
Rationale and Objectives
We retrospectively determined if signal enhancement ratio (SER), a quantitative measure of contrast kinetics using volumetric parameters, could reduce the number of biopsy recommendations without decreasing the number of cancers detected when applied to suspicious lesions seen on breast magnetic resonance imaging (MRI).
Materials and Methods
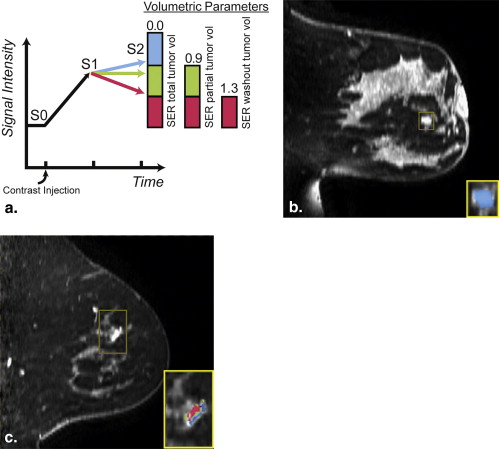
A retrospective review of Breast Imaging Reporting and Data System (BIRADS) 4 or 5 lesions seen on breast MRI in 2008 that were clinically and mammographically occult yielded a final sample size of 73 lesions in 65 patients. Images were processed with in-house software. Parameters used to predict benignity/malignancy included SER total tumor volume (lesion volume above a 70% initial enhancement level), SER partial tumor volume (volume with “washout” and “plateau” kinetics), SER washout tumor volume, peak SER, and peak percent enhancement. Thresholds were determined to retrospectively discriminate benign from malignant histopathology. Clinical impact was assessed through the reduction in the number of biopsies recommended (by eliminating benign lesions discriminated by SER).
Results
Based on the original radiologist interpretations, 73 occult lesions were called suspicious and biopsied with a predictive value of biopsies (PPV 3 ) of 18/73 (25%). SER parameters were found to be significantly associated with histopathology ( P < .05). Biopsy recommendations could be reduced using SER parameters of SER partial tumor volume (73 to 40), SER total tumor volume (73 to 45), and peak percent enhancement (73 to 55) without removing true positives.
Conclusion
The adjunctive use of SER parameters may reduce the number of recommended biopsies without reducing the number of cancers detected.
Breast magnetic resonance imaging (MRI) is the most sensitive method for detecting and diagnosing breast cancer. MRI is able to identify new malignancies occult to mammography or clinical breast examination and is used widely in clinical practice . However, because of its variable specificity, breast MRI has been controversial for causing a high proportion of benign biopsies and changes in surgical management . Improving diagnostic accuracy of histopathology by imaging alone would strongly impact the clinical management of these lesions. Increasing the specificity of MRI is a particular unmet need and could be resolved through better discrimination of which lesions are benign and therefore don’t require biopsy.
Signal enhancement ratio (SER), a quantitative method for characterizing neoangiogenesis in breast cancer, is a semiautomated, reproducible, computational analysis of MRI images acquired in regular clinical practice . It measures change in contrast signal intensity over three time points and acts as a surrogate marker for contrast kinetics. The overall analysis monotonically approximates the redistribution rate constant ( k ep ) in a two-compartment pharmacokinetic model when postcontrast time points are sampled appropriately . Variations of the SER technique have been incorporated in computer-aided detection breast MRI software. The SER technique has been applied in a variety of implementations, including curve classification, most-suspicious pixel cluster, or enhancing lesion volume . Although these investigations have looked at the ability of SER to improve diagnostic accuracy, few have specifically reviewed the impact of volumetric parameters.
Get Radiology Tree app to read full this article<
Materials and methods
Study Subjects and Lesions
Get Radiology Tree app to read full this article<
Table 1
Histopathology of 73 Biopsied Breast Lesions
Histopathology Malignant ( n = 18) Benign ( n = 55) Malignant Ductal carcinoma in situ (DCIS) 3 Invasive ductal ( DCIS) 12 Invasive lobular 1 Invasive periductal stromal 1 Invasive papillary 1 Benign Fibroadenoma 13 Normal breast tissue 12 Fibrocystic 7 Stromal fibrosis 5 Lymph node 5 Usual ductal hyperplasia 3 Apocrine metaplasia 3 Pseudoangiomatous stromal hyperplasia 3 Atypical lobular hyperplasia 1 Intraductal papilloma 1 Lobular carcinoma in situ 1 Cysts 1
Get Radiology Tree app to read full this article<
MRI Acquisition
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of Traditional MRI Parameters and Signal Enhancement Ratio (SER) Values between Malignant and Benign Lesions
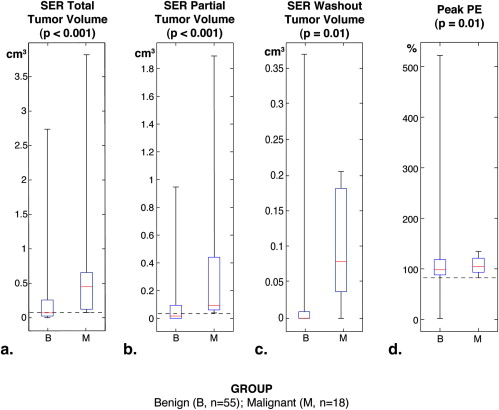
Parameter Malignant ( n = 18) Benign ( n = 55)P Value Mean lesion diameter, cm. (SD) 1.3 (0.7) 1.2 (0.8) .40 Enhancement type .12 Mass 15 30 Nonmass 1 10 Focus 2 15 SER total tumor volume, cm 3 0.45 (0.08–3.80) 0.07 (0–2.72) <.001 SER partial tumor volume, cm 3 0.09 (0.04–1.89) 0.02 (0–0.98) <.001 SER washout tumor volume, cm 3 0.01 (0–0.21) 0.0003 (0–0.38) .01 Peak SER ∗ 1.40 (0.99–2.92) 1.21 (0.42–3) .10 Peak PE 103% (82–138) 91% (2–522) .01
Data were non-normally distributed and statistically compared nonparametrically using Wilcoxon rank-sum test. Results are expressed as median (minimum-maximum).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Clinical Impact of MRI Signal Enhancement Ratio (SER) Parameters
Method Biopsies Recommended PPV 3 (Biopsy Yield of Malignancy) Initial MRI interpretation 73 25% Total tumor volume 45 40% SER partial tumor volume 40 45% SER washout tumor volume 73 25% Peak PE 55 33%
MRI, magnetic resonance imaging; PE, percent enhancement; SER, signal enhancement ratio.
Biopsies recommended are based on the number of total biopsies recommended by original radiologist’s MRI interpretation minus lesions retrospectively predicted to be benign using empirically derived thresholds at which a parameter performs with 100% sensitivity.
Initial MRI interpretation is defined as the original radiologists’ interpretations performed prospectively as part of routine clinical care and incorporates both Breast Imaging Reporting and Data System morphologic descriptors and a qualitative assessment of contrast kinetics.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Kuhl C.K.: Current status of breast MR imaging. Part 2. Clinical applications. Radiology 2007; 244: pp. 672-691.
2. Lehman C.D., Gatsonis C., Kuhl C.K., et. al.: MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356: pp. 1295-1303.
3. Bassett L.W., Dhaliwal S.G., Eradat J., et. al.: National trends and practices in breast MRI. AJR Am J Roentgenol 2008; 191: pp. 332-339.
4. Houssami N., Hayes D.: Review of preoperative magnetic resonance imaging (MRI) in breast cancer: should MRI be performed on all women with newly diagnosed, early stage breast cancer?. CA: Cancer J Clin 2009; 59: pp. 290-302.
5. Kuhl C., Kuhn W., Braun M., et. al.: Pre-operative staging of breast cancer with breast MRI: one step forward, two steps back?. Breast 2007; 16: pp. S34-S44.
6. Hylton N.: Dynamic contrast-enhanced magnetic resonance imaging as an imaging biomarker. J Clin Oncol 2006; 24: pp. 3293-3298.
7. Tofts P.S.: Modeling tracer kinetics in dynamic Gd-DTPA MR imaging. J Magnet Res Imaging JMRI 1997; 7: pp. 91-101.
8. Li K.L., Henry R.G., Wilmes L.J., et. al.: Kinetic assessment of breast tumors using high spatial resolution signal enhancement ratio (SER) imaging. Magnet Res Med 2007; 58: pp. 572-581.
9. Esserman L., Hylton N., George T., et. al.: Contrast-enhanced magnetic resonance imaging to assess tumor histopathology and angiogenesis in breast carcinoma. Breast J 1999; 5: pp. 13-21.
10. Hylton N.M.: Vascularity assessment of breast lesions with gadolinium-enhanced MR imaging. Magn Reson Imaging Clin N Am 1999; 7: pp. 411-420. x
11. Lehman C.D., Peacock S., DeMartini W.B., et. al.: A new automated software system to evaluate breast MR examinations: improved specificity without decreased sensitivity. AJR Am J Roentgenol 2006; 187: pp. 51-56.
12. Wang L.C., DeMartini W.B., Partridge S.C., et. al.: MRI-detected suspicious breast lesions: predictive values of kinetic features measured by computer-aided evaluation. AJR Am J Roentgenol 2009; 193: pp. 826-831.
13. Eby P.R., Partridge S.C., White S.W., et. al.: Metabolic and vascular features of dynamic contrast-enhanced breast magnetic resonance imaging and (15)O-water positron emission tomography blood flow in breast cancer. Acad Radiol 2008; 15: pp. 1246-1254.
14. Karahaliou A., Vassiou K., Arikidis N.S., et. al.: Assessing heterogeneity of lesion enhancement kinetics in dynamic contrast-enhanced MRI for breast cancer diagnosis. Br J Radiol 2010; 83: pp. 296-309.
15. D’Orsi C.J., Bassett L.W., Berg W.A., et. al.: Breast Imaging Reporting and Data System: ACR BI-RADS-Mammography.4th ed2003.American College of RadiologyReston, VA
16. ACRIN. Protocol 6657. In: American College of Radiology Imaging Network (ACRIN). Available online at: www.acrin.org/6657_protocol.aspx .
17. Moon M., Cornfeld D., Weinreb J.: Dynamic contrast-enhanced breast MR imaging. Magn Reson Imaging Clin N Am 2009; 17: pp. 351-362.
18. Szabo B.K., Aspelin P., Wiberg M.K., et. al.: Dynamic MR imaging of the breast. Analysis of kinetic and morphologic diagnostic criteria. Acta Radiol 2003; 44: pp. 379-386.
19. Williams T.C., DeMartini W.B., Partridge S.C., et. al.: Breast MR imaging: computer-aided evaluation program for discriminating benign from malignant lesions. Radiology 2007; 244: pp. 94-103.
20. Baltzer P.A., Renz D.M., Kullnig P.E., et. al.: Application of computer-aided diagnosis (CAD) in MR-mammography (MRM): do we really need whole lesion time curve distribution analysis?. Acad Radiol 2009; 16: pp. 435-442.
21. Levman J.E., Causer P., Warner E., et. al.: Effect of the enhancement threshold on the computer-aided detection of breast cancer using MRI. Acad Radiol 2009; 16: pp. 1064-1069.
22. Paldino M.J., Barboriak D.P.: Fundamentals of quantitative dynamic contrast-enhanced MR imaging. Magn Reson Imaging Clin N Am 2009; 17: pp. 277-289.
23. Kelcz F., Furman-Haran E., Grobgeld D., et. al.: Clinical testing of high-spatial-resolution parametric contrast-enhanced MR imaging of the breast. AJR Am J Roentgenol 2002; 179: pp. 1485-1492.
24. Hauth E.A., Stockamp C., Maderwald S., et. al.: Evaluation of the three-time-point method for diagnosis of breast lesions in contrast-enhanced MR mammography. Clin Imaging 2006; 30: pp. 160-165.
25. Jansen S.A., Shimauchi A., Zak L., et. al.: Kinetic curves of malignant lesions are not consistent across MRI systems: need for improved standardization of breast dynamic contrast-enhanced MRI acquisition. AJR Am J Roentgenol 2009; 193: pp. 832-839.