
Rationale and Objectives
To assess the performance of automated quantification of left ventricular function and mass based on heart deformation analysis (HDA) in asymptomatic older adults.
Materials and Methods
This study complied with Health Insurance Portability and Accountability Act regulations. Following the approval of the institutional review board, 160 asymptomatic older participants were recruited for cardiac magnetic resonance imaging including two-dimensional cine images covering the entire left ventricle in short-axis view. Data analysis included the calculation of left ventricular ejection fraction (LVEF), left ventricular mass (LVM), and cardiac output (CO) using HDA and standard global cardiac function analysis (delineation of end-systolic and end-diastolic left ventricle epi- and endocardial borders). The agreement between methods was evaluated using intraclass correlation coefficient (ICC) and coefficient of variation (CoV).
Results
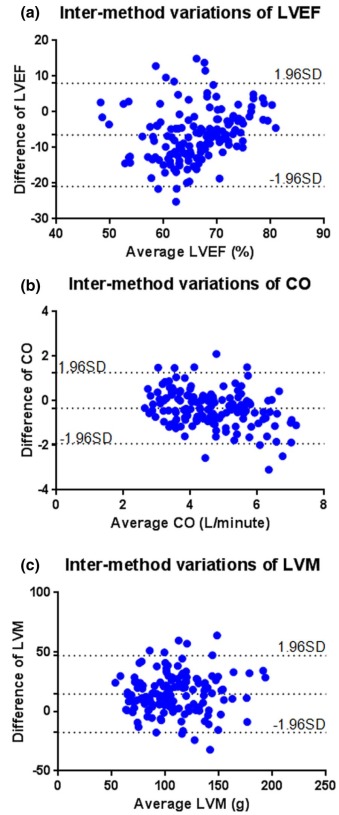
HDA had a shorter processing time than the standard method (1.5 ± 0.3 min/case vs. 5.8 ± 1.4 min/case, P < 0.001). There was good agreement for LVEF (ICC = 0.552, CoV = 10.5%), CO (ICC = 0.773, CoV = 13.5%), and LVM (ICC = 0.859, CoV = 14.5%) acquired with the standard method and HDA. There was a systemic bias toward lower LVEF (62.8% ± 8.3% vs. 69.3% ± 6.7%, P < 0.001) and CO (4.4 ± 1.0 L/min vs. 4.8 ± 1.3 L/min, P < 0.001) by HDA compared to the standard technique. Conversely, HDA overestimated LVM (114.8 ± 30.1 g vs. 100.2 ± 29.0 g, P < 0.001) as compared to the reference method.
Conclusions
HDA has the potential to measure LVEF, CO, and LVM without the need for user interaction based on standard cardiac two-dimensional cine images.
Introduction
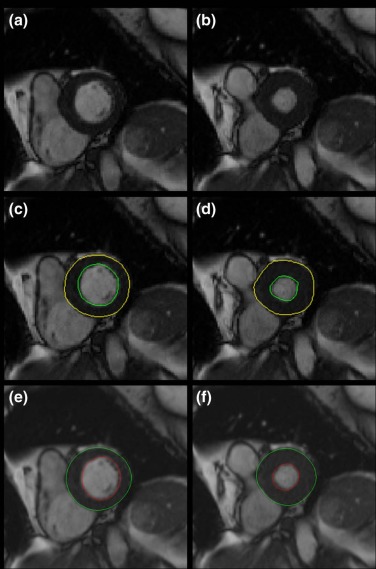
Cardiac aging, which can result in subclinical alterations in the heart, is considered a condition that bridges elderly patients and the incidence of cardiovascular events. At the same time, co-existing cardiovascular confounders, such as diabetes mellitus (DM) and hypertension (HTN), can further contribute to the development of cardiac aging. Left ventricular (LV) ejection fraction (LVEF) and LV mass (LVM) are indices presenting ventricular dysfunction and hypertrophy, two important indicators in cardiovascular risk estimation. In clinical practice, two-dimensional (2D) cine magnetic resonance imaging (MRI) has been adopted as a standard method for the measurement of LVEF and LVM. Balanced steady-state free processing (b-SSFP) is a commonly used MRI technique for the acquisition of cine MRI images at short-axis view because it provides good blood-myocardium contrasts . Generally, endocardial and epicardial borders of the LV are determined automatically or manually for each slice/phase of MRI based on signal differences among blood pool, LV wall, and outer structures. LV volumes at each cardiac phase will be obtained by summing up the LV areas in all slices covering the heart from the base to the apex. End systole and end diastole can be identified to define the smallest and the largest LV volumes, respectively, for the calculation of LVEF and cardiac output (CO). LV myocardial volume will be calculated by adding up the LV areas in each slice at end diastole and end systole. LVM can therefore be calculated by assuming a reasonable myocardial density.
Heart deformation analysis (HDA) is a recently developed image processing technique for the description of global and regional myocardial function and motion on cine MRI. Using a deformation image registration (DIR) algorithm, HDA is able to automatically track the shape of the LV through the entire cardiac cycle by calculating deformation fields (forward and backward) of myocardium tissue among sequential cardiac time frames . As such, global cardiac indices (LVEF, CO, and LVM) as well as regional myocardial motion indices (displacement, velocity, strain, and strain rate) can be extracted from cine images using a semiautomatic “one-stop-shop” analysis with minimal user interaction. However, to date, the capability of the HDA tool to evaluate LV global function and morphology has not been validated in a larger clinical study cohort. Therefore, the aim of the present study was to assess the accuracy of automated quantification of left ventricular function and mass based on HDA in asymptomatic older adults by using a standard LV global function analysis as the reference standard.
Materials and Methods
Study Participants
Get Radiology Tree app to read full this article<
Table 1
Description of Participants
Subjects ( N = 160) Male (%) 97 (60) Age (years) 72.0 ± 4.1 Weight (kg) 86.3 ± 17.8 Height (cm) 172.1 ± 9.8 BMI 28.9 ± 5.8 Heart rate (beats/min) 69.7 ± 10.2 DM (%) 39 (24) HTN (%) 57 (36)
BMI, body mass index. DM, diabetes mellitus. HTN, hypertension.
Get Radiology Tree app to read full this article<
MRI Facility
Get Radiology Tree app to read full this article<
Cine MRI Scan Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Processing
Standard Cine Image Processing
Get Radiology Tree app to read full this article<
HDA Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Processing and Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
The Differences of LVEF, CO, and LVM Measured with the HDA Tool and the Existing Method (Using Paired t Tests)
Processing Time (Min) LVEF (%) CO (L/min) LVM (g) HDA 1.5 ± 0.3 62.8 ± 8.3 4.4 ± 1.0 114.8 ± 30.1 Reference method 5.8 ± 1.4 69.3 ± 6.7 4.8 ± 1.3 100.2 ± 29.0P values <0.001 <0.001 <0.001 <0.001
CO, cardiac output; HDA, heart deformation analysis; LVEF, left ventricular ejection fraction; LVM, left ventricular mass.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Tyler D.J., Hudsmith L.E., Petersen S.E., et. al.: Cardiac cine MR-imaging at 3T: FLASH vs SSFP. J Cardiovasc Magn Reson 2006; 8: pp. 709-715.
2. Guetter C., Xue H., Chefd’hotel C., et. al.: Efficient symmetric and inverse-consistent deformable registration through interleaved optimization. Biomedical Imaging: From Nano to Macro, 2011 IEEE International Symposium on2011.pp. 590-593.
3. Jolly M.-P., Guetter C., Lu X., et. al.: Statistical atlases and computational models of the heart imaging and modelling challenges.Camara O.Konukoglu E.Pop M. et. al.Automatic segmentation of the myocardium in cine MR images using deformable registration.2012.Springerpp. 98-108.
4. Pirzada A., Reid K., Kim D., et. al.: Chicago Healthy Aging Study: objectives and design. Am J Epidemiol 2013; 178: pp. 635-644.
5. Sievers B., Kirchberg S., Bakan A., et. al.: Impact of papillary muscles in ventricular volume and ejection fraction assessment by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2004; 6: pp. 9-16.
6. MacDonald K.A., Kittleson M.D., Reed T., et. al.: Quantification of left ventricular mass using cardiac magnetic resonance imaging compared with echocardiography in domestic cats. Vet Radiol Ultrasound 2005; 46: pp. 192-199.
7. Kuhl H.P., Bucker A., Franke A., et. al.: Transesophageal 3-dimensional echocardiography: in vivo determination of left ventricular mass in comparison with magnetic resonance imaging. J Am Soc Echocardiogr 2000; 13: pp. 205-215.
8. Bottini P.B., Carr A.A., Prisant L.M., et. al.: Magnetic resonance imaging compared to echocardiography to assess left ventricular mass in the hypertensive patient. Am J Hypertens 1995; 8: pp. 221-228.
9. Phatak N.S., Maas S.A., Veress A.I., et. al.: Strain measurement in the left ventricle during systole with deformable image registration. Med Image Anal 2009; 13: pp. 354-361.
10. Boldea V., Sharp G.C., Jiang S.B., et. al.: 4D-CT lung motion estimation with deformable registration: quantification of motion nonlinearity and hysteresis. Med Phys 2008; 35: pp. 1008-1018.
11. Schuster A., Kutty S., Padiyath A., et. al.: Cardiovascular magnetic resonance myocardial feature tracking detects quantitative wall motion during dobutamine stress. J Cardiovasc Magn Reson 2011; 13: pp. 58.
12. Gottdiener J.S., Bednarz J., Devereux R., et. al.: American Society of Echocardiography recommendations for use of echocardiography in clinical trials. J Am Soc Echocardiogr 2004; 17: pp. 1086-1119.
13. Schlosser T., Pagonidis K., Herborn C.U., et. al.: Assessment of left ventricular parameters using 16-MDCT and new software for endocardial and epicardial border delineation. AJR Am J Roentgenol 2005; 184: pp. 765-773.
14. Seo H.Y., Lee S.P., Park J.B., et. al.: Discrepancies in left ventricular mass calculation based on echocardiography and cardiovascular magnetic resonance measurements in patients with left ventricular hypertrophy. J Am Soc Echocardiogr 2015; 28: pp. 1194-1203.
15. Bellenger N.G., Marcus N.J., Rajappan K., et. al.: Comparison of techniques for the measurement of left ventricular function following cardiac transplantation. J Cardiovasc Magn Reson 2002; 4: pp. 255-263.