
Rationale and Objectives
We investigated the feasibility of detecting left ventricular (LV) cardiac magnetic resonance (CMR) strain abnormalities using feature-tracking in patients with pulmonary hypertension (PH).
Materials and Methods
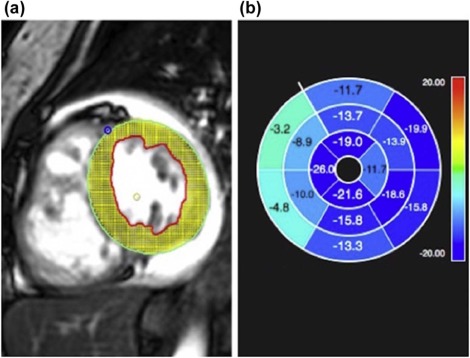
CMR was performed in 16 patients with all groups of PH and in 13 controls. Global and regional peak circumferential strains (%) (which have been shown to be robust by CMR), peak diastolic strain rate (%/s), and dyssynchrony index (ms) were quantified with feature-tracking software. Ventricular function and volumes were calculated from CMR, and right heart pressures were measured with catheterization.
Results
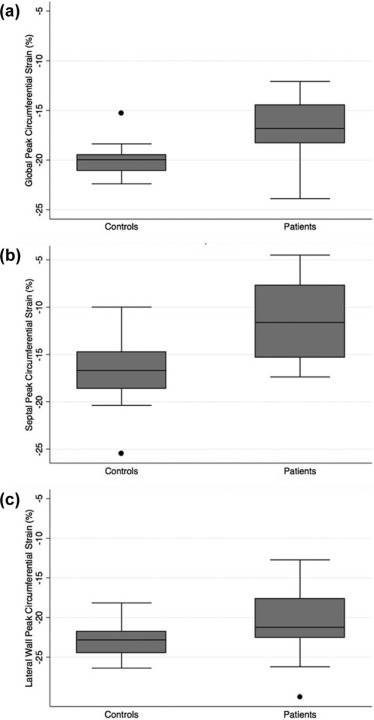
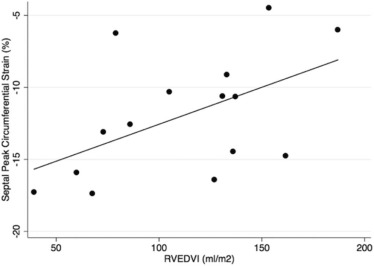
Left ventricular ejection fraction (LVEF) was similar in patients (60.2% ± 11.0%) and controls (61.9% ± 4.5%), P = .150. Global LV peak circumferential strain was significantly different in patients compared to controls, −16.7 ± 2.8% vs −19.9 ± 1.8%, respectively ( P = .001). The greatest difference in strain was seen in the LV septum, −11.6 ± 4.3% in patients vs −16.7 ± 4.0% in controls ( P < .001). There was a significant association between septal strain and right ventricular end-diastolic volume index ( P = .047) in patients with PH; however, there were no associations with pulmonary artery pressures or right ventricular ejection fraction.
Conclusions
Feature-tracking CMR can detect LV strain abnormalities in patients with PH and preserved or mildly depressed LVEF, with greatest abnormality in the septum. The association between septal strain and right ventricular end-diastolic volume index suggests that ventricular interdependence may be a mechanism of LV dysfunction in PH. Feature-tracking CMR may be useful for identification of LV dysfunction before LVEF significantly declines in patients with PH. The feasibility of detecting LV strain abnormalities in patients with PH shown by this study paves the way for a variety of future investigations into the applications of LV strain in this patient population.
Introduction
Pulmonary hypertension (PH) is a progressive, chronic disease characterized by sustained elevation of resting mean pulmonary artery pressure of 25 mmHg or greater. The World Health Organization (WHO) classifies PH into five major groups: pulmonary arterial hypertension (PAH), PH due to left heart disease, due to lung disease or hypoxia, chronic thromboembolic PH, and PH with unclear multifactorial mechanisms . Despite significant progress in medical management of PAH, overall prognosis remains poor, as shown in an analysis of patients with PAH that demonstrated 1-, 3-, 5-, and 7-year survival rates of 85%, 68%, 57%, and 49% .
A major limitation of the current management of patients with PH is the requirement for invasive cardiac catheterization to evaluate pulmonary artery pressures to risk-stratify patients and evaluate treatment response. The invasive tests performed in patients with PH expose the patients to procedural risks and radiation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
TABLE 1
Demographics, Volumetric, and Functional Parameters in Patients with Pulmonary Hypertension Versus Controls
Controls
n = 13 Patients
n = 16 Unadjusted
P Value Age-adjusted P Value Age—years 35.6 ± 12.0 52.9 ± 16.5 .004 — Male (%) 6/13 (46%) 5/16 (31%) .429 .989 White (%) 6/13 (46%) 10/16 (63%) .397 .173 LVEF (%) 61.9% ± 4.5% 60.2% ± 11.0% .634 .150 RVEF (%) 53.3% ± 5.6% 41.0% ± 15.4% .019 .085 LVEDVI mL/m 2 97.0 ± 36.3 73.0 ± 24.9 .057 .571 RVEDVI mL/m 2 96.6 ± 42.0 111.7 ± 42.55 .377 .177 RBBB — 5/16 (31%) — —
LVEDVI, left ventricular end-diastolic volume index; LVEF, left ventricular ejection fraction; RBBB, right bundle branch block; RVEDVI, right ventricular end-diastolic volume index; RVEF, right ventricular ejection fraction.
Continuous variables are expressed as mean ± standard deviation.
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Parameters
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Demographics
Get Radiology Tree app to read full this article<
CMR Function and Volumetrics
Get Radiology Tree app to read full this article<
Echocardiography
Get Radiology Tree app to read full this article<
Cardiac Catheterization
Get Radiology Tree app to read full this article<
Electrocardiography
Get Radiology Tree app to read full this article<
CMR Strain
Get Radiology Tree app to read full this article<
TABLE 2
Strain Analyses in Patients with Pulmonary Hypertension Versus Controls
Controls
n = 13 Patients
n = 16 Unadjusted
P Value Age-adjusted P Value Global strain (%) −19.9% ± 1.8% −16.7% ± 2.8% .002 .001 Septal strain (%) −16.7% ± 4.0% −11.6% ± 4.3% .003 <.001 Lateral wall strain (%) −22.9% ± 2.2% −20.5% ± 4.7% .096 .273 Dyssynchrony index (ms) 61.5 ± 7.9 74.4 ± 21.2 .047 .198 Diastolic strain rate (%/s) 121.0 ± 27.2 115.1 ± 42.4 .667 .988
ms, milliseconds; s, seconds.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Regression Analyses
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Simonneau G., Gatzoulis M.A., Adatia I., et. al.: Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013; 62: pp. D34-D41.
2. Benza R.L., Miller D.P., Barst R.J., et. al.: An evaluation of long-term survival from time of diagnosis in pulmonary arterial hypertension from the REVEAL Registry. Chest 2012; 142: pp. 448-456.
3. Voelkel N.F., Quaife R.A., Leinwand L.A., et. al.: Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation 2006; 114: pp. 1883-1891.
4. van de Veerdonk M.C., Kind T., Marcus J.T., et. al.: Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol 2011; 58: pp. 2511-2519.
5. Kindberg K., Haraldsson H., Sigfridsson A., et. al.: Myocardial strains from 3D displacement encoded magnetic resonance imaging. BMC Med Imaging 2012; 12: pp. 9.
6. Kindberg K., Haraldsson H., Sigfridsson A., et. al.: Temporal 3D Lagrangian strain from 2D slice-followed cine DENSE MRI. Clin Physiol Funct Imaging 2012; 32: pp. 139-144.
7. Leong D.P., De Pasquale C.G., Selvanayagam J.B.: Heart failure with normal ejection fraction: the complementary roles of echocardiography and CMR imaging. JACC Cardiovasc Imaging 2010; 3: pp. 409-420.
8. Ordovas K.G., Carlsson M., Lease K.E., et. al.: Impaired regional left ventricular strain after repair of tetralogy of Fallot. J Magn Reson Imaging 2012; 35: pp. 79-85.
9. Brauchlin A.E., Soccal P.M., Rochat T., et. al.: Severe left ventricular dysfunction secondary to primary pulmonary hypertension: bridging therapy with bosentan before lung transplantation. J Heart Lung Transplant 2005; 24: pp. 777-780.
10. Pielsticker E.J., Martinez F.J., Rubenfire M.: Lung and heart-lung transplant practice patterns in pulmonary hypertension centers. J Heart Lung Transplant 2001; 20: pp. 1297-1304.
11. Burkett D.A., Slorach C., Patel S.S., et. al.: Left ventricular myocardial function in children with pulmonary hypertension: relation to right ventricular performance and hemodynamics. Circ Cardiovasc Imaging 2015; 8:
12. Hor K.N., Baumann R., Pedrizzetti G., et. al.: Magnetic resonance derived myocardial strain assessment using feature tracking. J Vis Exp 2011; 48:
13. Schuster A., Hor K.N., Kowallick J.T., et. al.: Cardiovascular magnetic resonance myocardial feature tracking: concepts and clinical applications. Circ Cardiovasc Imaging 2016; 9: pp. e004077.
14. Pedrizzetti G., Claus P., Kilner P.J., et. al.: Principles of cardiovascular magnetic resonance feature tracking and echocardiographic speckle tracking for informed clinical use. J Cardiovasc Magn Reson 2016; 18: pp. 51.
15. de Siqueira M.E., Pozo E., Fernandes V.R., et. al.: Characterization and clinical significance of right ventricular mechanics in pulmonary hypertension evaluated with cardiovascular magnetic resonance feature tracking. J Cardiovasc Magn Reson 2016; 18: pp. 39.
16. Schuster A., Stahnke V.C., Unterberg-Buchwald C., et. al.: Cardiovascular magnetic resonance feature-tracking assessment of myocardial mechanics: intervendor agreement and considerations regarding reproducibility. Clin Radiol 2015; 70: pp. 989-998.
17. Morton G., Schuster A., Jogiya R., et. al.: Inter-study reproducibility of cardiovascular magnetic resonance myocardial feature tracking. J Cardiovasc Magn Reson 2012; 14: pp. 43.
18. Padiyath A., Gribben P., Abraham J.R., et. al.: Echocardiography and cardiac magnetic resonance-based feature tracking in the assessment of myocardial mechanics in tetralogy of Fallot: an intermodality comparison. Echocardiography 2013; 30: pp. 203-210.
19. Onishi T., Saha S.K., Delgado-Montero A., et. al.: Global longitudinal strain and global circumferential strain by speckle-tracking echocardiography and feature-tracking cardiac magnetic resonance imaging: comparison with left ventricular ejection fraction. J Am Soc Echocardiogr 2015; 28: pp. 587-596.
20. Cerqueira M.D., Weissman N.J., Dilsizian V., et. al.: Standardized myocardial segmentation and nomenclature for tomographic imaging of the heart. A statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. Int J Cardiovasc Imaging 2002; 18: pp. 539-542.
21. Helm R.H., Leclercq C., Faris O.P., et. al.: Cardiac dyssynchrony analysis using circumferential versus longitudinal strain: implications for assessing cardiac resynchronization. Circulation 2005; 111: pp. 2760-2767.
22. Rosen B.D., Fernandes V.R., Nasir K., et. al.: Age, increased left ventricular mass, and lower regional myocardial perfusion are related to greater extent of myocardial dyssynchrony in asymptomatic individuals: the multi-ethnic study of atherosclerosis. Circulation 2009; 120: pp. 859-866.
23. Kjaer A., Lebech A.M., Hesse B., et. al.: Right-sided cardiac function in healthy volunteers measured by first-pass radionuclide ventriculography and gated blood-pool SPECT: comparison with cine MRI. Clin Physiol Funct Imaging 2005; 25: pp. 344-349.
24. Haeck M.L., Hoke U., Marsan N.A., et. al.: Impact of right ventricular dyssynchrony on left ventricular performance in patients with pulmonary hypertension. Int J Cardiovasc Imaging 2014; 30: pp. 713-720.
25. Louie E.K., Lin S.S., Reynertson S.I., et. al.: Pressure and volume loading of the right ventricle have opposite effects on left ventricular ejection fraction. Circulation 1995; 92: pp. 819-824.
26. Lin S.S., Reynertson S.I., Louie E.K., et. al.: Right ventricular volume overload results in depression of left ventricular ejection fraction. Implications for the surgical management of tricuspid valve disease. Circulation 1994; 90: pp. II209-II213.
27. Puwanant S., Park M., Popovic Z.B., et. al.: Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension. Circulation 2010; 121: pp. 259-266.
28. Hardegree E.L., Sachdev A., Fenstad E.R., et. al.: Impaired left ventricular mechanics in pulmonary arterial hypertension: identification of a cohort at high risk. Circ Heart Fail 2013; 6: pp. 748-755.
29. Gan C., Lankhaar J.W., Marcus J.T., et. al.: Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol 2006; 290: pp. H1528-H1533.
30. Muzzarelli S., Ordovas K.G., Cannavale G., et. al.: Tetralogy of Fallot: impact of the excursion of the interventricular septum on left ventricular systolic function and fibrosis after surgical repair. Radiology 2011; 259: pp. 375-383.