
Rationale and Objectives
The purpose of this retrospective study was to compare the maximum intensity projection (MIP) images generated at a multidetector computed tomography (MDCT) scanner console using advanced tools at a three-dimensional (3D) workstation for assessment of pancreatic tumor resectability.
Materials and Methods
Institutional review board approval and informed consent wavier were obtained for this retrospective study. The intraoperative findings were used as reference standard. Two radiologists assessed console MIPs that were created using computed tomographic (CT) data sets of 30 patients (17 men and 13 women; age range, 35–79 years; mean age, 58 years) operated for pancreatic tumors. Semi-automated MIP images were created on a separate MDCT console. Two blinded radiologist (R1, R2) and surgeons (S1, S2) evaluated the image data independently for vascular involvement and tumor resectability. The image quality and diagnostic confidence for MIPs were graded on a 5-point scale (1 = poor, 2 = suboptimal, 3 = intermediate, 4 = good; 5 = excellent) and comparison was made with 3D workstation image scores.
Results
The findings revealed greater than 90% sensitivity, specificity, and accuracy for detecting involvement of peripancreatic vessels by pancreatic tumor with an excellent interobserver agreement (κ = 0.87–1.00). The findings of console-generated MIPs were same as the findings of 3D workstation images. The mean of image quality and diagnostic confidence grading for console MIPs by assessors were 4.4 and 4.2, respectively. The average time to generate simple MIPs at the console was 3.4 minutes (range, 2.3–4.4) compared to 26 minutes (range, 18–33) to create images at the 3D workstation.
Conclusion
Semi-automated MIPs generated from an MDCT scanner console is an excellent alternative to 3D workstation images for assessing resectability of pancreatic tumor based on vascular involvement. Console MIPs can be quickly generated during the time of scan and thus can improve CT workflow.
Computed tomography (CT) is highly reliable for tumor staging and the determination of resectability and prognosis of pancreatic carcinoma ( ). It is critical to ensure that potentially resectable or unresectable tumors be correctly identified to appropriately present either surgical options in resectable patients or curative alternatives in unresectable cases.
Multidetector computed tomography (MDCT) provides technical advantages such as shorter image acquisition time and isotropic voxel resolution ( ). In addition, post-processed two- and three-dimensional (2D and 3D) images, such as maximum intensity projection (MIP) and volume rendering (VR) from MDCT scans, are superior and facilitate more accurate assessment of tumor resectability ( ). Previous studies have revealed that greater than 50% encasement of the portal vein (PV) or the superior mesenteric vein (SMV) by the pancreatic tumor with or without its compression is suggestive of vessel involvement, and MIP images obtained perpendicular to the axis of the PV provides a better plane to assess vessel involvement ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
MDCT Technique
Get Radiology Tree app to read full this article<
Image Postprocessing
Console MIPs
Get Radiology Tree app to read full this article<
Table 1
Reconstruction Protocol for MIPs Created at the MDCT Scanner Console
View Slice Thickness (mm) Overlap (mm) Field of View (cm) No. of Images Axial (with decreased field of view) 5 2.5 27 23 Coronal 5 2.5 30 26 Oblique coronals (perpendicular to PV) 5 2.5 32 26 Oblique coronals (parallel to pancreatic body) 5 2.5 36 26 Sagittal (for celiac trunk and SMA origin) 5 2.5 36 26
MDCT: multidetector computed tomography; MIP: maximum intensity projection; PV: portal vein; SMA: superior mesenteric artery.
Get Radiology Tree app to read full this article<
Image Processing: 3D Workstation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Standard of Reference
Get Radiology Tree app to read full this article<
Time for Image Generation
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Surgery and Histopathology
Get Radiology Tree app to read full this article<
Console MIP Evaluation
Get Radiology Tree app to read full this article<
Table 2
Evaluation of Vascular Involvement on Review of Console MIP Images Generated from Preoperative 16-Slice MDCT Data Sets of 30 Patients with Pancreatic Malignancies (involved vessels = 21/161)
Blood Vessel Surgery Radiologist 1 ⁎ Radiologist 2 † No. of R/U on Surgery GDA 3 3 3 R ( n = 2); U ( n = 1) Hepatic artery 5 5 5 U ( n = 5) SMA 2 2 0 U ( n = 2) Celiac Trunk 0 0 0 — SMV 5 6 ‡ 5 U ( n = 4); R ( n = 1) Portal vein 5 6 ‡ 5 U ( n = 4) Splenic artery 0 0 0 — Splenic vein 1 1 1 R ( n = 1) Total 21 23 19 —
GDA: gastroduodenal artery; MDCT: multidetector computed tomography; MIP: maximum intensity projection; R: resectable; SMA: superior mesenteric artery; SMV: superior mesenteric vein; U: unresectable.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
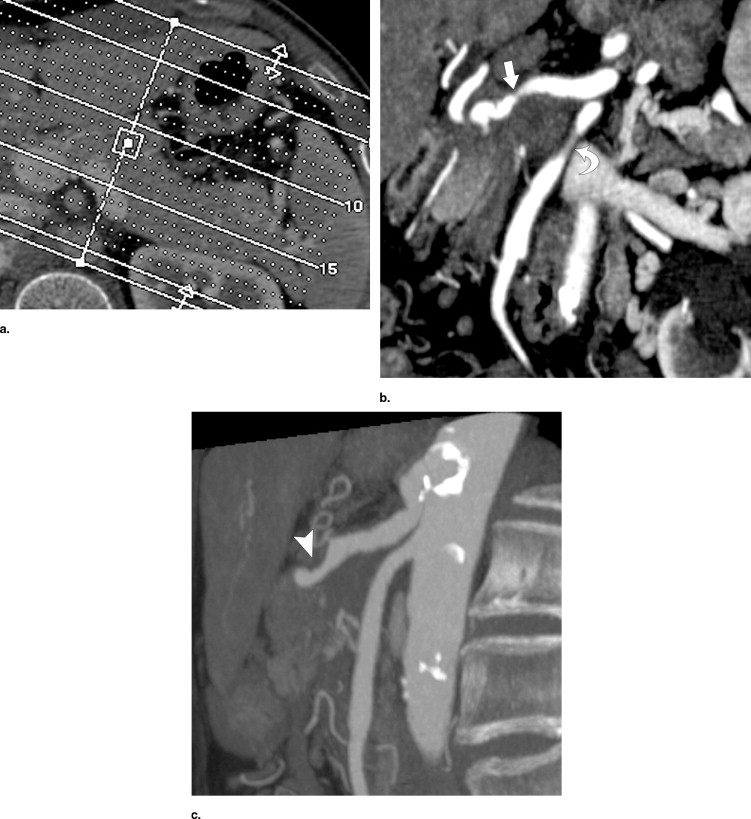
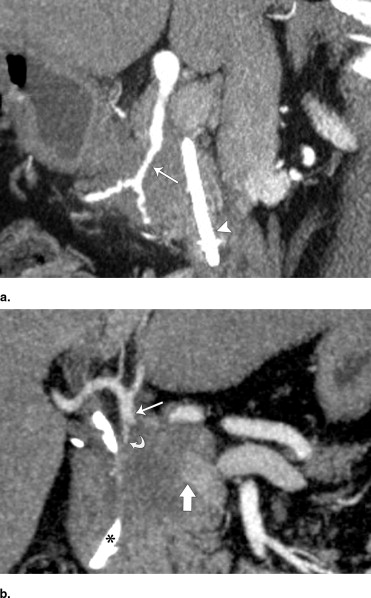
Table 3
Interobserver Agreement of Both Radiologists for Evaluation of Tumor Resectability and Important Vessel Involvements on Review of Console MIPs ⁎
Criterion κ Value 95% Confidence Interval Resectability 1.00 Not estimable Portal vein 0.87 0.62–1.00 Superior mesenteric vein 0.89 0.68–1.00 Hepatic artery 1.00 Not estimable
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Qualitative Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Time Spent in Image Generation
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Table 4
Statistical Evaluation of Vascular Involvement Detection on Console MIPs in 30 Patients with Pancreatic Malignancies ⁎
Variable R1, % 95% CI R2, % 95% CI Sensitivity 100 (21/21) 83.9–100 90.4 (19/21) 69.6–98.8 Specificity 98.5 (138/140) 94.9–99.8 100 (140/140) 97.3–100 Accuracy 98.7 (159/161) — 98.7 (159/161) — PPV 91 (21/23) — 100 (19/19) — NPV 100 (138/138) — 98 (140/142) —
CI: confidence interval; NPV: negative predictive value; PPV: positive predictive value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Freeny P.C., Marks W.M., Ryan J.A., Traverso L.W.: Pancreatic ductal adenocarcinoma: Diagnosis and staging with dynamic CT. Radiology 1988; 166: pp. 125-133.
2. Warshaw A.L., Fernandez-del Castillo C.: Pancreatic carcinoma. N Engl J Med 1992; 326: pp. 455-465.
3. Del Frate C., Zanardi R., Mortele K., Ros P.R.: Advances in imaging for pancreatic disease. Curr Gastroenterol Rep 2002; 4: pp. 140-148.
4. Schima W., Fugger R.: Evaluation of focal pancreatic masses: Comparison of mangafodipir-enhanced MR imaging and contrast-enhanced helical CT. Eur Radiol 2002; 12: pp. 2998-3008.
5. Fletcher J.G., Wiersema M.J., Farrell M.A., et. al.: Pancreatic malignancy: Value of arterial, pancreatic, and hepatic phase imaging with multi-detector row CT. Radiology 2003; 229: pp. 81-90.
6. Bluemke D.A., Cameron J.L., Hruban R.H., et. al.: Potentially resectable pancreatic adenocarcinoma: Spiral CT assessment with surgical and pathologic correlation. Radiology 1995; 197: pp. 381-385.
7. Diehl S.J., Lehmann K.J., Sadick M., Lachmann R., Georgi M.: Pancreatic cancer: Value of dual-phase helical CT in assessing resectability. Radiology 1998; 206: pp. 373-378.
8. Fishman E.K., Horton K.M., Urban B.A.: Multidetector CT angiography in the evaluation of pancreatic carcinoma: Preliminary observations. J Comput Assist Tomogr 2000; 24: pp. 849-853.
9. Tunaci M.: Multidetector row CT of the pancreas. Eur J Radiol 2004; 52: pp. 18-30.
10. Kirchgeorg M.A., Prokop M.: Increasing spiral CT benefits with post-processing applications. Eur J Radiol 1998; 28: pp. 39-54.
11. Raptopoulos V., Steer M.L., Sheiman R.G., et. al.: The use of helical CT and CT angiography to predict vascular involvement from pancreatic cancer: Correlation with findings at surgery. AJR Am J Roentgenol 1997; 168: pp. 971-977.
12. Loyer E.M., David C.L., Dubrow R.A., Evans D.B., Charnsangavej C.: Vascular involvement in pancreatic adenocarcinoma: Reassessment by thin-section CT. Abdom Imaging 1996; 21: pp. 202-206.
13. Harrison L.E., Brennan M.F.: Portal vein resection for pancreatic adenocarcinoma. Surg Oncol Clin N Am 1998; 7: pp. 165-181.
14. Gay S.B., Sobel A.H., Young L.Q., Dwyer S.J.: Process involved in reading imaging studies: Workflow analysis and implications for workstation development. J Digit Imaging 2002; 15: pp. 171-177. discussion 170
15. Hwang N.H.: You’ve got mail. J Leg Med 2004; 25: pp. 469-484.
16. Lougheed T.: Radiologists get that long distance feeling. CMAJ 2004; 170: pp. 1523.
17. Brugel M., Link T.M., Rummeny E.J., et. al.: Assessment of vascular invasion in pancreatic head cancer with multislice spiral CT: Value of multiplanar reconstructions. Eur Radiol 2004; 14: pp. 1188-1195.
18. Vargas R., Nino-Murcia M., Trueblood W., Jeffrey R.B.: MDCT in pancreatic adenocarcinoma: Prediction of vascular invasion and resectability using a multiphasic technique with curved planar reformations. AJR Am J Roentgenol 2004; 182: pp. 419-425.
19. Soyer P., Heath D., Bluemke D.A., Choti M.A., et. al.: Three-dimensional helical CT of intrahepatic venous structures: Comparison of three rendering techniques. J Comput Assist Tomogr 1996; 20: pp. 122-127.
20. Johnson P.T., Heath D.G., Kuszyk B.S., Fishman E.K.: CT angiography with volume rendering: Advantages and applications in splanchnic vascular imaging. Radiology 1996; 200: pp. 564-568.
21. Nino-Murcia M., Tamm E.P., Charnsangavej C., Jeffrey R.B.: Multidetector-row helical CT and advanced postprocessing techniques for the evaluation of pancreatic neoplasms. Abdom Imaging 2003; 28: pp. 366-377.
22. Marks M.P., Napel S., Jordan J.E., Enzmann D.R.: Diagnosis of carotid artery disease: Preliminary experience with maximum-intensity-projection spiral CT angiography. AJR Am J Roentgenol 1993; 160: pp. 1267-1271.
23. Jaffe T.A., Martin L.C., Thomas J., et. al.: Small-bowel obstruction: Coronal reformations from isotropic voxels at 16-section multi-detector row CT. Radiology 2006; 238: pp. 135-142.
24. Jaffe T.A., Nelson R.C., Johnson G.A., et. al.: Optimization of multiplanar reformations from isotropic data sets acquired with 16-detector row helical CT scanner. Radiology 2006; 238: pp. 292-299.
25. Singh A.K., Sahani D.V., Kagay C.R., et. al.: Semiautomated MIP images created directly on 16-section multidetector CT console for evaluation of living renal donors. Radiology 2007; 244: pp. 583-590.