
Rationale and Objectives
Hyperpolarized (HP) gas magnetic resonance imaging (MRI) is an advanced imaging technique that provides high-resolution regional information on lung function without using ionizing radiation. Before this modality can be considered for assessing clinical or investigational interventions, baseline repeatability needs to be established. We assessed repeatability of lung function measurement using HP helium-3 MRI (HP 3 He MRI) in a small cohort of patients with cystic fibrosis (CF).
Materials and Methods
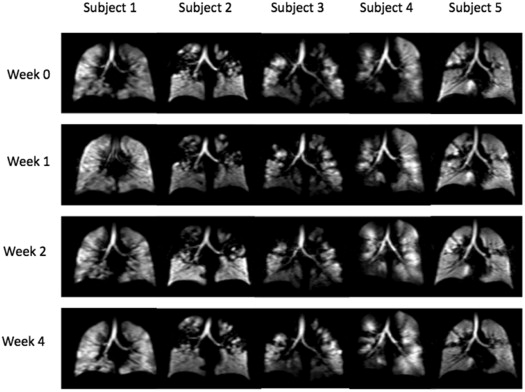
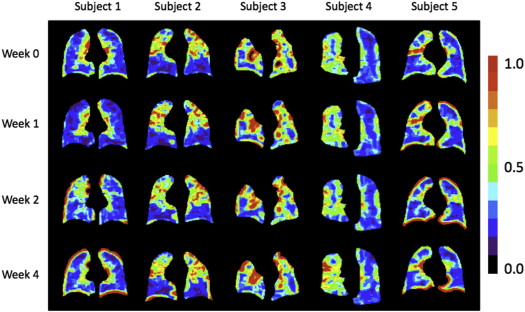
We examined repeatability of HP 3 He MR images of five patients with CF in four scanning sessions over a 4-week period. We acquired images on a Philips 3.0 Tesla Achieva MRI scanner using a quadrature, flexible, wrap-around, 3 He radiofrequency coil with a fast gradient-echo pulse sequence. We determined ventilation volume and ventilation defect volume using an advanced semiautomatic segmentation algorithm and also quantified ventilation heterogeneity.
Results
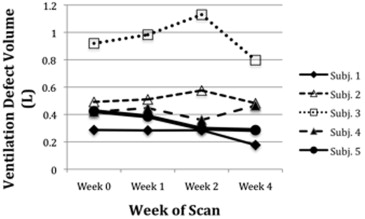
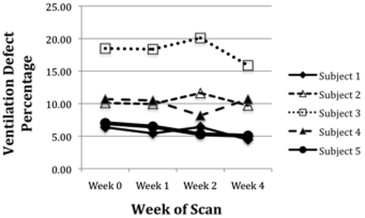
There were no significant differences in total ventilation volume, ventilation defect volume, ventilation defect percentage, or mean ventilation heterogeneity (repeated-measures analysis of variance, P = .2116, P = .2825, P = .2871, and P = .7265, respectively) in the patients across the four scanning sessions.
Conclusions
Our results indicate that total ventilation volume, ventilation defect volume, ventilation defect percentage, and mean ventilation heterogeneity as assessed by HP gas MRI in CF patients with stable health are reproducible over time. This repeatability and the technique’s capability to provide noninvasive high-resolution data on regional lung function without ionizing radiation make 3 He MRI a potentially useful outcome measure for CF-related clinical trials.
Cystic fibrosis (CF) is a potentially fatal genetic disease caused by defects of the cystic fibrosis transmembrane conductance regulator (CFTR) protein coded by the CFTR gene, leading to impaired chloride ion transport . Although there have been major advances in CF health care over the past 20 years, CF still negatively affects quality of life and considerably shortens life expectancy, and thus there is still a desire for new CF therapies. It is acknowledged that improved end points for clinical trials are needed for further development of treatments .
Currently, the most common outcome measures for CF-related trials are pulmonary function tests (PFTs) to assess lung function and high-resolution computed tomography (HRCT) for anatomic imaging measurements. Other common study end points include frequency of pulmonary exacerbations, quality of life, and chest radiographs. All these measures are limited by not providing regional information on lung function and by being unable to detect subtle changes in function that could be used for early detection and assessment of therapy efficacy . There are exciting advances being made with CT imaging of structural changes in early-stage CF by the Australian Respiratory Early Surveillance Team (AREST) CF group in Australia , but the ionizing radiation associated with HRCT poses risks when used repeatedly over time, especially for young children . Additionally, PFTs and radiographs cannot detect early stages of lung disease or accurately measure the progression of disease . Therefore, there is a need for a measurement modality that can provide sensitive data on regional lung function, help assess status of lung disease at early stages, assist with care planning, and assess the efficacy of novel treatments, without the use of ionizing radiation .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Evaluation of Repeatability
Get Radiology Tree app to read full this article<
Table 1
Pulmonary Function Test Data and HP 3 He Ventilation Imaging Data for the Five Patients for the Four Scanning Sessions (Week 0 = Baseline).
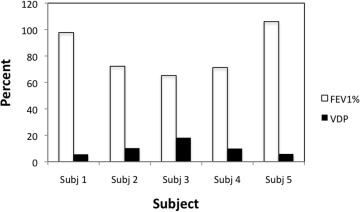
FEV 1 % NS FEV 1 NS FVC NS VV NS VDV NS VDP NS Subject 1 Week 0 98.00 3.40 4.25 4.19 0.29 6.37 Week 1 98.00 3.42 4.20 4.94 0.28 5.43 Week 2 96.00 3.35 4.11 4.16 0.28 6.41 Week 4 99.00 3.44 4.15 3.78 0.18 4.47 Subject 2 Week 0 70.00 2.95 3.81 4.38 0.49 10.10 Week 1 74.00 3.13 4.03 4.62 0.51 9.94 Week 2 72.00 3.03 3.98 4.38 0.58 11.62 Week 4 73.00 3.07 3.97 4.48 0.48 9.72 Subject 3 Week 0 63.00 3.18 4.63 4.06 0.92 18.48 Week 1 63.00 3.18 4.66 4.37 0.98 18.36 Week 2 67.00 3.37 4.97 4.49 1.13 20.09 Week 4 68.00 3.42 5.01 4.22 0.80 15.88 Subject 4 Week 0 72.00 2.04 3.01 3.50 0.42 10.69 Week 1 72.00 2.04 3.10 3.82 0.45 10.48 Week 2 70.00 2.00 3.16 4.05 0.36 8.17 Week 4 71.00 2.01 3.04 3.89 0.47 10.69 Subject 5 Week 0 105.00 4.43 5.09 5.64 0.42 7.00 Week 1 105.00 4.42 5.00 5.58 0.39 6.47 Week 2 111.00 4.69 5.28 5.28 0.30 5.31 Week 4 103.00 4.44 5.06 5.37 0.29 5.06
FEV 1 , forced expiratory volume in 1 second; FVC, forced vital capacity; VDP, ventilation defect percentage; VDV, ventilation defect volume; VV, total ventilation volume; NS, no significant difference found with repeated-measures analysis of variance.
Get Radiology Tree app to read full this article<
Comparison with Other Measures
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. O’Sullivan B.P., Freedman S.D.: Cystic fibrosis. Lancet 2009; 373: pp. 1891-1904.
2. Hoffman L.R., Ramsey B.W.: Chest 2013; 143: pp. 207-213.
3. Ramsey B.W.: Proc Am Thorac Soc 2007; 4: pp. 367-369.
4. Woodhouse N., Wild J.M., van Beek E.J., et. al.: Assessment of hyperpolarized 3 He lung MRI for regional evaluation of interventional therapy: a pilot study in pediatric cystic fibrosis. J Magn Reson Imaging 2009; 30: pp. 981-988.
5. Brody A.S., Frush D.P., Huda W., et. al., American Academy of Pediatrics, Section on Radiology: Radiation risk to children from computed tomography. Pediatrics 2007; 120: pp. 677-682.
6. Brody A.S., Klein J.S., Molina P.L., et. al.: High resolution computed tomography in young patients with cystic fibrosis: distribution of abnormalities and correlation with pulmonary function tests. J Pediatr 2004; 145: pp. 32-38.
7. Sly P.D., Gangell C.L., Chen L., et. al.: Risk factors for bronchiectasis in children with cystic fibrosis. N Engl J Med 2013; 368: pp. 1963-1970.
8. Albert M.S., Cates G.D., Driehuys B., et. al.: Biological magnetic resonance imaging using laser-polarized 129Xe. Nature 1994; 370: pp. 199-201.
9. Mentore K., Froh D.K., de Lange E.E., et. al.: Hyperpolarized He3 MRI of the lung in cystic fibrosis: assessment at baseline and after bronchodilator and airway clearance treatment. Acad Radiol 2005; 12: pp. 1423-1429.
10. Koumellis P., van Beek E.J., Woodhouse N., et. al.: Quantitative analysis of regional airways obstruction using dynamic hyperpolarized 3He MRI-preliminary results in children with cystic fibrosis. J Magn Reson Imaging 2005; 22: pp. 420-426.
11. Altes T.A., Eichinger M., Puderbach M.: Magnetic resonance imaging of the lung in cystic fibrosis. Proc Am Thorac Soc 2007; 4: pp. 321-327.
12. van Beek E.J., Hill C., Woodhouse N., et. al.: Assessment of lung disease in children with cystic fibrosis using hyperpolarized 3-Helium MRI: comparison with Shwachman score, Chrispin-Norman score and spirometry. Eur Radiol 2007; 17: pp. 1018-1024.
13. Sun Y., O’Sullivan B.P., Roche J.P., et. al.: Using hyperpolarized 3 He MRI to evaluate treatment efficacy in cystic fibrosis patients. J Magn Reson Imaging 2011; 34: pp. 1206-1211.
14. de Lange E.E., Altes T.A., Patrie J.T., et. al.: Evaluation of asthma with hyperpolarized helium-3 MRI: correlation with clinical severity and spirometry. Chest 2006; 130: pp. 1055-1062.
15. Evans A., McCormack D.G., Santyr G., et. al.: Mapping and quantifying hyperpolarized 3He magnetic resonance imaging apparent diffusion coefficient gradients. J Appl Physiol 2008; 105: pp. 693-699.
16. Tzeng Y.S., Hoffman E., Maurer R., et. al.: Comparison of airway diameters measurements from an anthropomorphic airway tree phantom using hyperpolarized 3He MRI and high resolution computed tomography. Magn Reson Med 2007; 58: pp. 636-642.
17. Tzeng Y.S., Hoffman E., Cook-Granroth J., et. al.: Investigation of hyperpolarized 3He magnetic resonance imaging utility in examining human airway diameter behavior in asthma through comparison with high-resolution computed tomography. Acad Radiol 2008; 15: pp. 799-808.
18. Campana L., Kenyon J., Zhalehdoust-Sani S., et. al.: Probing airway conditions governing ventilation defects in asthma via hyperpolarized MRI image functional modeling. J Appl Physiol 2009; 106: pp. 1293-1300.
19. Lee E.Y., Sun Y., Zurakowski D., et. al.: Hyperpolarized 3He MR imaging of the lung: normal range of ventilation defects and PFT correlation in young adults. J Thorac Imaging 2009; 24: pp. 110-114.
20. Mullally W., Betke M., Albert M., et. al.: Explaining clustered ventilation defects via a minimal number of airway closure locations. Ann Biomed Eng 2009; 37: pp. 286-300.
21. Sun Y., Butler J.P., Lindholm P., et. al.: Marked pericardial inhomogeneity of specific ventilation at total lung capacity and beyond. Respir Physiol Neurobiol 2009; 169: pp. 44-49.
22. Kirby M., Mathew L., Wheatley A., et. al.: Chronic obstructive pulmonary disease: longitudinal hyperpolarized (3)He MR imaging. Radiology 2010; 256: pp. 280-289.
23. Fain S., Schiebler M.L., McCormack D.G., et. al.: Imaging of lung function using hyperpolarized helium-3 magnetic resonance imaging: review of current and emerging translational methods and applications. J Magn Reson Imaging 2010; 32: pp. 1398-1408.
24. Lilburn D.M., Pavlovskaya G.E., Meersmann T.: Perspectives of hyperpolarized noble gas MRI beyond (3)He. J Magn Reson 2013; 229: pp. 173-186.
25. Kirby M., Svenningsen S., Ahmed H., et. al.: Quantitative evaluation of hyperpolarized helium-3 magnetic resonance imaging of lung function variability in cystic fibrosis. Acad Radiol 2011; 18: pp. 1006-1013.
26. Kirby M., Heydarian M., Svenningsen S., et. al.: Hyperpolarized 3He magnetic resonance functional imaging semiautomated segmentation. Acad Radiol 2012; 19: pp. 141-152.
27. Heydarian M, Kirby M, Choy S, et al. Semi-automated segmentation of pulmonary ventilation using hyperpolarized 3He magnetic resonance imaging. Biomedical Engineering Society Annual Meeting 2010 Imaging the Lung - The New Frontier [PS-8A-14–190]. 10.
28. Lui J.K., Laprad A.S., Parameswaran H., et. al.: Statistically robust and semiautomatic quantification of ventilation from static hyperpolarized 3He MRI: application to asthma. American Thoracic Society abstract 2009;
29. Tzeng Y.S., Lutchen K., Albert M.: The difference in ventilation heterogeneity between asthmatic and healthy subjects quantified using hyperpolarized 3 He MRI. J Appl Physiol 2009; 106: pp. 813-822.
30. Tustison N.J., Altes T.A., Song G., et. al.: Feature analysis of hyperpolarized helium-3 pulmonary MRI: a study of asthmatics versus nonasthmatics. Magn Reson Med 2010; 63: pp. 1448-1455.
31. van Beek E.J., Dahmen A.M., Stavngaard T., et. al.: Hyperpolarized 3He MRI versus HRCT in COPD and normal volunteers: PHIL trial. Eur Respir J 2009; 34: pp. 1311-1321.
32. Ireland R.H., Woodhouse N., Hoggard N., et. al.: An image acquisition and registration strategy for the fusion of hyperpolarized helium-3 and x-ray CT images of the lung. Phys Med Biol 2008; 53: pp. 6055-6063.
33. Bannier E., Cieslar K., Mosbah K., et. al.: Hyperpolarized 3He MR for sensitive imaging of ventilation function and treatment efficiency in young cystic fibrosis patients with normal lung function. Radiology 2010; 255: pp. 225-232.
34. Meyer K.C., Sharma A.: Regional variability of lung inflammation in cystic fibrosis. Am J Respir Crit Care Med 1997; 156: pp. 1536-1540.
35. Kirby M., Svenningsen S., Owrangi A., et. al.: Hyperpolarized 3He and 129Xe MR imaging in healthy volunteers and patients with chronic obstructive pulmonary disease. Radiology 2012; 265: pp. 600-610.