
Rationale and Objectives
To determine the benefit of using whole-body low-dose computed tomography (WBLD-CT) in patients with monoclonal gammopathy of undetermined significance (MGUS) for exclusion of multiple myeloma (MM) bone disease.
Materials and Methods
Seventy-one consecutive patients with confirmed MGUS (as defined by the latest criteria of the International Myeloma Working Group) who underwent WBLD-CT for diagnosis were identified retrospectively by a search of our institution’s electronic medical record database (2002–2009). Patients were classified as low-risk or intermediate/high-risk and followed over a ≥2-year period with additional CT imaging and/or laboratory parameters. Presence of osteolysis, medullary, or extramedullary abnormalities compatible with involvement by MM was recorded. A diffuse or focal increase in medullary density to Hounsfield unit (HU) values >20 HU/>0 HU was considered suspicious for bone marrow infiltration if no other causes identifiable.
Results
The presence of osteolysis was excluded in all 71 patients with MGUS at initial diagnosis and patients were surveilled for ≥2 years. Lytic changes were observed at follow-up in1/71 patients that progressed to MM and were detectable via WBLD-CT at an early stage (even before a significant rise in M-protein was recorded). In 3/71 patients with MGUS (4%) suspicious bone marrow attenuation values were measured, disclosing disease progression to smoldering myeloma in another patient and false-positive results in 2/71 patients. Bone marrow attenuation assessment resulted in a specificity and negative predictive value of 97%, respectively. No significant difference with respect to bone marrow attenuation was observed in patients with low-risk MGUS versus intermediate- to high-risk MGUS. One of 71 patients showed serologic disease progression to active MM without bone abnormalities detectable.
Conclusion
WBLD-CT reliably excludes findings compatible with myeloma in MGUS and thereby complements hematologic laboratory analysis.
A total of 3.2% of the population age 50 years or older and 5.3% of persons older than 70 years present with a monoclonal gammopathy of undetermined significance (MGUS) . MGUS is defined as the presence of a monoclonal protein (M protein) in the serum at a concentration of <3 g/dL, an amount of <10% plasma cells in the bone marrow and no additional features of plasma cell disease, such as lytic bone lesions, anemia, hypercalcemia, or renal insufficiency . Because this premalignant condition consistently precedes multiple myeloma (MM) with an average 1% annual risk of progression, regular follow-up needs to be performed .
In MM the most widely used staging system is based on the Durie-Salmon criteria encompassing the presence of lytic bone lesions on radiographs, a decrease in hemoglobin, an increase in serum calcium, the amount of M protein, and renal function . However, because at least 30%–50% of the bone mass needs to be destructed for a lytic lesion to become apparent on a radiograph , a substantial number of MM lesions (both within bone and extraosseous) are missed by conventional radiography . Because low-dose computed tomography (CT) is a sensitive imaging tool for the detection of destructive bone lesions, we routinely perform a whole-body low-dose multidetector CT (WBLD-CT) at our institution to exclude lytic bone involvement in patients presenting with a monoclonal gammopathy . WBLD-CT enables an accurate assessment of osteolysis in the entire skeleton and allows for a concise evaluation of the appendicular and pelvic bone marrow including the less frequent extramedullary involvement . Several studies revealed focal bone marrow abnormalities in MGUS patients via magnetic resonance (MR) imaging leading to redivivus interest in the Durie-Salmon PLUS staging system , even though prediction of overall survival was not improved by the latter . No data exist in the current literature concerning the applicability and the relevance of WBLD-CT in patients with MGUS.
Get Radiology Tree app to read full this article<
Materials and methods
Population
Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Laboratory Data
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Population and Disease Course
Get Radiology Tree app to read full this article<
Bone Marrow Attenuation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Recognition of Osteolysis via WBLD-CT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
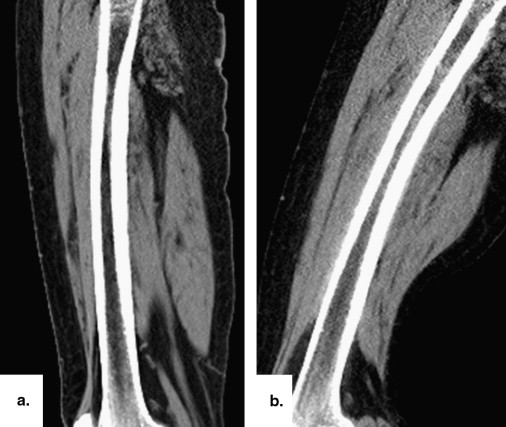
![Figure 3, A 78-year-old male patient with progressive multiple myeloma (immunoglobulin G kappa). At initial whole-body low-dose computed tomography (a) , mildly elevated bone marrow attenuation values were observed (around 22 Hounsfield units [HU], M-protein 1.3 g/dL). At 1.5 years later (b) , the patient progressed to high-grade multiple myeloma and bone marrow attenuation values increased to 60 HU (M-protein 3.4 g/dL). Dexter, a magnification of the left femur ( arrows ) is shown.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/CanWholebodyLowdoseMultidetectorCTExcludethePresenceofMyelomaBoneDiseaseinPatientswithMonoclonalGammopathyofUndeterminedSignificanceMGUS/2_1s20S1076633211004533.jpg)
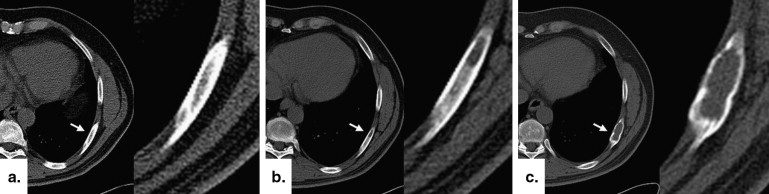
![Figure 4, Confident exclusion of monoclonal gammopathy of undetermined significance (MGUS) in a 78-year-old male patient with progressive multiple myeloma (immunoglobulin G kappa; same patient as in Figure 3 ). At initial whole-body low-dose computed tomography (a) , solitary osteolytic changes in the left lateral mass of the sacral bone are demonstrated allowing reliable exclusion of the MGUS status and timely diagnosis of multiple myeloma (MM). The M-protein was unremarkable at that time (M-protein 1.3 g/dL) and only mildly elevated bone marrow attenuation values were observed (around 22 Hounsfield units [HU]; see Figure 3 ). At 1.5 years later (b) , the patient developed high-grade MM with multifocal osteolysis. Note the progressive destruction of the left sacral bone with medullary outgrowth into the sacral neuroforamina ( arrow ). Bone marrow attenuation values increased to 60 HU (see Figure 3 , M-protein 3.4 g/dL). In the lower row, a magnification of the sacral bone is shown and the lytic changes are indicated ( arrows ).](https://storage.googleapis.com/dl.dentistrykey.com/clinical/CanWholebodyLowdoseMultidetectorCTExcludethePresenceofMyelomaBoneDiseaseinPatientswithMonoclonalGammopathyofUndeterminedSignificanceMGUS/3_1s20S1076633211004533.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Kyle R.A., Therneau T.M., Rajkumar S.V., et. al.: Prevalence of monoclonal gammopathy of undetermined significance. N Engl J Med 2006; 354: pp. 1362-1369.
2. Kyle R.A., Rajkumar S.V.: Monoclonal gammopathy of undetermined significance. Br J Haematol 2006; 134: pp. 573-589.
3. Kyle R.A., Therneau T.M., Rajkumar S.V., et. al.: A long-term study of prognosis in monoclonal gammopathy of undetermined significance. N Engl J Med 2002; 346: pp. 564-569.
4. Landgren O., Kyle R.A., Pfeiffer R.M., et. al.: Monoclonal gammopathy of undetermined significance (MGUS) consistently precedes multiple myeloma: a prospective study. Blood 2009; 113: pp. 5412-5417.
5. Durie B.G., Salmon S.E.: A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 1975; 36: pp. 842-854.
6. Horger M., Claussen C.D., Bross-Bach U., et. al.: Whole-body low-dose multidetector row-CT in the diagnosis of multiple myeloma: an alternative to conventional radiography. Eur J Radiol 2005; 54: pp. 289-297.
7. Mahnken A.H., Wildberger J.E., Gehbauer G., et. al.: Multidetector CT of the spine in multiple myeloma: comparison with MR imaging and radiography. AJR Am J Roentgenol 2002; 178: pp. 1429-1436.
8. Fechtner K., Hillengass J., Delorme S., et. al.: Staging monoclonal plasma cell disease: comparison of the Durie-Salmon and the Durie-Salmon PLUS staging systems. Radiology 2010; 257: pp. 195-204.
9. Horger M., Pereira P., Claussen C.D., et. al.: Hyperattenuating bone marrow abnormalities in myeloma patients using whole-body non-enhanced low-dose MDCT: correlation with haematological parameters. Br J Radiol 2008; 81: pp. 386-396.
10. Vande Berg B.C., Michaux L., Lecouvet F.E., et. al.: Nonmyelomatous monoclonal gammopathy: correlation of bone marrow MR images with laboratory findings and spontaneous clinical outcome. Radiology 1997; 202: pp. 247-251.
11. Bäuerle T., Hillengass J., Fechtner K., et. al.: Multiple myeloma and monoclonal gammopathy of undetermined significance: importance of whole-body versus spinal MR imaging. Radiology 2009; 252: pp. 477-485.
12. Durie B.G., Kyle R.A., Belch A., et. al.: Scientific Advisors of the International Myeloma Foundation. Myeloma management guidelines: a consensus report from the Scientific Advisors of the International Myeloma Foundation. Hematol J 2003; 4: pp. 379-398.
13. International Myeloma Working Group: Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol 2003; 121: pp. 749-757.
14. Cosentini T., Le Donne R., Mancini D., et. al.: Magnetic resonance imaging evaluation of bone marrow changes in obstructive sleep apnoea syndrome in adults. Radiol Med 2006; 111: pp. 572-584.
15. Poulton T.B., Murphy W.D., Duerk J.L., et. al.: Bone marrow reconversion in adults who are smokers: MR imaging findings. AJR Am J Roentgenol 1993; 161: pp. 1217-1221.
16. Kyle R.A., Durie B.G., Rajkumar S.V., et. al.: International Myeloma Working Group. Monoclonal gammopathy of undetermined significance (MGUS) and smoldering (asymptomatic) multiple myeloma: IMWG consensus perspectives risk factors for progression and guidelines for monitoring and management. Leukemia 2010; 24: pp. 1121-1127.
17. Landgren O.: Monoclonal gammopathy of undetermined significance and smoldering myeloma: new insights into pathophysiology and epidemiology. Hematol Am Soc Hematol Educ Program 2010; 2010: pp. 295-302.
18. Bladé J.: Clinical practice. Monoclonal gammopathy of undetermined significance. N Engl J Med 2006; 355: pp. 2765-2770.
19. Bladé J., Rosiñol L., Cibeira M.T., et. al.: Pathogenesis and progression of monoclonal gammopathy of undetermined significance. Leukemia 2008; 22: pp. 1651-1657.
20. Pepe J., Petrucci M.T., Nofroni I., et. al.: Lumbar bone mineral density as the major factor determining increased prevalence of vertebral fractures in monoclonal gammopathy of undetermined significance. Br J Haematol 2006; 134: pp. 485-490.
21. Kristinsson S.Y., Pfeiffer R.M., Björkholm M., et. al.: Arterial and venous thrombosis in monoclonal gammopathy of undetermined significance and multiple myeloma: a population-based study. Blood 2010; 115: pp. 4991-4998.
22. Lecouvet F.E., Vande Berg B.C., Michaux L., et. al.: Stage III multiple myeloma: clinical and prognostic value of spinal bone marrow MR imaging. Radiology 1998; 209: pp. 653-660.
23. Sager S., Ergül N., Ciftci H., et. al.: The value of FDG PET/CT in the initial staging and bone marrow involvement of patients with multiple myeloma. Skeletal Radiol 2011; [Epub ahead of print]
24. Horger M., Kanz L., Denecke B., et. al.: The benefit of using whole-body, low-dose, nonenhanced, multidetector computed tomography for follow-up and therapy response monitoring in patients with multiple myeloma. Cancer 2007; 109: pp. 1617-1626.
25. Huang B., Li J., Law M.W., et. al.: Radiation dose and cancer risk in retrospectively and prospectively ECG-gated coronary angiography using 64-slice multidetector CT. Br J Radiol 2010; 83: pp. 152-158.