
Rationale and Objectives
Cavernous malformations (cavernomas) occur in 0.4%–0.9% of the population. The most common symptoms of cavernous malformations are seizures. An improved detection of small cavernomas might possibly help to clarify cryptogenic seizures, which represent 30% of all seizures. The aim of this study was to evaluate the benefit of magnetic resonance imaging at a field strength of 7 T in the detection of cavernomas.
Materials and Methods
Ten consecutive patients with known cavernomas were enrolled in this study. First a T2∗-weighted gradient echo sequence was performed at 1.5 T with a slice thickness of 6 mm in axial orientation. Subsequently, the examination was repeated at 7 T. Both examinations were independently read by two blinded senior neuroradiologists. Localization and dimension of the hypointensities were recorded.
Results
One additional hypointensity was detected in one patient, which was not visible in the 1.5 T examination even retrospectively. In another patient with known cavernomatosis, innumerable new small hypointense lesions were detected at 7 T.
Conclusion
Our small series suggests that ultra–high-field magnetic resonance imaging at 7 T improves the detection of cavernomas.
Cavernous malformations (cavernomas) occur in 0.4%–0.9% of the population and represent 8%–15% of all vascular malformations . It is not a neoplastic tumour but a nonmalignant vascular hamartoma with close-packed malformed blood vessels exhibiting endothelial proliferation and neoangiogenesis . The bleeding risk of cavernomas is 0.27%–0.7% per year. Such hemorrhages are usually the cause of symptoms in the patients. Blood breakdown products have high epileptogenic potential; consequently, seizures are the most common symptom of cavernomas . Because of the various ages of the hemorrhages, cavernomas often have a popcorn-like pattern with a hypointense ring of hemosiderin in T2∗-weighted magnetic resonance images (MRIs). Dependent on the different stages of a hemorrhage, the T1 signal varies between hypo- and hyperintense . The occurrence of multiple cavernomas in one patient is mostly genetically determined , but might also be a result of radiation therapy .
Nowadays, the clarification of the etiology of seizures is based on electroencephalogram and MRI mostly at 1.5Tesla (T). With this approach, 30% of all seizures remain cryptogenic. An improved detection of cavernomas might possibly help to clarify cryptogenic seizures, which might be caused by cavernomas not detectable at 1.5 T. This could lead to a surgical therapy. With the recent implementation of 7 T MRI systems for ultra–high-field MRIs of humans, researchers have examined the advantages and limitations of this field strength for various imaging applications . One major advantage of ultra–high-field MRI is the potentially higher achievable overall signal-to-noise ratio. In addition to the theoretically four- to fivefold higher signal-to-noise ratio at 7 T compared with that at 1.5 T, the sensitivity to tissue susceptibility differences also increases linearly with field strength and theoretically should lead to improved susceptibility artefacts. This could lead to a higher sensitivity in detecting lesions such as cavernomas in T2∗-weighted images .
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Clinical Data of the 10 Patients
Subject Age Gender Symptom Localization 1.5 T, Diameter (mm) Localization 7 T, Diameter (mm) 1 37 F Paresis of left oculomotor and facial nerve Midbrain tegmentum (10) Midbrain tegmentum (10) 2 59 F Seizures Left frontal lobe (14) Left frontal lobe (16) 3 46 M Ataxia Medulla oblongata (15) Medulla oblongata (15) 4 34 F Asymptomatic, incidental finding Brainstem (4) Brainstem (6) 5 24 F Headache Left parietal lobe (7) Left parietal lobe (10) 6 30 F Seizures Right basal ganglia (9)
Right thalamus (26 × 8)
Left thalamus (17 × 20)
Left temporal lobe (6)
Brainstem (3) Right basal ganglia (11)
Right thalamus (28 × 9)
Left thalamus (14 × 25)
Left temporal lobe (6)
Brainstem (5)
Right frontal lobe (4) 7 41 M Dysarthria, dysphagia Medulla oblongata (10) Medulla oblongata (11) 8 52 M Seizures Cavernomatosis Cavernomatosis 9 32 M Seizures Left frontotemporal lobe (18) Left frontotemporal lobe (18) 10 35 M Seizures Left parietal lobe (19) Left parietal lobe (21)
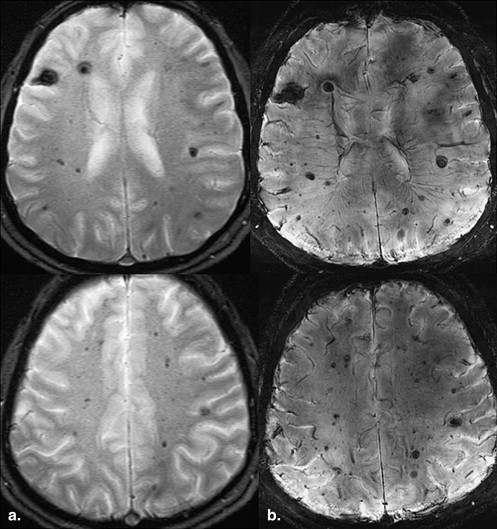
One additional cavernoma was found at 7 T in Subject 6 ( italic ). In Subject 8 with known cavernomatosis, many additional small lesions were detected at 7 T ( Figure 1 ). Sizes of the cavernomas at 7 T were equal or larger than at 1.5 T. The sizes given are the means of the sizes determined by the two independent readers.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Bertalanffy H., Benes L., Miyazawa T., et. al.: Cerebral cavernomas in the adult. Review of the literature and analysis of 72 surgically treated patients. Neurosurg Rev 2002; 25: pp. 1-53. discussion 4–5
2. Sure U., Freman S., Bozinov O., et. al.: Biological activity of adult cavernous malformations: a study of 56 patients. J Neurosurg 2005; 102: pp. 342-347.
3. Ahlhelm F., Hagen T., Schulte-Altedorneburg G., et. al.: Cavernous malformations. Radiologe 2007; 47: pp. 863-867.
4. Felbor U., Gaetzner S., Verlaan D.J., et. al.: Large germline deletions and duplication in isolated cerebral cavernous malformation patients. Neurogenetics 2007; 8: pp. 149-153.
5. Heckl S., Aschoff A., Kunze S.: Radiation-induced cavernous hemangiomas of the brain: a late effect predominantly in children. Cancer 2002; 94: pp. 3285-3291.
6. Huang C.W., Hsieh Y.J., Tsai J.J., et. al.: Cognitive performance in cryptogenic epilepsy. Acta Neurol Scand 2005; 112: pp. 228-233.
7. Ladd M.E.: High-field-strength magnetic resonance: potential and limits. Top Magn Reson Imaging 2007; 18: pp. 139-152.
8. Santhosh K., Kesavadas C., Thomas B., et. al.: Susceptibility weighted imaging: a new tool in magnetic resonance imaging of stroke. Clin Radiol 2009; 64: pp. 74-83.
9. Ryvlin P., Mauguiere F., Sindou M., et. al.: Interictal cerebral metabolism and epilepsy in cavernous angiomas. Brain 1995; 118: pp. 677-687.
10. Stefan H., Hammen T.: Cavernous haemangiomas, epilepsy and treatment strategies. Acta Neurol Scand 2004; 110: pp. 393-397.
11. Kollia K., Maderwald S., Putzki N., et. al.: First clinical study on ultra-high-field MR imaging in patients with multiple sclerosis: comparison of 1.5 T and 7 T. AJNR Am J Neuroradiol 2009; 30: pp. 699-702.
12. Monninghoff C., Maderwald S., Theysohn J.M., et. al.: Evaluation of intracranial aneurysms with 7 T versus 1.5 T time-of-flight MR angiography—initial experience. Rofo 2009; 181: pp. 16-23.
13. Novak V., Chowdhary A., Abduljalil A., et. al.: Venous cavernoma at 8 Tesla MRI. Magn Reson Imaging 2003; 21: pp. 1087-1089.
14. Pinker K., Stavrou I., Szomolanyi P., et. al.: Improved preoperative evaluation of cerebral cavernomas by high-field, high-resolution susceptibility-weighted magnetic resonance imaging at 3 Tesla: comparison with standard (1.5 T) magnetic resonance imaging and correlation with histopathological findings—preliminary results. Invest Radiol 2007; 42: pp. 346-351.
15. Theysohn J.M., Kraff O., Maderwald S., et. al.: The human hippocampus at 7 T—in vivo MRI. Hippocampus 2009; 19: pp. 1-7.