
Rationale and Objectives
Breast magnetic resonance imaging (MRI) is recommended for the screening of women with a history of chest radiotherapy and consequent increased breast cancer risk. The purpose of this study was to evaluate the impact of prior chest radiotherapy on breast tissue background parenchymal enhancement (BPE) at screening breast MRI.
Materials and Methods
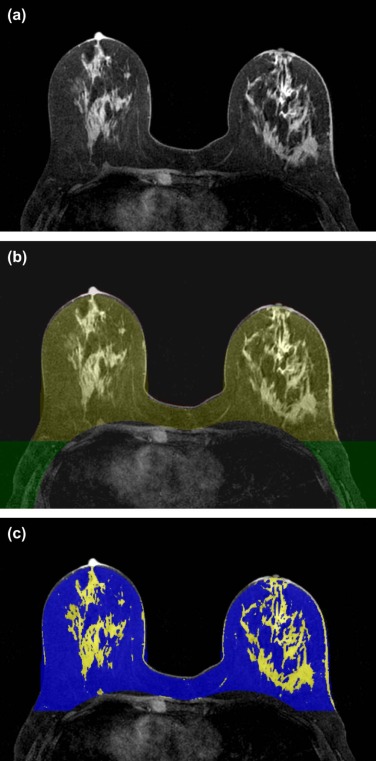
A departmental database was reviewed to identify asymptomatic women with either a history of chest radiotherapy for Hodgkin’s lymphoma or age-matched controls who underwent screening breast MRI between 2009 and 2013. MRI studies were analyzed on an automated breast MRI viewing platform to calculate breast BPE and breast density.
Results
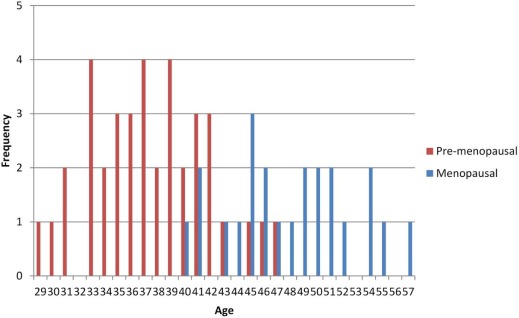
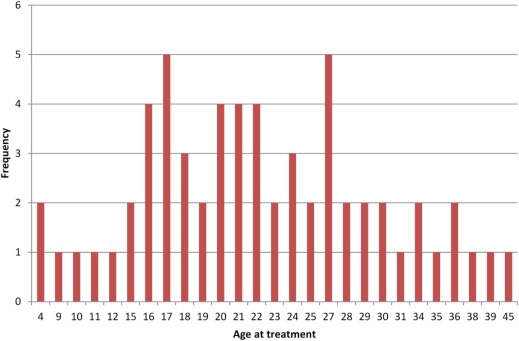
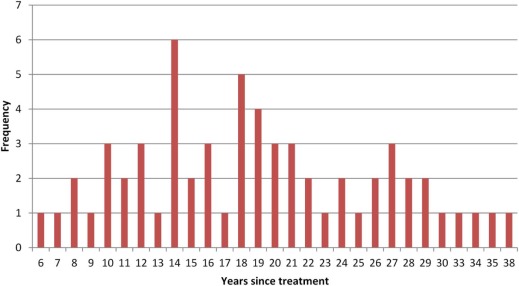
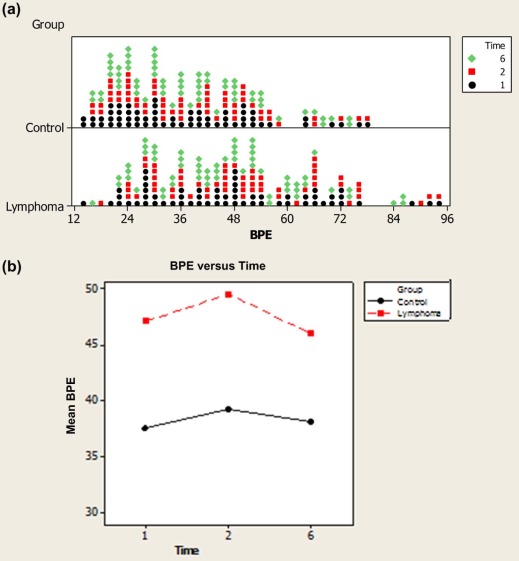
A total of 61 cases (mean age 41.6 ± 6.75 years) and 61 controls (mean age 40.8 ± 6.99 years) were included. The age of patients at the time of chest radiotherapy was 22.6 ± 8.17 years. Screening MRI was performed 19.0 ± 7.43 years after chest radiotherapy. BPE was significantly higher in patients who received chest radiotherapy (50% vs. 37%, P < 0.01). A weak to moderate positive correlation (r > 0.3; P < 0.03) was found between BPE and number of years post radiotherapy. There was a trend toward significant difference between the two groups in the correlation of BPE and age ( P = 0.05). Breast density was not significantly different between the two groups.
Conclusions
BPE is significantly greater in women who receive chest radiotherapy for childhood Hodgkin’s lymphoma, and unexpectedly, it positively correlates with the number of years passed after radiation therapy. Long-term biological effects of radiation therapy on breast parenchyma need further research.
Introduction
It is well established that women treated with chest radiotherapy for Hodgkin’s lymphoma (HL) at a young age are at significantly increased risk of developing breast cancer after a latency period . In a recent large multicenter study, Moskowitz et al. reported a 35% cumulative incidence of breast cancer among HL survivors by 50 years of age; this is higher than the cumulative risk of breast cancer among BRCA1 or BRCA2 mutation carriers by age 50 years .
Numerous studies have shown that breast magnetic resonance imaging (MRI) is significantly more sensitive than mammography for breast cancer detection in women with a genetic or familial predisposition to breast cancer . In women with a history of chest radiotherapy for HL, breast MRI adjunctive to annual mammographic screening was recommended largely based on expert opinion and was recently supported by results from a few single-center studies . Despite a very high sensitivity, screening breast MRI is tempered by imperfect specificity because of overlap in the appearances of benign and malignant lesions. Identification of factors associated with low specificity may improve the accuracy and cost efficiency of breast MRI and allow for wider implementation of screening MRI.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Patient and Control Selection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Indications for MRI Screening in the Control Group
Indication Number of Cases Mean Age, Years BRCA 1 carriers 10 37.7 BRCA 2 carrier 3 38.9 First-degree relative BRCA carrier 5 34.1 Lifetime risk from 25% to 30% \* 32 40.9 Lifetime risk >30% \* 10 46.3 Cowden syndrome 1 46
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Techniques
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Comparison of background parenchymal enhancement (%) Between Cases and Controls
Descriptive Statistics Independent Samples t Test_N_ Mean Std. Dev_t_ Statistic_P_ Value 1 minute POST Lymphoma 59 47.5 18.9 3.286 0.0013 Control 60 36.9 16.3 2 minutes POST Lymphoma 57 50.0 18.4 3.618 0.00045 Control 58 38.5 15.6 6 minutes POST Lymphoma 59 46.4 16.7 2.797 0.0060 Control 61 38.1 15.9
POST, postcontrast administration; Std. dev, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Pearson Correlation ( P Value) Between Years Since Treatment and background parenchymal enhancement
BPE 1 min BPE 2 min BPE 6 min All patients ( n = 61) 0.311
(0.016) 0.392
(0.003) 0.294
(0.024)
BPE, background parenchymal enhancement; 1 min, 1 minute post contrast; 2 min, 2 minutes post contrast; 6 min, 6 minutes post contrast.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Pearson Correlation Between Age and background parenchymal enhancement ( P Value)
BPE 1 min BPE 2 min BPE 6 min Lymphoma ( n = 61) 0.185
(0.160) 0.163
(0.227) 0.157
(0.236) Control ( n = 61) −0.114
(0.385) −0.088
(0.513) −0.065
(0.619)
BPE, background parenchymal enhancement; 1 min, 1 minute post contrast; 2 min, 2 minutes post contrast; 6 min, 6 minutes post contrast.
TABLE 5
Fisher r-to-z Transformation Test to Assess the Difference in Correlations Between Breast background parenchymal enhancement and Age in Cases and Controls at Different Time Points
BPE 1 min BPE 2 min BPE 6 min_P_ value 0.05 0.0934 0.117
BPE, background parenchymal enhancement; 1 min, 1 minute post contrast; 2 min, 2 minutes post contrast; 6 min, 6 minutes post contrast.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Travis L.B., Hill D., Dores G.M., et. al.: Cumulative absolute breast cancer risk for young women treated for Hodgkin lymphoma. J Natl Cancer Inst 2005; 97: pp. 1428-1437.
2. Moskowitz C.S., Chou J.F., Wolden S.L., et. al.: Breast cancer after chest radiation therapy for childhood cancer. J Clin Oncol 2014; 32: pp. 2217-2223.
3. Kriege M., Brekelmans C.T.M., Boetes C., et. al.: Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med 2004; 351: pp. 427-437.
4. Warner E., Plewes D.B., Hill K.A., et. al.: Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004; 292: pp. 1317-1325.
5. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
6. Saslow D., Boetes C., Burke W., et. al.: American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin 2007; 57: pp. 75-89.
7. Lee C.H., Dershaw D.D., Kopans D., et. al.: Breast cancer screening with imaging: recommendations from the Society of Breast Imaging and the ACR on the use of mammography, breast MRI, breast ultrasound, and other technologies for the detection of clinically occult breast cancer. J Am Coll Radiol 2010; 7: pp. 18-27.
8. Sung J.S., Lee C.H., Morris E.A., et. al.: Screening breast MR imaging in women with a history of chest irradiation. Radiology 2011; 259: pp. 65-71.
9. Ng A.K., Garber J.E., Diller L.R., et. al.: Prospective study of the efficacy of breast magnetic resonance imaging and mammographic screening in survivors of Hodgkin lymphoma. J Clin Oncol 2013; 31: pp. 2282-2288.
10. Freitas V., Scaranelo A., Menezes R., et. al.: Added cancer yield of breast magnetic resonance imaging screening in women with a prior history of chest radiation therapy. Cancer 2013; 119: pp. 495-503.
11. Kuhl C.K., Bieling H.B., Gieseke J., et. al.: Healthy premenopausal breast parenchyma in dynamic contrast-enhanced MR imaging of the breast: normal contrast medium enhancement and cyclical-phase dependency. Radiology 1997; 203: pp. 137-144.
12. Teifke A., Hlawatsch A., Beier T., et. al.: Undetected malignancies of the breast: dynamic contrast-enhanced MR imaging at 1.0 T. Radiology 2002; 224: pp. 881-888.
13. Shimauchi A., Jansen S.A., Abe H., et. al.: Breast cancers not detected at MRI: review of false-negative lesions. AJR Am J Roentgenol 2010; 194: pp. 1674-1679.
14. Uematsu T., Kasami M., Watanabe J.: Does the degree of background enhancement in breast MRI affect the detection and staging of breast cancer?. Eur Radiol 2011; 21: pp. 2261-2267.
15. Hambly N.M., Liberman L., Dershaw D.D., et. al.: Background parenchymal enhancement on baseline screening breast MRI: impact on biopsy rate and short-interval follow-up. AJR Am J Roentgenol 2011; 196: pp. 218-224.
16. KIng V., Brooks J.D., Bernstein J.L., et. al.: Background parenchymal enhancement at breast MR imaging and breast cancer risk. Radiology 2011; 260: pp. 50-60.
17. Dontchos B.N., Rahbar H., Patridge S.C., et. al.: Are quantitative assessments of background parenchymal enhancement, amount of fibroglandular tissue on MR images, and mammography density associated with breast cancer risk?. Radiology 2015; 276: pp. 371-380.
18. Li J., Dershaw D.D., Lee C.H., et. al.: Breast MRI after conservation therapy: usual findings in routine follow-up examinations. AJR Am J Roentgenol 2010; 195: pp. 799-807.
19. Kim Y.J., Kim S.H., Choi B.G., et. al.: Impact of radiotherapy on background parenchymal enhancement in breast magnetic resonance imaging. Asian Pac J Cancer Prev 2014; 15: pp. 2939-2943.
20. Mousa N.A., Eiada R., Crystal P., et. al.: The effect of acute aromatase inhibition on breast parenchymal enhancement in magnetic resonance imaging: a prospective pilot clinical trial. Menopause 2012; 19: pp. 420-425.
21. Giess C.S., Yeh E.D., Raza S., et. al.: Background parenchymal enhancement at breast MR imaging: normal patterns, diagnostic challenges, and potential for false-positive and false-negative interpretation. Radiographics 2014; 34: pp. 234-247.
22. Ahmed M.N., Yamany S.M., Mohamed N., et. al.: A modified fuzzy C-means algorithm for bias field estimation and segmentation of MRI data. IEEE Trans Med Imaging 2002; 21: pp. 193-199.
23. Klifa S., Carballido-Gamio G., Wilmes L., et. al.: Quantification of breast tissue index from MR data using fuzzy clustering. Conf Proc IEEE Eng Med Biol Soc 2004; 3: pp. 1667-1670.
24. Uematsu T., Kasami M., Watanabe J.: Should breast MRI be performed with adjustment for the phase in patients’ menstrual cycle? Correlation between mammographic density, age, and background enhancement on breast MRI without adjusting for the phase in patients’ menstrual cycle. Eur J Radiol 2012; 81: pp. 1539-1542.
25. Melsaether A., McDermott M., Gupta D., et. al.: Inter- and intrareader agreement for categorization of background parenchymal enhancement at baseline and after training. AJR Am J Roentgenol 2014; 203: pp. 209-215.
26. Grimm L.J., Anderson A.L., Baker J.A., et. al.: Interobserver variability between breast imagers using the fifth edition of the BI-RADS MRI Lexicon. AJR Am J Roentgenol 2015; 204: pp. 1120-1124.
27. Klifa C., Suzuki S., Aliu S., et. al.: Quantification of background enhancement in breast magnetic resonance imaging. J Magn Reson Imaging 2011; 33: pp. 1229-1234.
28. Boyd N.F., Guo H., Martin L.J., et. al.: Mammographic density and the risk and detection of breast cancer. N Engl J Med 2007; 356: pp. 227-236.
29. Passaperuma K., Warner E., Hill K.A., et. al.: Is mammographic breast density a breast cancer risk factor in women with BRCA mutations?. J Clin Oncol 2010; 28: pp. 3779-3783.
30. Jansen S.A., Shimauchi A., Zak L., et. al.: Kinetic curves of malignant lesions are not consistent across MRI systems: need for improved standardization of breast dynamic contrast-enhanced MRI acquisition. AJR Am J Roentgenol 2009; 193: pp. 832-839.