
Rationale and Objectives
The aim of this study was to investigate the experience and desire for training breast imagers in discussing “bad news” with their patients. No such information has been previously reported.
Materials and Methods
Following University of Michigan (UM) institutional review board approval and approval from the Society of Breast Imaging (SBI), questionnaires were mailed to current UM breast imaging faculty members, fellows, and residents and to SBI fellows. The final questionnaire page was mistakenly omitted in the SBI mailing. After institutional review board approval, the final page was sent to the SBI fellows.
Results
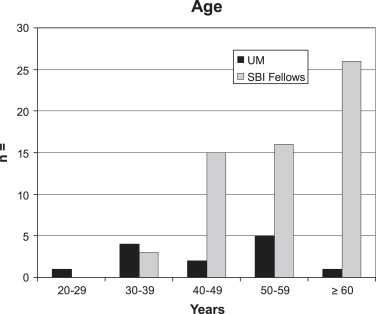
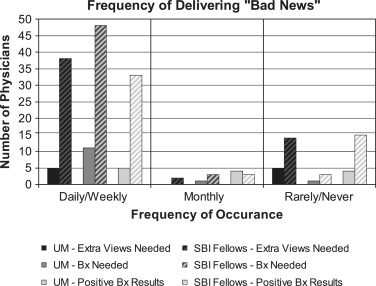
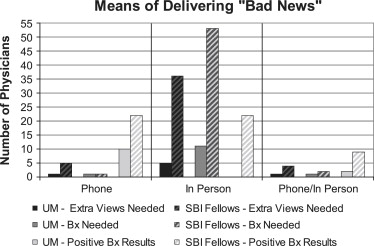
The response rates were 65% (61 of 94) for SBI fellows and 65% (13 of 20) for UM physicians. Ninety-five percent of respondents were aged ≥ 40 years. Sixty-two percent of UM physicians were women, compared to 52% of SBI fellows. Sixty-four percent of respondents practiced in university settings and 34% in private settings. Thirty-five percent of respondents had breast imaging fellowships. The frequency of delivering bad news was most often weekly or daily, whether the news was a need for extra views, a biopsy recommendation, or positive core biopsy results. Recommendations for extra views and breast biopsies were reported to be usually given in person, whereas 59% of respondents delivered positive biopsy results by telephone. Eighty-five percent of respondents noted no previous training in delivering bad news. On a comfort scale ranging from 1 (very uncomfortable) to 10 (very comfortable), 95% of respondents rated their comfort at 8 to 10 for recommending extra views, 85% had the same comfort level for recommending biopsies, and 67% had the same level for giving positive biopsy results. Sixty-two percent of UM radiologists expressed interest in obtaining further training in how to deliver bad news, whereas only 32% of SBI fellows were desirous of such training.
Conclusion
Although radiologists commonly delivered bad news in the breast imaging setting, very few had training in how to do so. Comfort levels declined as the severity of news increased, yet a majority of respondents were not interested in obtaining training in how to deliver bad news. These findings raise the need for further study.
The majority of radiologic examinations occur without patients ever encountering the radiologists who will interpret their examinations. The field of breast imaging is unique in that radiologists frequently interact with their patients. Radiologist–patient interactions can occur during image-guided procedures, breast physical examinations, and breast ultrasound; while telling women the results of their mammographic studies; and/or during discussion of the results of examinations or procedures. Particularly in the latter case, the interaction may include informing a woman that she may have, or likely has, breast cancer.
Discussing “bad news” is known to be a complex and challenging task requiring a combination of compassion and effective communication skills. Both of these, however, receive relatively little attention during physician training, especially in fields such as radiology, which is not a primary care specialty.
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Practice Types and Levels of Training of Respondents
Level_n_ SBI fellows University practice 39 Private practice 21 Both 1 Total 61 UM physicians Faculty members 8 Fellows 2 Residents 3 Total 13
SBI, Society of Breast Imaging; UM, University of Michigan.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
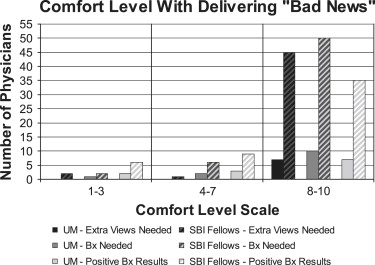
Table 2
Bad News Communication Strategies Listed by Respondents
Be honest and straightforward Use plain English Answer questions Have patience Be optimistic, give hope Sit down Speak slowly Repeat, rephrase Have empathy Listen Follow the patient’s lead Allow time Provide written information Make eye contact Include family and friends Phone the clinician first Show films Provide statistics Always have a plan Ask what the patient knows Have an appointment set with the surgeon Use the word “cancer” Try not to use the word “cancer” Never tell a patient “I think it’s probably cancer” State that “this is unlikely to affect your overall health”
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Ptacek J.T., Eberhardt T.L.: Breaking bad news. JAMA 1996; 276: pp. 496-502.
2. Buckman R.: Breaking bad news: why is it still so difficult?. Br Med J 1984; 288: pp. 1597-1599.
3. Orlander J.D., Fincke B.G., Hermanns D., Johnson G.A.: Medical residents’ first clearly remembered experiences of giving bad news. J Gen Intern Med 2002; 17: pp. 825-840.
4. Baile W.F., Lenzi R., Parker P.A., et. al.: Oncologists’ attitudes toward and practices in giving bad news: an exploratory study. J Clin Oncol 2002; 20: pp. 2189-2196.
5. Stewart M.A.: Effective physician-patient communication and health outcomes: a review. Can Med Assoc J 1995; 152: pp. 1423-1433.
6. Kaplan S.H., Greenfield S., Ware J.E.: Assessing the effects of physician-patient interactions on the outcomes of chronic disease. Med Care 1989; 27: pp. S110-S127.
7. Roberts C.S., Cox C.E., Reintgen D.S., Baile W.F., Gibertini M.: Influence of physician communication on newly diagnosed breast patients’ psychologic adjustment and decision-making. Cancer 1994; 74: pp. 336-341.
8. Beckman H.B., Markakis K.M., Suchman A.L., Frankel R.M.: The doctor-patient relationship and malpractice. Arch Intern Med 1994; 154: pp. 1365-1370.
9. Berlin L.: Communicating findings of radiologic examinations—whither goest the radiologist’s duty?. AJR Am J Roentgenol 2002; 179: pp. 809-815.
10. Hattery R.R.: The president’s message. ABR Examiner 2000; 5: pp. 1-3.
11. Gunderman R.B.: Patient communication. AJR Am J Roentgenol 2001; 177: pp. 41-43.
12. Sickles E.A., Philpotts L.E., Parkinson B.T., et. al.: American College of Radiology/Society of Breast Imaging curriculum for resident and fellow education in breast imaging. J Am Coll Radiol 2006; 3: pp. 279-884.
13. Gurevich M., Devins G.M., Wilson C., McCready D., Marmar C.R., Rodin G.M.: Stress response syndromes in women undergoing mammography: a comparison of women with and without a history of breast cancer. Psychosom Med 2004; 66: pp. 104-112.
14. Liu S., Bassett L.W., Sayre J.: Women’s attitudes about receiving mammographic results directly from radiologists. Radiology 1994; 193: pp. 783-786.
15. Levin K.S., Braeuning P., O’Malley M.S., Pisano E.D., Barrett E.D., Earp J.A.L.: Communicating results of diagnostic mammography: what do the patients think?. Acad Radiol 2000; 7: pp. 1069-1076.
16. Levitsky D.B., Frank M.S., Richardson M.L., Shneidman R.J.: How should radiologists reply when patients ask about their diagnosis?. AJR Am J Roentgenol 1993; 161: pp. 433-436.
17. Lind S.E., Kopans D., Delvecchio Good M.: Patients’ preferences for learning the results of mammographic examinations. Breast Cancer Res Treat 1992; 23: pp. 223-232.
18. Vallely S.R., Manton Mills J.O.: Should radiologists talk to patients?. Br Med J 1990; 300: pp. 305-306.
19. Schreiber M.H., Leonard M., Youmans Rieniets C.: Disclosure of imaging findings to patients directly by radiologists: survey of patients’ preferences. AJR Am J Roentgenol 1995; 165: pp. 467-469.
20. Hoffman N.Y., Janus J., Destounis S., Logan-Young W.: When the patient asks for the results of her mammogram, how should the radiologist reply?. AJR Am J Roentgenol 1994; 162: pp. 597-599.
21. Baile W.F., Kudelka A.P., Beale E.A., et. al.: Communication skills training in oncology: Description and preliminary outcomes of workshops on breaking bad news and managing patient reactions to illness. Cancer 1999; 86: pp. 887-897.
22. Baile W.F., Buckman R., Lenzi R., Glober G., Beale E.A., Kudelka A.P.: SPIKES—a six-step protocol for delivering bad news: application to the patient with cancer. Oncologist 2000; 5: pp. 302-311.
23. Fallowfield L., Jenkins V., Farewell V., Solis-Trapola I.: Enduring impact of communication skills training: results of a 12-month follow-up. Br J Cancer 2003; 89: pp. 1445-1449.
24. Jenkins V., Fallowfield L.: Can communication skills training alter physicians’ beliefs and behaviors in clinics?. J Clin Oncol 2002; 20: pp. 765-769.
25. Vaidya V.U., Greenberg L.W., Patel K.M., Strauss L.H., Pollack M.M.: Teaching physicians how to break bad news. Arch Pediatr Adolesc Med 1999; 153: pp. 419-422.
26. Vandekieft G.K.: Breaking bad news. Am Fam Physician 2001; 64: pp. 1975-1978.
27. Sutton S., Saidi G., Bickler G., Hunter J.: Does routine screening for breast cancer raise anxiety?. J Epidemiol Commun Health 1995; 49: pp. 413-418.
28. Smith R.L., Crawford B.J., Petersen L.R., Johnson R.E., Hartmann L.C.: Breaking bad news: current trends in disclosure of cancer diagnosis as related by women with newly diagnosed breast cancer. Psycho-Oncol 2006; 15: pp. S60.
29. Eggly S., Penner L., Albrecht T.L., et. al.: Discussing bad news in the outpatient oncology clinic: rethinking current communication guidelines. J Clin Oncol 2006; 24: pp. 716-719.