inappropriate (no follow-up or no documented reason). Providers of a second patient group were contacted 5–6 days after imaging examinations to determine notification preferences.
Results
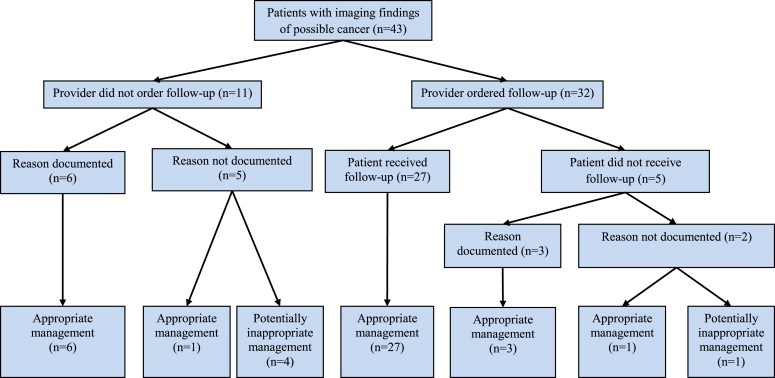
Among 43 patients in the first group, five (12%) received potentially inappropriate management. Reasons included patient loss to follow-up and provider failure to review imaging results, document known imaging findings, or communicate findings to providers outside the health system. Among 16 providers caring for patients in the second group, 33% were unaware of the findings, 75% preferred to be notified of abnormal findings via e-mail or EMR, 56% wanted an embedded hyperlink enabling immediate follow-up order entry, and only 25% had a system to monitor whether patients had completed ordered testing.
Conclusions
One in eight patients did not receive potentially necessary follow-up care within 3 months of imaging findings of possible cancer. Automated notification of imaging findings and follow-up monitoring not only is desired by providers but can also address many of the reasons we found for inappropriate management.
Lack of follow-up for imaging findings of possible cancer can result in missed or delayed diagnoses and preventable patient harm . When radiologists report imaging findings that may represent cancer and issue recommendations for follow-up, they may be unaware of whether follow-up is clinically indicated. For some patients (eg, those with diffuse metastatic disease, limited life expectancy, or guarded prognosis), it is appropriate for clinicians not to pursue further testing or interventions, even if follow-up is recommended by a radiologist. Conversely, when follow-up is clinically indicated, lack of follow-up is inappropriate and generally due to system errors (eg, provider fails to read radiology report, provider fails to order follow-up test, patient misses scheduled test) . Patients who do not complete clinically indicated follow-up may present with advanced cancer long after follow-up should have occurred, often resulting in medical malpractice suits . Therefore, to improve patient safety and reduce medicolegal risk, it is critical for providers and health systems to monitor follow-up of imaging findings of possible cancer and ensure that indicated follow-up actually occurs.
Automated systems have decreased provider notification time for abnormal laboratory and pathology results, increased rates of completed laboratory and pathology follow-up, and improved provider and patient satisfaction regarding communication of these test results . Because imaging findings of possible cancer generally require delayed follow-up, sometimes up to 12 months after initial detection, automated systems are ideally suited to provide notification and monitoring of these findings. However, the effect of these systems in radiology remains relatively unexplored compared to other areas of medicine . In addition, optimal methods for communicating nonemergent radiology findings to physicians are poorly understood.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Chart Review and Telephone Survey for Determining Patient Follow-up Patterns
1. Admission status when imaging examination was performed (ambulatory, Emergency Department, inpatient) 2. Was the imaging finding of possible cancer acknowledged in the patient chart?If yes, proceed to question 3; if no, skip to question 4 3. Days between date of imaging examination and acknowledgement of finding(s) 4. Did the provider order/plan to order any follow-up for the imaging finding of possible cancer?If yes, proceed to question 5; if no, skip to question 6 5. What type of follow-up did the provider order/plan to order? 6. If no follow-up was planned/ordered, was a reason found in the patient chart?If yes, proceed to question 7; if no, skip to question 8 7. What reason for lack of planned/ordered follow-up was given in the chart? 8. What reason for lack of planned/ordered follow-up was given by the provider (via telephone or email)? Chart is complete 9. Did the patient receive planned follow-up?If yes, chart is complete; if no, proceed to question 10 10. Was a reason for lack of follow-up found in the patient chart?If yes, proceed to question 11; if no, skip to question 12 11. What reason for lack of follow-up was given in the patient chart? 12. What reason for lack of follow-up was given by the provider (via telephone or email)?
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Telephone Survey for Determining Provider Communication Preferences
1. Are you the provider who ordered this imaging examination? 2. Were you aware of the abnormal finding(s) on the imaging examination? 3. How do you plan to follow-up on the abnormal finding(s)? 4. We are creating an automated system to notify providers about abnormal imaging findings. What type of automatic notification would you prefer? Examples include: a. Message through electronic medical record b. Email c. Telephone call d. Page e. Text message f. Other 5. Do you have suggestions for how this automated system could facilitate follow-up? Examples include: a. An automated email or phone call to the patient that provides imaging results b. An automated email or phone call to the patient that asks him/her to call the office but does not provide results c. A hyperlink embedded within the electronic medical record or email notification allowing you to order a follow-up examination immediately d. An automated message sent to a staff member who can contact the patient on your behalf and order follow-up testing e. Other 6. Who should be notified of imaging findings of possible cancer? Options include: a. Provider only b. Patient only c. Provider and patient 7. Do you currently have a system to monitor whether a patient for whom you have ordered a test has received that test?If no, survey is complete; if yes, proceed to question 8 8. Please describe your monitoring system.
Get Radiology Tree app to read full this article<
Data Collection and Management
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 3
Patient and Imaging Characteristics
Variable Value_n_ % Number of exams flagged 71 — Mean examinations flagged per day 12 — Patient age, years (mean, range) 61 18 to >90 Male gender 38 54 Admission status Outpatient 54 76 Emergency department ∗ 6 8 Inpatient 11 15 Known history of cancer 48 68 Active cancer † 39 55 Imaging modality of initial detection Computed tomography (CT) 47 66 Magnetic resonance imaging (MRI) 17 24 Ultrasound 7 10 Organ with imaging finding of possible cancer ( n = 79) ‡ Liver 36 46 Pancreas 5 6 Kidney 29 37 Adrenal gland 9 11 Types of imaging findings ( n = 79) ‡ Indeterminate 31 39 Suspicious for malignancy 48 61
CT, abdomen/pelvis or urogram, with or without contrast; MRI, with or without contrast; Ultrasound, retroperitoneal or right upper quadrant.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Patient Follow-up Patterns
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Reasons for Incomplete Follow-up of Imaging Findings of Possible Cancer
Reason Follow-up Management_n_ Follow-up ordered but not completed; reason documented ( n = 3) Follow-up planned for future date Appropriate 2 Follow-up at outside institution Appropriate 1 Follow-up ordered but not completed; reason not documented ( n = 2) Patient death Appropriate 1 Loss to follow-up after hospital discharge Potentially inappropriate 1 Follow-up not ordered; reason documented ( n = 6) Disagreement with recommended follow-up Appropriate 1 Patient choice Appropriate 1 Poor prognosis Appropriate 4 Follow-up not ordered; reason not documented ( n = 5) Disagreement with recommended follow-up Appropriate 1 Provider unaware of finding Potentially inappropriate 2 Provider aware of finding; no follow-up ordered Potentially inappropriate 1 Patient presumed to have followed up at outside institution Potentially inappropriate 1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Communication Preferences
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Gandhi T.K., Kachalia A., Thomas E.J., et. al.: Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med 2006; 145: pp. 488-496.
2. Schiff G.D., Hasan O., Kim S., et. al.: Diagnostic error in medicine: analysis of 583 physician-reported errors. Arch Intern Med 2009; 169: pp. 1881-1887.
3. Studdert D.M., Mello M.M., Gawande A.A., et. al.: Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med 2006; 354: pp. 2024-2033.
4. Callen J.L., Westbrook J.I., Georgiou A., et. al.: Failure to follow-up test results for ambulatory patients: a systematic review. J Gen Intern Med 2012; 27: pp. 1334-1348.
5. Choksi V.R., Marn C.S., Bell Y., et. al.: Efficiency of a semiautomated coding and review process for notification of critical findings in diagnostic imaging. AJR Am J Roentgenol 2006; 186: pp. 933-936.
6. Dupuis E.A., White H.F., Newman D., et. al.: Tracking abnormal cervical cancer screening: evaluation of an EMR-based intervention. J Gen Intern Med 2010; 25: pp. 575-580.
7. Verberne C.J., Nijboer C.H., de Bock G.H., et. al.: Evaluation of the use of decision-support software in carcino-embryonic antigen (CEA)-based follow-up of patients with colorectal cancer. BMC Med Inform Decis Mak 2012; 12: pp. 14.
8. El-Kareh R., Roy C., Williams D.H., et. al.: Impact of automated alerts on follow-up of post-discharge microbiology results: a cluster randomized controlled trial. J Gen Intern Med 2012; 27: pp. 1243-1250.
9. Humphrey L.L., Shannon J., Partin M.R., et. al.: Improving the follow-up of positive hemoccult screening tests: an electronic intervention. J Gen Intern Med 2011; 26: pp. 691-697.
10. Piva E., Sciacovelli L., Zaninotto M., et. al.: Evaluation of effectiveness of a computerized notification system for reporting critical values. Am J Clin Pathol 2009; 131: pp. 432-441.
11. Rind D.M., Safran C., Phillips R.S., et. al.: Effect of computer-based alerts on the treatment and outcomes of hospitalized patients. Arch Intern Med 1994; 154: pp. 1511-1517.
12. Park H., Min W.-K., Lee W., et. al.: Evaluating the short message service alerting system for critical value notification via PDA telephones. Ann Clin Lab Sci 2008; 38: pp. 149-156.
13. Dalal A.K., Roy C.L., Poon E.G., et. al.: Impact of an automated email notification system for results of tests pending at discharge: a cluster-randomized controlled trial. J Am Med Inform Assoc JAMIA 2013;
14. Dalal A.K., Schnipper J.L., Poon E.G., et. al.: Design and implementation of an automated email notification system for results of tests pending at discharge. J Am Med Inform Assoc JAMIA 2012; 19: pp. 523-528.
15. Matheny M.E., Gandhi T.K., Orav E.J., et. al.: Impact of an automated test results management system on patients’ satisfaction about test result communication. Arch Intern Med 2007; 167: pp. 2233-2239.
16. Poon E.G., Haas J.S., Louise Puopolo A., et. al.: Communication factors in the follow-up of abnormal mammograms. J Gen Intern Med 2004; 19: pp. 316-323.
17. Singh H., Arora H.S., Vij M.S., et. al.: Communication outcomes of critical imaging results in a computerized notification system. J Am Med Inform Assoc 2007; 14: pp. 459-466.
18. Burnside E.S., Sickles E.A., Bassett L.W., et. al.: The ACR BI-RADS experience: learning from history. J Am Coll Radiol JACR 2009; 6: pp. 851-860.
19. Langlotz C.P.: ACR BI-RADS for breast imaging communication: a roadmap for the rest of radiology. J Am Coll Radiol JACR 2009; 6: pp. 861-863.
20. Singh H., Thomas E.J., Mani S., et. al.: Timely follow-up of abnormal diagnostic imaging test results in an outpatient setting: are electronic medical records achieving their potential?. Arch Intern Med 2009; 169: pp. 1578-1586.
21. Eskander M.G., Leung A., Lee D.: Style and content of CT and MR imaging lumbar spine reports: radiologist and clinician preferences. AJNR Am J Neuroradiol 2010; 31: pp. 1842-1847.
22. Berland L.L., Silverman S.G., Gore R.M., et. al.: Managing incidental findings on abdominal CT: white paper of the ACR Incidental Findings Committee. J Am Coll Radiol 2010; 7: pp. 754-773.
23. Berland L.L., Silverman S.G., Megibow A.J., et. al.: ACR members’ response to JACR white paper on the management of incidental abdominal CT findings. J Am Coll Radiol JACR 2014; 11: pp. 30-35.
24. Larson P.A., Berland L.L., Griffith B., et. al.: Actionable findings and the role of IT support: report of the ACR Actionable Reporting Work Group. J Am Coll Radiol JACR 2014; 11: pp. 552-558.
25. Poon E.G., Gandhi T.K., Sequist T.D., et. al.: “I wish I had seen this test result earlier!”: dissatisfaction with test result management systems in primary care. Arch Intern Med 2004; 164: pp. 2223-2228.
26. Boohaker E.A., Ward R.E., Uman J.E., et. al.: Patient notification and follow-up of abnormal test results. A physician survey. Arch Intern Med 1996; 156: pp. 327-331.
27. Poon E.G., Kachalia A., Puopolo A.L., et. al.: Cognitive errors and logistical breakdowns contributing to missed and delayed diagnoses of breast and colorectal cancers: a process analysis of closed malpractice claims. J Gen Intern Med 2012; 27: pp. 1416-1423.
28. Giardina T.D., King B.J., Ignaczak A.P., et. al.: Root cause analysis reports help identify common factors in delayed diagnosis and treatment of outpatients. Health Aff Proj Hope 2013; 32: pp. 1368-1375.
29. Lopiano M., Stolz J., Sunshine J., et. al.: Physician referrals to radiologists. AJR Am J Roentgenol 1990; 155: pp. 1327-1330.
30. Schreiber M.H., Leonard M., Rieniets C.Y.: Disclosure of imaging findings to patients directly by radiologists: survey of patients’ preferences. AJR Am J Roentgenol 1995; 165: pp. 467-469.
31. Johnson A.J., Easterling D., Nelson R., et. al.: Access to radiologic reports via a patient portal: clinical simulations to investigate patient preferences. J Am Coll Radiol JACR 2012; 9: pp. 256-263.
32. Berlin L.: Communicating results of all outpatient radiologic examinations directly to patients: the time has come. AJR Am J Roentgenol 2009; 192: pp. 571-573.
33. Chadalavada S., Cook T., Langlotz C.: Communicating radiology results to patients: results from universal online release by an academic radiology department (LL-INS-SU2B). Radiological Society of North America 2013;