
Rationale and Objectives
Abnormal blood flow with bicuspid aortic valve (BAV) has been characterized with four-dimensional flow magnetic resonance imaging (MRI), but this approach is time consuming and requires technical expertise. We assess the relationship between different leaflets fusion patterns with BAV, eccentric systolic flow, and dilation patterns of the ascending aorta using two-dimensional (2D) phase-contrast (PC) MRI.
Materials and Methods
Fifty-nine patients with BAV who underwent cardiac MRI were identified; 47 had right–left (RL) aortic leaflet fusion and 12 had right-noncoronary (RN) fusion. Flow displacement was calculated, and patients with abnormal displacement (>0.1) were classified as either rightward or leftward. Patterns of aortopathy were determined (0–3), and correlation between leaflet fusion, flow direction, aortopathy type, and other clinical parameters was performed with Pearson correlation, the Fisher exact test and chi-square analysis.
Results
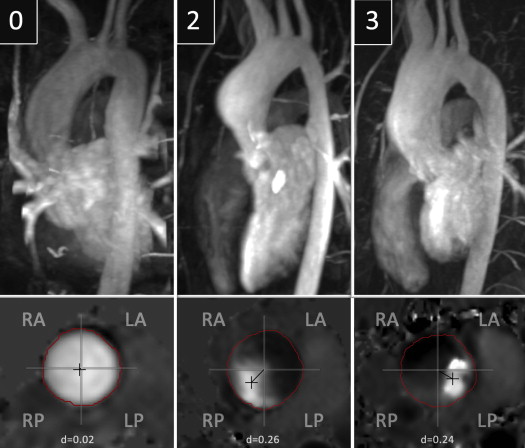
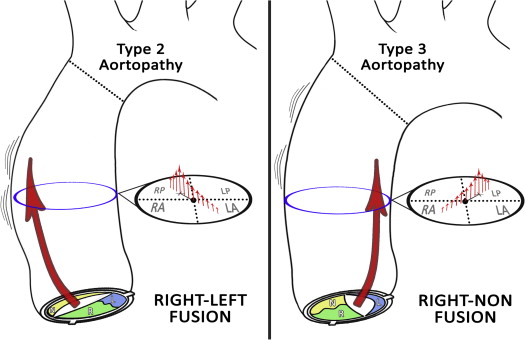
Normal systolic flow was seen in 24% of cases and was significantly correlated with normal aortas ( P = .011). Abnormal flow displacement with RL fusion was strongly associated with rightward deviation (36 of 37 cases), whereas RN fusion skewed leftward (seven of eight cases; P < .01). In patients with aortopathy, RL fusion was strongly associated with type 2 aortopathy and RN with type 3 aortopathy ( P < .01).
Conclusions
Conventional PC MRI can identify abnormal systolic flow and differences in jet orientation with BAV. RL leaflet fusion is associated with rightward flow deviation and type 2 aortopathy, whereas RN fusion is linked to leftward deviation and type 3 aortopathy. The presence and direction of eccentric flow jets may help risk stratify these patients for valve-related aortic disease.
Characterization of eccentric systolic blood flow with bicuspid aortic valve (BAV) has been extensively performed using four-dimensional flow (4D Flow) magnetic resonance imaging (MRI) . Although there is much debate about the significance of these flow patterns, their presence and association with aortic dilation in patients with BAV has been used to support the argument that altered systolic hemodynamics with BAV play a significant role in the aortopathy exhibited by these patients . However, to date, only a few, small cohorts have suggested the prognostic value of MRI flow data in patients with BAV . One reason for this is the relatively slow growth rates of the ascending aorta, typically in the range of ≤1 mm/year . Another reason is the length and complexity of both the 4D Flow acquisition and calculation of flow-related parameters, which have limited its clinical applicability.
Conventional phase-contrast (PC) MRI is often performed in the ascending aortas of patients with BAV to quantify the degree of aortic regurgitation . The calculation is derived from through-plane velocity data for a cross-sectional plane in the tubular ascending aorta, which can be acquired in a single breath-hold. These same data can also be used to assess some of the less-complex findings that have been reported with 4D Flow, such as the presence of eccentric systolic flow and calculation of flow displacement . The aim of this study is to use routine PC data (i.e., two-dimensional [2D] PC MRI) to evaluate the interrelationship between systolic flow, aortopathy, and different aortic leaflets fusion patterns in patients with BAV. We hypothesize that this faster and less technically involved MRI approach to assessing aortic hemodynamics with BAV will reveal important abnormalities of flow that are associated with different types of aortopathy and aortic leaflet fusion patterns.
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
MRI Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Collection and Analysis
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Study Population by Valve Fusion Pattern
Characteristic Right–Left Fusion ( n = 47) Right-Noncoronary Fusion ( n = 12)P Value Age (years), mean ± standard deviation 29.8 ± 12.8 28.1 ± 17.2 .7 Male patients, n (%) 28 (60) 10 (83) .18 Coarctation history, n (%) 24 (51) 3 (25) .11 Aortopathy, n (%) Type 0 20 (43) 4 (33) .56 Type 1 2 (4) 0 .46 Type 2 20 (43) 1 (8) .023 Type 3 5 (10) 7 (58) .0002 Systolic flow, n (%) Normal 10 (22) 4 (33) .38 Rightward 36 (76) 1 (8) <.0001 Leftward 1 (2) 7 (58) <.0001 Aortic stenosis, n (%) ∗ 4 (9) 3 (25) .12 Aortic insufficiency, n (%) ∗ 10 (22) 2 (17) .72
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Aortic Leaflet Fusion Patterns
Get Radiology Tree app to read full this article<
Flow Displacement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Associations by Flow Subgroup
Characteristic Normal Flow ( n = 14) Rightward Flow ( n = 37) Leftward Flow ( n = 8) Age (years) 23.8 ± 12.6 32.2 ± 12.5 26.6 ± 19.0 Flow displacement 0.06 ± 0.02 0.21 ± 0.04 ∗ 0.26 ± 0.09 ∗ Aortic shape Type 0 10 (72) † 11 (30) 3 (37) Type 1 1 (7) 1 (3) 0 Type 2 1 (7) 19 (51) † 1 (13) Type 3 2 (14) 6 (16) 4 (50) ‡ Fusion pattern RL 10 (71) 36 (97) † 1 (13) RN 4 (29) 1 (3) 7 (87) †
The values are presented as mean ± standard deviation or n (%).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hope M.D., Hope T.A., Meadows A.K., et. al.: Bicuspid aortic valve: four-dimensional MR evaluation of ascending aortic systolic flow patterns. Radiology 2010; 255: pp. 53-61.
2. Bissell M.M., Hess A.T., Biasiolli L., et. al.: Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type. Circ Cardiovasc Imaging 2013; 6: pp. 499-507.
3. Mahadevia R., Barker A.J., Schnell S., et. al.: Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy. Circulation 2014; 129: pp. 673-682.
4. Uretsky S., Gillam L.D.: Nature versus nurture in bicuspid aortic valve aortopathy: more evidence that altered hemodynamics may play a role. Circulation 2014; 129: pp. 622-624.
5. Della Corte A., Bancone C., Conti C.A., et. al.: Restricted cusp motion in right-left type of bicuspid aortic valves: a new risk marker for aortopathy. J Thorac Cardiovasc Surg 2012; 144: pp. 360-369.
6. Hope M., Sigovan M., Wrenn J., et. al.: MRI hemodynamic markers of progressive bicuspid aortic valve-related aortic disease. J Magn Reson Imaging 2014; 40: pp. 140-145.
7. Thanassoulis G., Yip J.W., Filion K., et. al.: Retrospective study to identify predictors of the presence and rapid progression of aortic dilatation in patients with bicuspid aortic valves. Nat Clin Pract Cardiovasc Med 2008; 5: pp. 821-828.
8. Muzzarelli S., Monney P., O’Brien K., et. al.: Quantification of aortic flow by phase-contrast magnetic resonance in patients with bicuspid aortic valve. Eur Heart J Cardiovasc Imaging 2014; 15: pp. 77-84.
9. Sigovan M., Hope M.D., Dyverfeldt P., et. al.: Comparison of four-dimensional flow parameters for quantification of flow eccentricity in the ascending aorta. J Magn Reson Imaging 2011; 34: pp. 1226-1230.
10. Hiratzka L.F., Bakris G.L., Beckman J.A., et. al.: 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010; 121: pp. e266-e369.
11. Roman M.J., Devereux R.B., Kramer-Fox R., et. al.: Two-dimensional echocardiographic aortic root dimensions in normal children and adults. Am J Cardiol 1989; 64: pp. 507-512.
12. Della Corte A., Bancone C., Buonocore M., et. al.: Pattern of ascending aortic dimensions predicts the growth rate of the aorta in patients with bicuspid aortic valve. JACC Cardiovasc Imaging 2013; 6: pp. 1301-1310.
13. Kang J.W., Song H.G., Yang D.H., et. al.: Association between bicuspid aortic valve phenotype and patterns of valvular dysfunction and bicuspid aortopathy: comprehensive evaluation using MDCT and echocardiography. JACC Cardiovasc Imaging 2013; 6: pp. 150-161.
14. Ward C.: Clinical significance of the bicuspid aortic valve. Heart 2000; 83: pp. 81-85.
15. Michelena H.I., Khanna A.D., Mahoney D., et. al.: Incidence of aortic complications in patients with bicuspid aortic valves. JAMA 2011; 306: pp. 1104-1112.
16. Siu S.C., Silversides C.K.: Bicuspid aortic valve disease. J Am Coll Cardiol 2010; 55: pp. 2789-2800.
17. Girdauskas E., Borger M.A., Secknus M.A., et. al.: Is aortopathy in bicuspid aortic valve disease a congenital defect or a result of abnormal hemodynamics? A critical reappraisal of a one-sided argument. Eur J Cardiothorac Surg 2011; 39: pp. 809-814.
18. Bauer M., Gliech V., Siniawski H., et. al.: Configuration of the ascending aorta in patients with bicuspid and tricuspid aortic valve disease undergoing aortic valve replacement with or without reduction aortoplasty. J Heart Valve Dis 2006; 15: pp. 594-600.
19. Cotrufo M., Della Corte A.: The association of bicuspid aortic valve disease with asymmetric dilatation of the tubular ascending aorta: identification of a definite syndrome. J Cardiovasc Med (Hagerstown) 2009; 10: pp. 291-297.
20. Schaefer B.M., Lewin M.B., Stout K.K., et. al.: The bicuspid aortic valve: an integrated phenotypic classification of leaflet morphology and aortic root shape. Heart 2008; 94: pp. 1634-1638.
21. Fazel S.S., Mallidi H.R., Lee R.S., et. al.: The aortopathy of bicuspid aortic valve disease has distinctive patterns and usually involves the transverse aortic arch. J Thorac Cardiovasc Surg 2008; 135: pp. 901-907. 907.e1–2
22. Verma S., Siu S.C.: Aortic dilatation in patients with bicuspid aortic valve. N Engl J Med 2014; 370: pp. 1920-1929.
23. Sievers H.H., Schmidtke C.: A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg 2007; 133: pp. 1226-1233.
24. Sabet H.Y., Edwards W.D., Tazelaar H.D., et. al.: Congenitally bicuspid aortic valves: a surgical pathology study of 542 cases (1991 through 1996) and a literature review of 2,715 additional cases. Mayo Clin Proc 1999; 74: pp. 14-26.
25. Burris N.S., Sigovan M., Knauer H.A., et. al.: Systolic flow displacement correlates with future ascending aortic growth in patients with bicuspid aortic valves undergoing magnetic resonance surveillance. Investigative radiology 2014; 49: pp. 635-639.
26. Girdauskas E., Borger M.A.: Bicuspid aortic valve and associated aortopathy: an update. Semin Thorac Cardiovasc Surg 2014; 25: pp. 310-316.