
Purpose
To determine whether coronary artery anomalies can be detected on noncontrast computed tomography (CT) coronary artery calcium scoring (CCS) studies.
Materials and Methods
A total of 126 patients (mean age 62 years; 35 women) underwent noncontrast CCS and contrast enhanced coronary CT angiography (cCTA). Thirty-three patients were diagnosed with a coronary anomaly on cCTA, whereas coronary anomalies were excluded in 93. Two observers (reader 1 [R1] and reader 2 [R2]), blinded to patient information independently evaluated each CCS study for: 1) visibility of coronary artery origins, 2) detection of coronary anomalies, and 3) benign or malignant (ie, interarterial) course. Using cCTA as the reference standard, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of CCS studies for detecting coronary anomalies were calculated.
Results
Of the 33 coronary anomalies, 16 were benign and 17 malignant. Based on noncontrast CCS studies, R1 and R2 correctly identified the left main origin in 123/126 (97.6%) and 121/126 (96%) patients; the left anterior descending origin in 125/126 (99.2%) and 122/126 (96.8%); the circumflex origin in 120/126 (95.2%) and 105/126 (83.3%); and the right coronary artery origin in 117/126 (92.9%) and 103/126 (81.7%), respectively. R1 and R2 identified 34 and 27 coronary anomalies and classified 19 and 15 as malignant, respectively. Interobserver reproducibility for detection of coronary anomalies was good (k = 0.76). Interobserver agreement for detection of malignant variants was even stronger (k = 0.80). On average, coronary artery anomalies were diagnosed with 85.2% sensitivity, 96.4% specificity, 90.5% PPV, and 94.1% NPV on noncontrast CCS studies.
Conclusion
Benign and malignant coronary artery anomalies can be detected with relatively high accuracy on noncontrast-enhanced CCS studies. CCS studies should be reviewed for signs of coronary artery anomalies in order to identify malignant variants with possible impact on patient management.
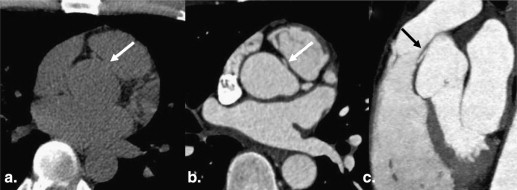
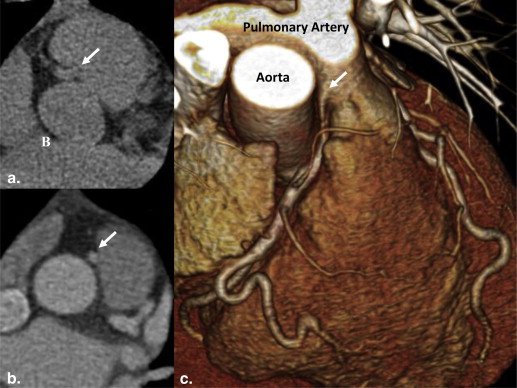
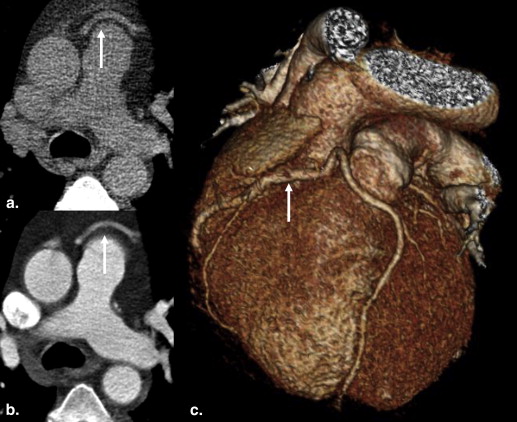
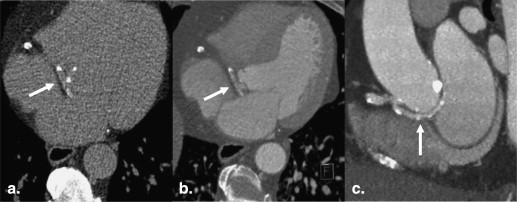
The anatomy of the coronary arteries is not always predictable. Normal coronary anatomy is defined by a left coronary artery (LCA) and a right coronary artery (RCA) originating from the left and right aortic sinus, respectively. Coronary artery anomalies are variants rarely observed in the common population. Some are classified as benign while others—malignant types—can be life-threatening. Anomalies of the coronary arteries can be defined by their origin, course, or termination . Other variants such as anomalies of intrinsic coronary arterial anatomy (eg, congenital ostial stenosis, coronary aneurysms) were not subject of this study. Prognostically important variants, sometimes referred to as “malignant” anomalies, take an interarterial proximal course between the main pulmonary artery and the aorta. This path is subject to compression—especially during exercise—whereas “benign” coronary artery anomalies (non-interarterial, eg, retro-aortic course) do not carry such risk . Specific examples of interarterial coronary anomalies include an anomalous origin of the LCA from the RCA or right coronary sinus, or the anomalous origin of the RCA from the LCA or left coronary sinus. A common example of an anomaly not associated with possible myocardial ischemia is the circumflex artery (Cx) originating from the right coronary sinus without interarterial course.
Malignant coronary artery anomalies have been linked with chest pain, sudden death, cardiomyopathy, syncope, dyspnea, arrhythmia, ventricular fibrillation, and myocardial infarction . The prevalence of these anomalies in society is estimated to be at or less than 1% but that number may be misleading because of the number of asymptomatic patients that go undiagnosed . Some studies suggest that sudden cardiac death is caused by malignant coronary artery anomalies in upwards of 12% of cases .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Review
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
cCTA
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CCS Studies
Get Radiology Tree app to read full this article<
Table 1
Diagnostic Performance of CCS for Detecting Coronary Anomalies
Sensitivity (%) Specificity (%) PPV (%) NPV (%) R1 91.7 95.9 89.2 96.9 R2 78.6 96.9 91.7 91.2 Average 85.2 96.4 90.5 94.1
CCS, coronary calcium scoring; NPV, negative predictive value; PPV, positive predictive value; R1, reader 1; R2, reader 2.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Number of Patients with Detectable Coronary Artery Origin at CCS
LM LAD Cx RCA Yes No % Yes No % Yes No % Yes No % R1 123 3 (97.6) 125 1 (99.2) 120 6 (95.2) 117 9 (92.9) R2 121 5 (96.0) 122 4 (96.8) 105 21 (83.3) 103 23 (81.7)
CCS, coronary calcium scoring; Cx, left circumflex coronary artery; LAD, left anterior descending coronary artery; LM, left main coronary artery; R1, reader 1; R2, reader 2; RCA, right coronary artery.
Percentage of correct identification in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Inter-observer Agreement of Overall Coronary Anomalies and Malignant Anomalies (n = 126)
Coronary Anomalies Malignant Yes No Yes No R1 34 92 19 15 R2 27 99 15 12 Interobserver agreement (Κ) 0.76 0.80
R1, reader 1; R2, reader 2.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Angelini P., Velasco J.A., Flamm S.: Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation 2002; 105: pp. 2449-2454.
2. Angelini P.: Coronary artery anomalies: an entity in search of an identity. Circulation 2007; 115: pp. 1296-1305.
3. Pannu H.K., Flohr T.G., Corl F.M., et. al.: Current concepts in multi-detector row CT evaluation of the coronary arteries: principles, techniques, and anatomy. Radiographics 2003; pp. S111-S125.
4. Taylor A.J., Rogan K.M., Virmani R.: Sudden cardiac death associated with isolated congenital coronary artery anomalies. J Am Coll Cardiol 1992; 20: pp. 640-647.
5. Ichikawa M., Komatsu S., Asanuma H., et. al.: Acute myocardial infarction caused by “malignant” anomalous right coronary artery detected by multidetector row computed tomography. Circ J 2005; 69: pp. 1564-1567.
6. Shi H., Aschoff A.J., Brambs H.J., et. al.: Multislice CT imaging of anomalous coronary arteries. Eur Radiol 2004; 14: pp. 2172-2181.
7. van Ooijen P.M., Dorgelo J., Zijlstra F., et. al.: Detection, visualization and evaluation of anomalous coronary anatomy on 16-slice multidetector-row CT. Eur Radiol 2004; 14: pp. 2163-2171.
8. Chou M.C., Wu M.T., Chen C.H., et. al.: Multidetector CT findings of a congenital coronary sinus anomaly: a report of two cases. Korean J Radiol 2008; pp. S1-S6.
9. Kim S.Y., Seo J.B., Do K.H., et. al.: Coronary artery anomalies: classification and ECG-gated multi-detector row CT findings with angiographic correlation. Radiographics 2006; 26: pp. 317-333. discussion 33–34
10. Sundaram B., Kreml R., Patel S.: Imaging of coronary artery anomalies. Radiol Clin North Am 2010; 48: pp. 711-727.
11. Cademartiri F., Runza G., Luccichenti G., et. al.: Coronary artery anomalies: incidence, pathophysiology, clinical relevance and role of diagnostic imaging. Radiol Med 2006; 111: pp. 376-391.
12. Rodenwaldt J.: Multislice computed tomography of the coronary arteries. Eur Radiol 2003; 13: pp. 748-757.
13. Wilson G.T., Gopalakrishnan P., Tak T.: Noninvasive cardiac imaging with computed tomography. Clin Med Res 2007; 5: pp. 165-171.
14. Duran C., Kantarci M., Durur Subasi I., et. al.: Remarkable anatomic anomalies of coronary arteries and their clinical importance: a multidetector computed tomography angiographic study. J Comput Assist Tomogr 2006; 30: pp. 939-948.
15. Herzog C., Britten M., Balzer J.O., et. al.: Multidetector-row cardiac CT: diagnostic value of calcium scoring and CT coronary angiography in patients with symptomatic, but atypical, chest pain. Eur Radiol 2004; 14: pp. 169-177.
16. Hong C., Bae K.T., Pilgram T.K., et. al.: Coronary artery calcium quantification at multi-detector row CT: influence of heart rate and measurement methods on interacquisition variability initial experience. Radiology 2003; 228: pp. 95-100.
17. Morin R.L., Gerber T.C., McCollough C.H.: Radiation dose in computed tomography of the heart. Circulation 2003; 107: pp. 917-922.
18. Shemesh J., Evron R., Koren-Morag N., et. al.: Coronary artery calcium measurement with multi-detector row CT and low radiation dose: comparison between 55 and 165 mAs. Radiology 2005; 236: pp. 810-814.
19. Landis J.R., Koch G.G.: The measurement of observer agreement for categorical data. Biometrics 1977; 33: pp. 159-174.
20. Maron B.J.: Sudden death in young athletes. N Engl J Med 2003; 349: pp. 1064-1075.
21. Hendel R.C., Patel M.R., Kramer C.M., et. al.: ACCF/ACR/SCCT/SCMR/ASNC/NASCI/SCAI/SIR 2006 appropriateness criteria for cardiac computed tomography and cardiac magnetic resonance imaging: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Criteria Working Group, American College of Radiology, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, American Society of Nuclear Cardiology, North American Society for Cardiac Imaging, Society for Cardiovascular Angiography and Interventions, and Society of Interventional Radiology. J Am Coll Cardiol 2006; 48: pp. 1475-1497.
22. Lee H.J., Kim Y.J., Hur J., et. al.: Coronary artery anomalies: detection on coronary artery calcium scoring scan. AJR Am J Roentgenol 2010; 194: pp. W382-W387.