
Rationale and Objectives
To identify and compare cardiovascular findings on computed tomography (CT) scans after pneumonectomy (PNX) with those after lobectomy (LOBX).
Materials and Methods
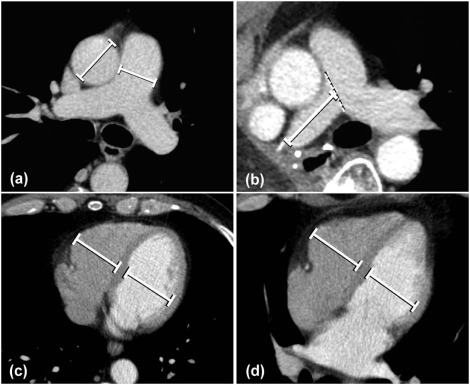
Pre- and postoperative CT scans from 25 PNX patients were retrospectively analyzed and compared to those from 30 LOBX patients. The diameter of the main pulmonary artery (PA) and its ratio to the ascending aorta (PA/Ao) were determined. Cardiac morphometry values were ascertained by measuring maximum diameters of the right and left ventricle on axial (RV axial , LV axial ) and four-chamber (RV 4-ch , LV 4-ch ) views. RV axial /LV axial and RV 4-ch /LV 4-ch ratios were calculated. Vessel stumps were evaluated for thrombosis.
Results
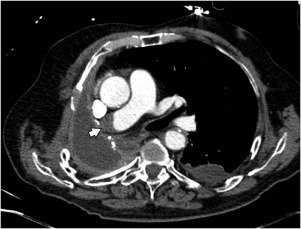
After PNX, PA (31.1 ± 5.8 mm vs 28.7 ± 5.4 mm, P = 0.003), PA/Ao (0.97 ± 0.15 vs 0.86 ± 0.12, P = 0.0001), and cardiac morphometry values significantly increased (RV axial 43.6 ± 7.4 vs 39.4 ± 7.1, P = 0.029; RV 4-ch 41.1 ± 6.3 vs 37.6 ± 5.7, P = 0.041; RV axial /LV axial 1.18 ± 0.27 vs 1.03 ± 0.22, P = 0.04; RV 4-ch /LV 4-ch 1.17 ± 0.21 vs 1.02 ± 0.16, P = 0.03). There were no significant differences between right and left PNX. One case of PA stump thrombosis was identified after right PNX. LOBX resulted in a significant increase in PA (30.6 ± 4.3 vs 28.7 ± 3.5, P = 0.005) and PA/Ao (0.90 ± 0.09 vs 0.85 ± 0.10, P = 0.017), whereas cardiac morphometry values were not significantly changed compared to baseline values. No vessel stump thrombosis was observed after LOBX. In comparison to LOBX, all ascertained values were significantly elevated after PNX.
Conclusions
Morphologic alterations of the cardiovascular system following PNX can be identified on CT scans. Alterations are more distinct after PNX compared to LOBX.
Introduction
Pneumonectomy (PNX) has various early and late effects on the cardiovascular system that are based on displacement of the heart and major vessels , altered hemodynamics in vessel stumps , increased perfusion to the remaining lung tissue , and elevated vascular resistance . In about 40% of patients after PNX these effects were shown to induce pulmonary hypertension (PH), that is, resting mean pulmonary artery pressures (PAP) exceeding 25 mmHg with concomitant dysfunction and remodeling of the right ventricle .
Doppler echocardiography was found to be useful in the evaluation of patients undergoing PNX as the right ventricular function and morphology as well as PAP can be assessed noninvasively .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Patients’ Characteristics
Pneumonectomy LobectomyMale 17 17Female 8 13Mean age at surgery (range) 61.3(40–73) 64.3(46–81)Right 11 Upper lobe 14
Lower lobe 2
Middle lobe 4Left 14 Upper lobe 6
Lower lobe 4Indication Bronchogenic carcinoma 19 25 Metastases from extrapulmonary malignancy 2 3 Pleural empyema 1 — Bleeding from pulmonary artery aneurysm — 1 Tuberculosis 1 — Bronchial carcinoid tumor 1 1 Lung abscess 1 —
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Thoracic Vessels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cardiac Morphometry
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
PNX
Get Radiology Tree app to read full this article<
Table 2
Morphometric Data Before and After PNX
Before PNX After PNX_P_ Value Interobserver Agreement Bias \* 95% Limits of Agreement † PA [mm] 28.7 ± 5.4 31.1 ± 5.8 0.003 −0.062 [−0.63, 0.50] PA/Ao 0.86 ± 0.12 0.97 ± 0.15 0.0001 −0.003 [−0.06, 0.05] RV axial [mm] 39.4 ± 7.1 43.6 ± 7.4 0.029 0.052 [−0.53, 0.63] RV 4-ch [mm] 37.6 ± 5.7 41.1 ± 6.3 0.041 −0.130 [−0.83, 0.57] RV axial /LV axial 1.03 ± 0.22 1.18 ± 0.27 0.04 −0.010 [−0.07, 0.05] RV 4-ch /LV 4-ch 1.02 ± 0.16 1.17 ± 0.21 0.03 −0.039 [−0.11, 0.03]
Ao, diameter of the ascending aorta; LV 4-ch , left ventricular diameter in four-chamber view; LV axial , left ventricular diameter on axial sections; PA, pulmonary artery diameter; PNX, pneumonectomy; RV 4-ch , right ventricular diameter in four-chamber view; RV axial , right ventricular diameter on axial sections.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Right PNX Versus Left PNX
Get Radiology Tree app to read full this article<
Table 3
Morphometric Data of Patients Who Underwent Right or Left PNX
After Right PNX After Left PNX_P_ Value PA [mm] 31.6 ± 5.4 34.1 ± 5.8 ns PA/Ao 0.99 ± 0.15 0.99 ± 0.14 ns RV axial [mm] 41.4 ± 8.4 42.3 ± 7.8 ns RV 4-ch [mm] 38.1 ± 5.4 41.6 ± 1.1 ns RV axial /LV axial 1.12 ± 0.17 1.20 ± 0.33 ns RV 4-ch /LV 4-ch 1.12 ± 0.13 1.16 ± 0.25 ns PA stump length [mm] 31.5 ± 12.0 12.9 ± 9.5 <0.0001
Ao, diameter of the ascending aorta; LV 4-ch , left ventricular diameter in four-chamber view; LV axial , left ventricular diameter on axial sections; ns, not significant; PA, pulmonary artery diameter; PNX, pneumonectomy; RV 4-ch , right ventricular diameter in four-chamber view; RV axial , right ventricular diameter on axial sections.
Get Radiology Tree app to read full this article<
LOBX
Get Radiology Tree app to read full this article<
Table 4
Morphometric Data of Patients Before and After LOBX
Before LOBX After LOBX_P_ Value Interobserver Agreement Bias \* 95% Limits of Agreement † PA [mm] 28.7 ± 3.5 30.6 ± 4.3 0.005 −0.005 [−0.59, 0.58] PA/Ao 0.85 ± 0.10 0.90 ± 0.09 0.017 −0.020 [−0.08, 0.04] RV axial [mm] 38.0 ± 6.9 38.5 ± 5.5 ns −0.120 [−0.70, 0.46] RV 4-ch [mm] 36.0 ± 7.5 37.0 ± 5.5 ns −0.035 [−0.54, 0.47] RV axial /LV axial 0.94 ± 0.15 0.99 ± 0.16 ns 0.007 [−0.03, 0.04] RV 4-ch /LV 4-ch 0.93 ± 0.18 0.99 ± 0.24 ns 0.008 [−0.04, 0.05]
Ao, diameter of the ascending aorta; LOBX, lobectomy; LV 4-ch , left ventricular diameter in four-chamber view; LV axial , left ventricular diameter on axial sections; ns, not significant; PA, pulmonary artery diameter; RV 4-ch , right ventricular diameter in four-chamber view; RV axial , right ventricular diameter on axial sections.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
PNX Versus LOBX
Get Radiology Tree app to read full this article<
Table 5
Morphometric Data of Patients Before and After PNX or LOBX
Before Surgery After Surgery PNX LOBX_P_ Value PNX LOBX_P_ Value PA [mm] 28.7 ± 5.4 28.7 ± 3.5 ns 31.1 ± 5.8 30.6 ± 4.3 0.045 PA/Ao 0.86 ± 0.12 0.85 ± 0.10 ns 0.99 ± 0.14 0.90 ± 0.09 0.014 RV axial [mm] 39.4 ± 7.1 38.0 ± 6.9 ns 43.6 ± 7.4 38.5 ± 5.5 0.011 RV 4-ch [mm] 37.6 ± 5.7 36.0 ± 7.5 ns 41.1 ± 6.3 37.0 ± 5.5 0.002 RV axial /LV axial 1.03 ± 0.22 0.94 ± 0.15 ns 1.18 ± 0.27 0.99 ± 0.16 0.003 RV 4-ch /LV 4-ch 1.02 ± 0.16 0.93 ± 0.18 ns 1.17 ± 0.21 0.99 ± 0.24 0.004
Ao, diameter of the ascending aorta; LOBX, lobectomy; LV 4-ch , left ventricular diameter in four-chamber view; LV axial , left ventricular diameter on axial sections; ns, not significant; PA, pulmonary artery diameter; PNX, pneumonectomy; RV 4-ch , right ventricular diameter in four-chamber view; RV axial , right ventricular diameter on axial sections.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Venuta F., Sciomer S., Andreetti C., et. al.: Long-term Doppler echocardiographic evaluation of the right heart after major lung resections. Eur J Cardiothorac Surg 2007; 32: pp. 787-790.
2. Shen K.R., Wain J.C., Wright C.D., et. al.: Postpneumonectomy syndrome: surgical management and long-term results. J Thorac Cardiovasc Surg 2008; 135: pp. 1210-1216. discussion 1216-1219
3. Kim S.Y., Seo J.B., Chae E.J., et. al.: Filling defect in a pulmonary arterial stump on CT after pneumonectomy: radiologic and clinical significance. AJR Am J Roentgenol 2005; 185: pp. 985-988.
4. Ohtaka K., Hida Y., Kaga K., et. al.: Left upper lobectomy can be a risk factor for thrombosis in the pulmonary vein stump. J Cardiothorac Surg 2014; 9: pp. 5.
5. Foroulis C.N., Kotoulas C.S., Kakouros S., et. al.: Study on the late effect of pneumonectomy on right heart pressures using Doppler echocardiography. Eur J Cardiothorac Surg 2004; 26: pp. 508-514.
6. Kalathiya R.J., Saha S.P.: Pneumonectomy for non-small cell lung cancer: outcomes analysis. South Med J 2012; 105: pp. 350-354.
7. Mlczoch J., Zutter W., Keller R., et. al.: Influence of lung resection on pulmonary circulation and lung function at rest and on exercise. Respiration 1975; 32: pp. 424-435.
8. Deslauriers J., Ugalde P., Miro S., et. al.: Long-term physiological consequences of pneumonectomy. Semin Thorac Cardiovasc Surg 2011; 23: pp. 196-202.
9. Potaris K., Athanasiou A., Konstantinou M., et. al.: Pulmonary hypertension after pneumonectomy for lung cancer. Asian Cardiovasc Thorac Ann 2014; 22: pp. 1072-1079.
10. Amar D., Burt M.E., Roistacher N., et. al.: Value of perioperative Doppler echocardiography in patients undergoing major lung resection. Ann Thorac Surg 1996; 61: pp. 516-520.
11. Devaraj A., Wells A.U., Meister M.G., et. al.: The effect of diffuse pulmonary fibrosis on the reliability of CT signs of pulmonary hypertension. Radiology 2008; 249: pp. 1042-1049.
12. Matsushita S., Matsuoka S., Yamashiro T., et. al.: Pulmonary arterial enlargement in patients with acute exacerbation of interstitial pneumonia. Clin Imaging 2014; 38: pp. 454-457.
13. Kwek B.H., Wittram C.: Postpneumonectomy pulmonary artery stump thrombosis: CT features and imaging follow-up. Radiology 2005; 237: pp. 338-341.
14. Kang D.K., Ramos-Duran L., Schoepf U.J., et. al.: Reproducibility of CT signs of right ventricular dysfunction in acute pulmonary embolism. AJR Am J Roentgenol 2010; 194: pp. 1500-1506.
15. Edwards P.D., Bull R.K., Coulden R.: CT measurement of main pulmonary artery diameter. Br J Radiol 1998; 71: pp. 1018-1020.
16. Kuriyama K., Gamsu G., Stern R.G., et. al.: CT-determined pulmonary artery diameters in predicting pulmonary hypertension. Invest Radiol 1984; 19: pp. 16-22.
17. Mahammedi A., Oshmyansky A., Hassoun P.M., et. al.: Pulmonary artery measurements in pulmonary hypertension: the role of computed tomography. J Thorac Imaging 2013; 28: pp. 96-103.
18. Ng C.S., Wells A.U., Padley S.P.: A CT sign of chronic pulmonary arterial hypertension: the ratio of main pulmonary artery to aortic diameter. J Thorac Imaging 1999; 14: pp. 270-278.
19. Okada M., Ota T., Okada M., et. al.: Right ventricular dysfunction after major pulmonary resection. J Thorac Cardiovasc Surg 1994; 108: pp. 503-511.
20. Reed C.E., Spinale F.G., Crawford F.A.: Effect of pulmonary resection on right ventricular function. Ann Thorac Surg 1992; 53: pp. 578-582.
21. Hsia C.C., Carlin J.I., Cassidy S.S., et. al.: Hemodynamic changes after pneumonectomy in the exercising foxhound. J Appl Physiol 1990; 69: pp. 51-57.
22. Kocaturk M., Salci H., Yilmaz Z., et. al.: Pre- and post-operative cardiac evaluation of dogs undergoing lobectomy and pneumonectomy. J Vet Sci 2010; 11: pp. 257-264.
23. Kang D.K., Thilo C., Schoepf U.J., et. al.: CT signs of right ventricular dysfunction: prognostic role in acute pulmonary embolism. JACC Cardiovasc Imaging 2011; 4: pp. 841-849.
24. Becattini C., Agnelli G., Germini F., et. al.: Computed tomography to assess risk of death in acute pulmonary embolism: a meta-analysis. Eur Respir J 2014; 43: pp. 1678-1690.
25. Hatz R.A., Klotz L.V.: [Consequences of pneumonectomy in the early and late phases]. Article in German Chirurg 2013; 84: pp. 497-501.
26. Lin F.Y., Devereux R.B., Roman M.J., et. al.: Cardiac chamber volumes, function, and mass as determined by 64-multidetector row computed tomography: mean values among healthy adults free of hypertension and obesity. JACC Cardiovasc Imaging 2008; 1: pp. 782-786.
27. Lee K.S., Sista A.K., Friedman O.A., et. al.: Successful catheter-directed thrombolysis of a massive pulmonary embolism in a patient after recent pneumonectomy. Clin Imaging 2015; 39: pp. 140-143.
28. Ohtaka K., Hida Y., Kaga K., et. al.: Thrombosis in the pulmonary vein stump after left upper lobectomy as a possible cause of cerebral infarction. Ann Thorac Surg 2013; 95: pp. 1924-1928.
29. Colt H.G., Murgu S.D., Korst R.J., et. al.: Follow-up and surveillance of the patient with lung cancer after curative-intent therapy: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013; 143: pp. e437S-e454S.
30. Pedoto A., Amar D.: Right heart function in thoracic surgery: role of echocardiography. Curr Opin Anaesthesiol 2009; 22: pp. 44-49.
31. Dogan H., Kroft L.J., Huisman M.V., et. al.: Right ventricular function in patients with acute pulmonary embolism: analysis with electrocardiography-synchronized multi-detector row CT. Radiology 2007; 242: pp. 78-84.
32. Lu M.T., Cai T., Ersoy H., et. al.: Comparison of ECG-gated versus non-gated CT ventricular measurements in thirty patients with acute pulmonary embolism. Int J Cardiovasc Imaging 2009; 25: pp. 101-107.
33. Bach A.G., Nansalmaa B., Kranz J., et. al.: CT pulmonary angiography findings that predict 30-day mortality in patients with acute pulmonary embolism. Eur J Radiol 2015; 84: pp. 332-337.
34. Liu M., Ma Z.H., Guo X.J., et. al.: A septal angle measured on computed tomographic pulmonary angiography can noninvasively estimate pulmonary vascular resistance in patients with chronic thromboembolic pulmonary hypertension. J Thorac Imaging 2012; 27: pp. 325-330.