
Rationale and Objectives
We aimed to investigate the utility of problem-solving breast magnetic resonance imaging (MRI) for mammographic Breast Imaging Reporting and Data System (BI-RADS) categories 3 and 4 microcalcifications.
Materials and Methods
Between January 1, 2010 and December 31, 2011, 138 women with 146 areas of categories 3 and 4 microcalcifications without sonographic correlates underwent breast MRI and had a stereotactic core biopsy using an 11-gauge needle or follow-up at least for 24 months. Positive predictive value (PPV), negative predictive value, sensitivity, and specificity were calculated on the basis of BI-RADS category, with categories 1–3 being considered benign and categories 4 and 5 being considered malignant.
Results
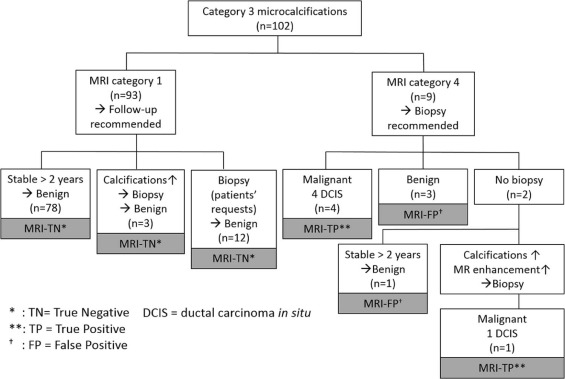
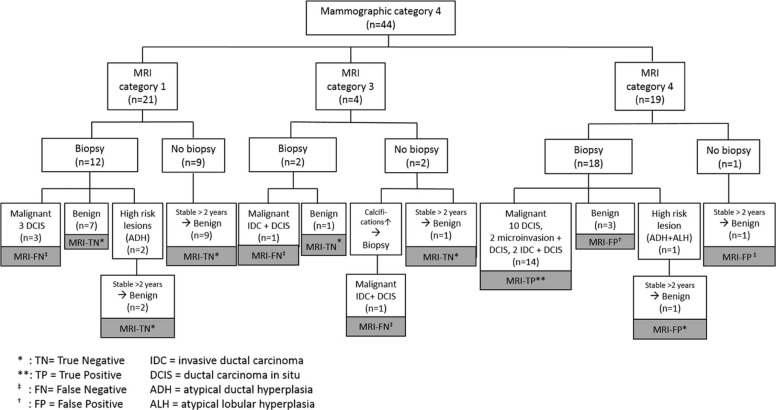
Twenty-four cases (16.4%) were malignant (18 ductal carcinoma in situ, 6 invasive). MRI increased PPV and specificity from 43% to 68% and from 80% to 93% ( P = .054 and .005) compared to mammography. Within 102 category 3 microcalcifications, 5 carcinomas were assessed correctly as category 4 by MRI. Within 44 category 4 microcalcifications, a correct diagnosis was made by MRI in 77% (34 of 44) as opposed to 43% (19 of 44) by mammography, and 80% (20 of 25) of unnecessary biopsies could have been avoided. Within the 24 carcinomas, 5 were negative at MRI. MRI-negative carcinomas have a significantly higher possibility of being low grade (ductal carcinoma in situ or invasive) ( P = .0362).
Conclusions
Breast MRI has the potential to improve the diagnosis of category 3 or 4 microcalcifications and could alter indications for biopsy. Breast MRI could help predict the presence or absence of higher-grade carcinoma for category 3 or 4 microcalcifications.
Introduction
Breast magnetic resonance imaging (MRI) has been widely used for patients with newly diagnosed breast carcinoma and for high-risk screening . However, there is no clear consensus on the use of MRI for “problem-solving” purposes in cases of inconclusive mammographic or ultrasound findings. Because positive predictive values (PPVs) of screening mammography and ultrasound have been reported to be only 18.4%–31.0% and 6.7%–13.2% , respectively, it would be desirable to reduce the number of biopsies that yield benign results. Although the performance of problem-solving breast MRI has been reported to be excellent for noncalcified lesions , reported results of those for microcalcifications are inconsistent , and only few studies used a large dataset including Breast Imaging Reporting and Data System (BI-RADS) categories 3 and 4 microcalcifications.
Previous studies evaluating the role of MRI in the diagnosis of microcalcifications suggested that false-negative carcinomas at MRI are low- or intermediate-grade ductal carcinoma in situ (DCIS) , although the characteristics of such cases were not further investigated in these studies. The results suggest that low-grade carcinomas negative at MRI might be biologically unimportant , and MRI could be used for microcalcifications at least to detect high-grade carcinomas.
Get Radiology Tree app to read full this article<
Materials and Methods
Inclusion Criteria
Get Radiology Tree app to read full this article<
Imaging Technique and Interpretation
Mammography Protocol and Interpretation
Get Radiology Tree app to read full this article<
Breast MRI Protocol and Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Management
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Patient Cohort
Get Radiology Tree app to read full this article<
Table 1
Demographic Data ( n = 138)
Age (y) Mean 51.7 Median 51 Range 33–74 Menopausal status Premenopausal 53 (38) Postmenopausal 72 (52) Irregular 6 (4) Unknown 7 (5) Indication for mammography Screening 109 (79) Diagnostic 29 (21) Follow-up after benign biopsy 9 Follow-up for a US lesion 5 Follow-up for calcifications 3 Follow-up after breast cancer 3 Other reasons (breast pain, palpable lesion) 9 Family history of breast cancer Yes (not first degree relative) 9 (7) Yes (first degree relative) 6 (4) No 123 (89) Personal history of breast cancer Yes 3 (2) No 135 (98) History of high-risk lesion Yes 4 (3) No 134 (97) Breast density Entirely fatty 6 (4) Scattered areas of fibroglandular density 50 (36) Heterogeneously dense 66 (48) Extremely dense 16 (11)
US, ultrasound.
Data are numbers of patients except for age. Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Final Diagnoses of Microcalcifications and Incidental MRI Findings
No. of Lesions No. of Incidental MRI Lesions Total Histologic type of breast cancers Total no. of cancers 24 1 25 DCIS 18 (75) 1 (100) 19 (76) DCIS with microinvasion 2 (8) 0 2 (8) IDC + DCIS 4 (17) 0 4 (16) Breast cancer stage pTis 19 (79) 1 (100) 20 (80) pT1a 2 (8) 2 (8) pT1b 0 0 pT1c 3 (13) 3 (12) Nuclear grade of DCIS Low-grade 1 (6) 1 (100) 2 (11) Intermediate-grade 11 (61) 0 11 (58) High-grade 6 (33) 0 6 (31) Nuclear grade of invasive breast cancers Grade 1 2 (33) 1 (100) 3 (43) Grade 2 4 (67) 0 4 (57) Grade 3 0 0 0 High-risk lesions Total no. of high-risk lesions 3 0 3 ADH 2 (67) 0 2 (67) ADH and ALH 1 (33) 0 1 (33) Benign diagnoses Total diagnosis of benign findings 119 8 127 Benign diagnosis confirmed by biopsy 29 (24) 2 (25) 30 (24) Fibrocystic changes 24 (20) 0 24 (19) Fibroadenoma 1 (1) 0 1 (1) Intraductal papilloma without atypia 0 1 (13) 1 (1) Nonspecific benign findings 4 (3) 1 (13) 5 (4) Benign diagnosis confirmed by follow-up 90 (76) 6 (75) 96 (76)
ADH, atypical ductal hyperplasia; ALH, atypical lobular hyperplasia; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; MRI, magnetic resonance imaging.
Data are numbers of lesions. Numbers in parentheses are percentages.
Get Radiology Tree app to read full this article<
Overall Performances of Mammography Only and Mammography Plus MRI
Get Radiology Tree app to read full this article<
Table 3
Overall Performances of Mammography and MRI
Parameter Mammography Mammography + MRI_P_ Value True-positive 19 19 NA True-negative 97 113 False-positive 25 9 False-negative 5 5 Sensitivity 79.2% (22/27) 79.2% (22/27) NS Specificity 79.5% (97/122) 92.6% (113/122) .005 PPV 43.2% (22/47) 67.9% (22/31) .054 NPV 95.1% (97/102) 95.8% (113/118) NS
MRI, magnetic resonance imaging; NA, not available; NPV, negative predictive value; NS, not significant; PPV, positive predictive value.
Data are numbers of lesions for test characteristics, and percentages for sensitivity, specificity, PPV, and NPV.
Get Radiology Tree app to read full this article<
Frequency of Malignancy According to Mammography Findings
Get Radiology Tree app to read full this article<
Mammographic Category 3 Microcalcifications
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Mammographic Category 4 Microcalcifications
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
False-Negative Malignancy at Mammography and MRI
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 4
Nuclear Grades of Carcinomas ( n = 24)
Modality Test Characteristics Low Grade or Grade 1 Higher Grade_P_ Value MRI True-positive 0 19 .0362 False-negative 2 3 Mammography True-positive 3 16 1 False-negative 0 5
MRI, magnetic resonance imaging.
Get Radiology Tree app to read full this article<
Incidental Lesions Found at MRI
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix S1
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Kuhl C.K., Schrading S., Leutner C.C., et. al.: Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol 2005; 23: pp. 8469-8476.
2. Halladay J.R., Yankaskas B.C., Bowling J.M., et. al.: Positive predictive value of mammography: comparison of interpretations of screening and diagnostic images by the same radiologist and by different radiologists. AJR Am J Roentgenol 2010; 195: pp. 782-785.
3. van Luijt P.A., Fracheboud J., Heijnsdijk E.A., et. al.: Nation-wide data on screening performance during the transition to digital mammography: observations in 6 million screens. Eur J Cancer 2013; 49: pp. 3517-3525.
4. Lehman C.D., Lee C.I., Loving V.A., et. al.: Accuracy and value of breast ultrasound for primary imaging evaluation of symptomatic women 30–39 years of age. AJR Am J Roentgenol 2012; 199: pp. 1169-1177.
5. Weigert J., Steenbergen S.: The Connecticut Experiment: the role of ultrasound in the screening of women with dense breasts. Breast J 2012; 18: pp. 517-522.
6. Pediconi F., Catalano C., Roselli A., et. al.: The challenge of imaging dense breast parenchyma: is magnetic resonance mammography the technique of choice? A comparative study with x-ray mammography and whole-breast ultrasound. Invest Radiol 2009; 44: pp. 412-421.
7. El-Barhoun E.N., Pitman A.G.: Impact of breast MR in non-screening Australian clinical practice: audit data from a single-reader single-centre site. J Med Imaging Radiat Oncol 2011; 55: pp. 461-473.
8. Bick U., Engelken F., Diederichs G., et. al.: MRI of the breast as part of the assessment in population-based mammography screening. Rofo 2013; 185: pp. 849-856.
9. Benndorf M., Baltzer P.A., Vag T., et. al.: Breast MRI as an adjunct to mammography: does it really suffer from low specificity? A retrospective analysis stratified by mammographic BI-RADS classes. Acta Radiol 2010; 51: pp. 715-721.
10. Bennani-Baiti B., Bennani-Baiti N., Baltzer P.A.: Diagnostic performance of breast magnetic resonance imaging in non-calcified equivocal breast findings: results from a systematic review and meta-analysis. PLoS ONE 2016; 11: e0160346
11. Zhu J., Kurihara Y., Kanemaki Y., et. al.: Diagnostic accuracy of high-resolution MRI using a microscopy coil for patients with presumed DCIS following mammography screening. J Magn Reson Imaging 2007; 25: pp. 96-103.
12. Strobel K., Schrading S., Hansen N.L., et. al.: Assessment of BI-RADS category 4 lesions detected with screening mammography and screening US: utility of MR imaging. Radiology 2015; 274: pp. 343-351.
13. Stehouwer B.L., Merckel L.G., Verkooijen H.M., et. al.: 3-T breast magnetic resonance imaging in patients with suspicious microcalcifications on mammography. Eur Radiol 2014; 24: pp. 603-609.
14. Li E., Li J., Song Y., et. al.: A comparative study of the diagnostic value of contrast-enhanced breast MR imaging and mammography on patients with BI-RADS 3–5 microcalcifications. PLoS ONE 2014; 9: e111217
15. Kneeshaw P.J., Lowry M., Manton D., et. al.: Differentiation of benign from malignant breast disease associated with screening detected microcalcifications using dynamic contrast enhanced magnetic resonance imaging. Breast 2006; 15: pp. 29-38.
16. Jiang Y., Lou J., Wang S., et. al.: Evaluation of the role of dynamic contrast-enhanced MR imaging for patients with BI-RADS 3–4 microcalcifications. PLoS ONE 2014; 9: e99669
17. Fiaschetti V., Pistolese C.A., Perretta T., et. al.: 3–5 BI-RADS microcalcifications: correlation between MRI and histological findings. ISRN Oncol 2011; 2011: pp. 643890.
18. Brnic D., Brnic D., Simundic I., et. al.: MRI and comparison mammography: a worthy diagnostic alliance for breast microcalcifications?. Acta Radiol 2016; 57: pp. 413-421.
19. Bluemke D.A., Gatsonis C.A., Chen M.H., et. al.: Magnetic resonance imaging of the breast prior to biopsy. JAMA 2004; 292: pp. 2735-2742.
20. Uematsu T., Yuen S., Kasami M., et. al.: Dynamic contrast-enhanced MR imaging in screening detected microcalcification lesions of the breast: is there any value?. Breast Cancer Res Treat 2007; 103: pp. 269-281.
21. Kikuchi M., Tanino H., Kosaka Y., et. al.: Usefulness of MRI of microcalcification lesions to determine the indication for stereotactic mammotome biopsy. Anticancer Res 2014; 34: pp. 6749-6753.
22. Houserkova D., Prasad S.N., Svach I., et. al.: The value of dynamic contrast enhanced breast MRI in mammographically detected BI-RADS 5 microcalcifications. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2008; 152: pp. 107-115.
23. Akita A., Tanimoto A., Jinno H., et. al.: The clinical value of bilateral breast MR imaging: is it worth performing on patients showing suspicious microcalcifications on mammography?. Eur Radiol 2009; 19: pp. 2089-2096.
24. Bazzocchi M., Zuiani C., Panizza P., et. al.: Contrast-enhanced breast MRI in patients with suspicious microcalcifications on mammography: results of a multicenter trial. AJR Am J Roentgenol 2006; 186: pp. 1723-1732.
25. Sanders M.E., Schuyler P.A., Dupont W.D., et. al.: The natural history of low-grade ductal carcinoma in situ of the breast in women treated by biopsy only revealed over 30 years of long-term follow-up. Cancer 2005; 103: pp. 2481-2484.
26. Sagara Y., Mallory M.A., Wong S., et. al.: Survival benefit of breast surgery for low-grade ductal carcinoma in situ: a population-based cohort study. JAMA Surg 2015; 150: pp. 739-745.
27. Morimoto T., Okazaki M., Endo T.: Current status and goals of mammographic screening for breast cancer in Japan. Breast Cancer 2004; 11: pp. 73-81.
28. Tozaki M., Fukuda K.: High-spatial-resolution MRI of non-masslike breast lesions: interpretation model based on BI-RADS MRI descriptors. AJR Am J Roentgenol 2006; 187: pp. 330-337.
29. Tozaki M., Igarashi T., Fukuda K.: Positive and negative predictive values of BI-RADS-MRI descriptors for focal breast masses. Magn Reson Med Sci 2006; 5: pp. 7-15.
30. Tozaki M., Fukuma E.: 1H MR spectroscopy and diffusion-weighted imaging of the breast: are they useful tools for characterizing breast lesions before biopsy?. AJR Am J Roentgenol 2009; 193: pp. 840-849.
31. Uematsu T., Kasami M., Watanabe J.: Does the degree of background enhancement in breast MRI affect the detection and staging of breast cancer?. Eur Radiol 2011; 21: pp. 2261-2267.
32. Bennani-Baiti B., Baltzer P.A.: MR imaging for diagnosis of malignancy in mammographic microcalcifications: a systematic review and meta-analysis. Radiology 2017; 283: pp. 692-701.
33. Kuhl C.K., Schrading S., Bieling H.B., et. al.: MRI for diagnosis of pure ductal carcinoma in situ: a prospective observational study. Lancet 2007; 370: pp. 485-492.
34. Sanders M.E., Schuyler P.A., Simpson J.F., et. al.: Continued observation of the natural history of low-grade ductal carcinoma in situ reaffirms proclivity for local recurrence even after more than 30 years of follow-up. Mod Pathol 2015; 28: pp. 662-669.
35. International Federation of Health Plans : Variation in medical and hospital prices by country. Comparative price report; Available at: https://static1.squarespace.com/static/518a3cfee4b0a77d03a62c98/t/57d3ca9529687f1a257e9e26/1473497751062/2015+Comparative+Price+Report+09.09.16.pdf