
Rationale and Objectives
This study aimed to determine the average time for breast radiologists of varied experience to interpret automated breast ultrasound (ABUS) examinations.
Materials and Methods
A reader performance study was conducted on female patients, with ACR BI-RADS 4 breast density classifications of C or D, who received both an ABUS screening examination and a digital mammogram from 2013 to 2014 at an academic institution. Three faculty breast radiologists with varied levels of ABUS experience (advanced, intermediate, novice) read all ABUS examinations, with interpretation times and final impressions (categorized as “normal” or “abnormal”) recorded for each examination.
Results
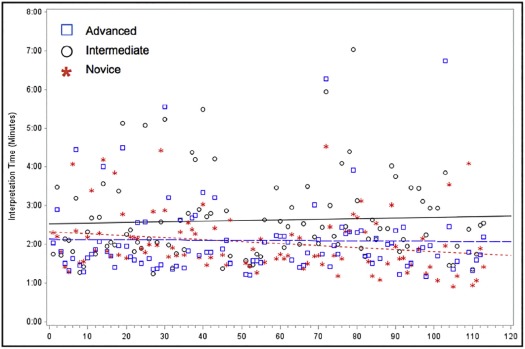
Ninety-nine patients were included, with all readers demonstrating an average ABUS interpretation time of less than 3 minutes. Compared to the other two readers, the intermediate reader had a significantly longer mean interpretation time at 2.6 minutes (95% confidence interval 2.4–2.8; P < .001). In addition to having the shortest mean interpretation time, the novice reader also demonstrated reduced times in subsequent interpretations, with a significant decrease in interpretation times of 3.1 seconds (95% confidence interval 0.4–5.8) for every 10 ABUS examinations interpreted ( P < .05).
Conclusions
Overall, mean ABUS interpretation time by radiologists of all experience levels was short, at less than 3 minutes per examination, which should not deter radiologists from incorporating ABUS examinations into a busy clinical environment.
Introduction
Although overall breast cancer-related mortality has steadily decreased over the last 30 years, in part due to major advances in mammographic screening, it remains a leading cause of death among US women . The sensitivity of screening mammography has been shown to be as low as 30%–48% in patients with dense breasts, which constitute nearly 50% of the screening population , because of a masking effect by the density for cancer visualization . Moreover, breast density is a strong, independent risk factor for the development of breast cancer, with studies demonstrating an increased lifetime risk of 2.8–6.0 times that of women with less dense, fatty breast tissue and a 6.1–17.8 greater risk of interval cancers in women with extremely dense breasts . Supplemental breast cancer screening with handheld ultrasound has documented an increased detection rate of approximately three to four cancers per thousand women with dense breasts, and, as 85% of cancers detected by screening ultrasound alone are invasive and node negative, ultrasound has become a particularly appealing method of screening . Although ultrasound can help address the challenges of cancer detection in dense breasts, traditional handheld ultrasound has several important limitations, including operator dependency, variable scan quality and reproducibility, and long acquisition times, which raise concerns for broad-scale implementation as an adjunct breast cancer screening tool .
Automated breast ultrasound (ABUS), which is a US Food and Drug Administration–approved adjunct-screening tool specifically for women with dense breast tissue , has the potential to overcome several limitations of handheld screening ultrasound because it acquires three-dimensional (3D) volumes viewable in three orthogonal planes, reducing operator variability and subjectivity . However, as alternative screening methodologies such as ABUS are gaining popularity, questions have been raised regarding time required for radiologist interpretation of the ABUS examination. Typical acquisition time for ABUS volumes is approximately 6 minutes in 20- to 30-minute examination slots, which compares favorably to typical 30-minute slots for handheld ultrasound examinations . Additionally, both mammography technologists and sonographers of varying skill levels can be trained to acquire ABUS images, obviating the need for highly trained ultrasound technologists who perform large-scale handheld ultrasound screenings .
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics ( n = 99)
Characteristic Value Mean age, y (SD) 56.2 (10.0) Clinical history, n (%) Prior biopsy 29 (29.3) Breast cancer 9 (9.1) Prior lumpectomy 9 (9.1) Breast radiation 8 (8.1) Prior augmentation 2 (2.0) Prior reduction 3 (3.0) Breast density, n (%) Category C 76 (76.8) Category D 23 (23.2)
SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
ABUS Examination Interpretation Times by Radiologist
Radiologist Mean Time, min (SD) 95% Confidence Interval Novice 2.0 (0.8) 1.9–2.2 Intermediate 2.6 \* (1.1) 2.4–2.8 Advanced 2.1 (1.0) 1.9–2.3
ABUS, automated breast ultrasound; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. National Cancer Institute : SEER Stat Fact Sheets: breast cancer. Available at http://seer.cancer.gov/statfacts/html/breast.html
2. Checka C.M., Chun J.E., Schnabel F.R., et. al.: The relationship of mammographic density and age: implications for breast cancer screening. Am J Roentgenol 2012; 198: pp. W292-W295.
3. Kelly K.M., Dean J., Comulada W.S., et. al.: Breast cancer detection: using automated whole breast ultrasound and mammography in radiographically dense breasts. Eur Radiol 2010; 20: pp. 734-742.
4. Giuliano V., Giuliano C.: Improved breast cancer detection in asymptomatic women using 3D-automated breast ultrasound in mammographically dense breasts. Clin Imaging 2013; 37: pp. 480-486.
5. Berg W.A., Blume J.D., Cormack J.B., et. al.: Combined screening with ultrasound and mammography vs mammography alone in women at elevated risk of breast cancer. JAMA 2008; 299: pp. 2151-2163.
6. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
7. Pisano E.D., Gastonis C., Hendrick E., et. al.: Diagnostic performance of digital versus film mammography for breast cancer screening. N Engl J Med 2005; 353: pp. 1773-1783.
8. Byrne C., Schairer C., Wolfe J., et. al.: Mammographic features and breast cancer risk: effects with time, age, and menopause status. J Natl Cancer Inst 1995; 87: pp. 1622-1629.
9. Boyd N.F., Byng J.W., Jong R.A., et. al.: Quantitative classification of mammographic densities and breast cancer risk: results from the Canadian National Breast Screening Study. J Natl Cancer Inst 1995; 87: pp. 670-675.
10. Saftlas A.F., Wolfe J.N., Hoover R.N., et. al.: Mammographic parenchymal patterns as indicators of breast cancer risk. Am J Epidemiol 1989; 129: pp. 518-526.
11. Boyd N.F., Guo H., Martin L.J., et. al.: Mammographic density and the risk and detection of breast cancer. N Engl J Med 2007; 356: pp. 227-236.
12. Harvey J.A., Bovbjerg V.E.: Quantitative assessment of mammographic breast density: relationship with breast cancer risk. Radiology 2004; 230: pp. 29-41.
13. Boyd N., Martin L., Yaffe M., et. al.: Mammographic density and breast cancer risk: current understanding and future prospects. Breast Cancer Res 2011; 13: pp. 223.
14. Freer P.: Mammographic breast density: impact on breast cancer risk and implications for screening. Radiographics 2015; 35: pp. 302-315.
15. Mandelson M.T., Oestreicher N., Porter P.L., et. al.: Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst 2000; 92: pp. 1081-1087.
16. Berg W.: Current status of supplemental screening in dense breasts. J Clin Oncol 2016; 34: pp. 1840-1843.
17. Berg W.A., Zhang Z., Lehrer D., et. al.: Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012; 307: pp. 1394-1404.
18. Buchberger W., Niehoff A., Obrist P., et. al.: Clinically and mammographically occult breast lesions: detection and classification with high-resolution sonography. Semin Ultrasound CT MR 2000; 21: pp. 325-336.
19. Corsetti V., Houssami N., Ferrari A., et. al.: Breast screening with ultrasound in women with mammography-negative dense breasts: evidence on incremental cancer detection and false positives, and associated cost. Eur J Cancer 2008; 44: pp. 539-544.
20. Crystal P., Strano S.D., Shcharynski S., et. al.: Using sonography to screen women with mammographically dense breasts. Am J Roentgenol 2003; 181: pp. 177-182.
21. Gordon P.B., Goldenberg S.L.: Malignant breast masses detected only by ultrasound. A retrospective review. Cancer 1995; 76: pp. 626-630.
22. Kolb T.M., Lichy J., Newhouse J.H.: Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology 2002; 225: pp. 165-175.
23. Berg W.A., Mendelson E.B.: Technologist-performed handheld screening breast US imaging: how is it performed and what are the outcomes to date?. Radiology 2014; 272: pp. 27.
24. Berg W.A.: Supplemental screening sonography in dense breasts. Radiol Clin North Am 2004; 42: pp. 845-851.
25. Baker J.A., Soo M.S., Breast U.S.: Assessment of technical quality and image interpretation. Radiology 2002; 223: pp. 229-238.
26. Bosch A.M., Kessels A.G., Beets G.L., et. al.: Interexamination variation of whole breast ultrasound. Br J Radiol 2003; 76: pp. 328-331.
27. Berg W.A., Blume J.D., Cormack J.B., et. al.: Training the ACRIN 6666 Investigators and effects of feedback on breast ultrasound interpretive performance and agreement in BI-RADS ultrasound feature analysis. Am J Roentgenol 2012; 199: pp. 224-235.
28. Berg W.A., Blume J.D., Cormack J.B., et. al.: Operator dependence of physician-performed whole-breast US: lesion detection and characterization. Radiology 2006; 241: pp. 355-365.
29. Tagliafico A.S., Calabrese M., Mariscotti G., et. al.: Adjunct screening with tomosynthesis or ultrasound in women with mammography-negative dense breasts: interim report of a prospective comparative trial. J Clin Oncol 2016; 34: pp. 1882-1888.
30. Wilczek B., Wilczek H., Rasouliyan L., et. al.: Adding 3D automated breast ultrasound to mammography screening in women with heterogeneously and extremely dense breasts: Report from a hospital-based, high-volume, single-center breast center screening program. Eur J Radiol 2016; 85: pp. 1554-1563.
31. US Food and Drug Administration : Premarket approval. Available at http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=7828
32. Brem R.F., Tabár L., Duffy S.W., et. al.: Assessing improvement in detection of breast cancer with three-dimensional automated breast US in women with dense breast tissue: the SomoInsight study. Radiology 2015; 274: pp. 663-673.
33. Jiang W.W., Cheng L., Li A.H., et. al.: A novel breast ultrasound system for providing coronal images: systems development and feasibility study. Ultrasonics 2015; 56: pp. 427-434.
34. Kaplan S.S.: Automated whole breast ultrasound. Radiol Clin North Am 2014; 52: pp. 539-546.
35. Giger M., Inciardi M.F., Edwards A., et. al.: Automated breast ultrasound in breast cancer screening of women with dense breasts: reader study of mammography-negative and mammography-positive cancers. Am J Roentgenol 2016; 206: pp. 1-10.
36. Scheel J.R., Lee J.M., Sprague B.L., et. al.: Screening ultrasound as an adjunct to mammography in women with mammographically dense breasts. Am J Obstet Gynecol 2015; 212: pp. 9-17.
37. Maughan K.L., Lutterbie M.A., Ham P.S.: Treatment of breast cancer. Am Fam Physician 2010; 81: pp. 1339-1346.
38. Senie R.T., Lesser M., Kinne D.W., et. al.: Method of tumor detection influence disease-free survival of women with breast carcinoma. Cancer 1994; 73: pp. 1666-1672.
39. Skaane P., Gullien R., Eben E.B., et. al.: Interpretation of automated breast ultrasound (ABUS) with and without knowledge of mammography: a reader performance study. Acta Radiol 2015; 56: pp. 404-412.
40. Chang J.M., Moon W.K., Cho N., et. al.: Breast cancers initially detected by hand-held ultrasound: detection performance of radiologists using automated breast ultrasound data. Acta Radiol 2011; 52: pp. 8-14.
41. Wang H.-Y., Jiang Y.-X., Zhu Q.-L., et. al.: Differentiation of benign and malignant breast lesions: a comparison between automatically generated breast volume scans and handheld ultrasound examinations. Eur J Radiol 2012; 81: pp. 3190-3200.
42. Wang A.T., Vachon C.M., Brandt K.R., et. al.: Breast density and breast cancer risk: a practical review. Mayo Clin Proc 2014; 89: pp. 548-557.
43. Miglioretti D.L., Gard C.C., Carney P.A., et. al.: When radiologists perform best: the learning curve in screening mammography interpretation. Radiology 2009; 253: pp. 3.
44. Bernardi D., Ciatto S., Pellegrini M., et. al.: Application of breast tomosynthesis in screening: incremental effect on mammography acquisition and reading time. Br J Radiol 2012; 85: pp. 1174-1178.
45. Ciatto S., Andreoli C., Di Maggio C.: Proficiency test in clinical mammography. Results of a consecutive series of 130 volunteer Italian radiologists. Radiol Med 1999; 98: pp. 255-258.
46. Dang P.A., Freer P.E., Humphrey K.L., et. al.: Addition of tomosynthesis to conventional digital mammography: effect on image interpretation time of screening examinations. Radiology 2014; 270: pp. 49-56.
47. Burnside E.S., Park J.M., Fine J.P., et. al.: The use of batch reading to improve the performance of screening mammography. Am J Roentgenol 2005; 185: pp. 790-796.
48. Gur D., Abrams G.S., Chough D.M., et. al.: Digital breast tomosynthesis: observer performance study. Am J Roentgen 2009; 193: pp. 586-591.