
Rationale and Objectives
The aim of this study was to determine the efficacy of hyperpolarized 3 He (HHe) ventilation and apparent diffusion coefficient (ADC) HHe magnetic resonance imaging (MRI) in detecting changes in lung function and microstructure in emphysematous lung after bronchial valve (BV) placement.
Materials and Methods
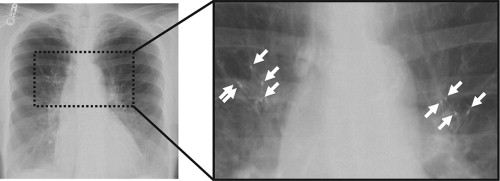
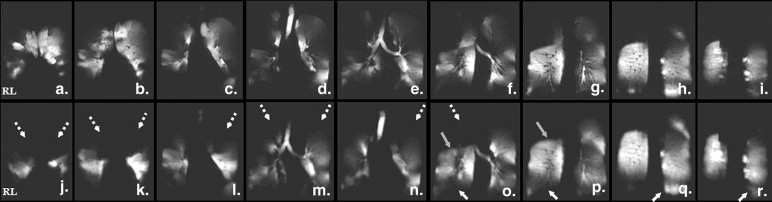
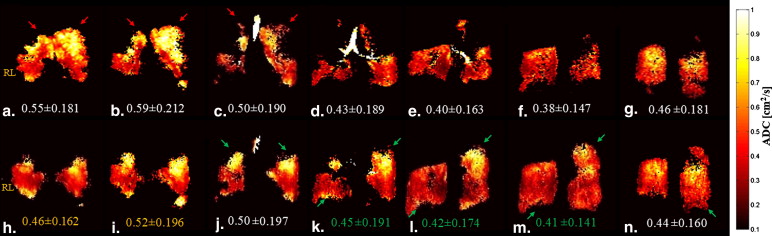
One patient diagnosed with emphysema had nine BVs placed in upper lobe bronchi. Imaging was performed before and 6 months after BV placement. Coronal HHe ventilation MRI was used to assess volume changes in the ventilated portions of the lung. Coronal ADC HHe MRI, acquired with b value pairs of 0 and 1.6 s/cm 2 during a second 10-second breath-hold, was used to compute ADC values.
Results
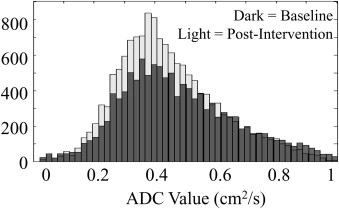
HHe ventilation MRI revealed decreased ventilation in the treated segments of the upper lobes after BV placement. Increased ventilation in the lower lobes and two untreated segments of the left upper lobes were also observed, with an upward shift of the major fissure of the right lung. Whole-lung mean ADC decreased by 6.3% from baseline, from 0.48 ± 0.196 to 0.45 ± 0.176 cm 2 /s (toward healthier values) following BV placement.
Conclusions
HHe ventilation MRI detected an increase in whole-lung volume and an interlobar fissure shift indicative of increased ventilation of lower relative to upper lobes. Reduced ADC values suggest increased ventilation to healthy lower lobes at the expense of more diseased, expanded alveolar spaces in the upper lobes distal to BV placement. These results suggest that this ionizing radiation–free method of examining the lungs may offer functional and structural information useful in BV intervention planning.
Chronic obstructive pulmonary disease (COPD) is a disease state characterized by chronic airflow limitation due to chronic bronchitis and emphysema, a condition marked by the progressive destruction of the alveolar walls and subsequent enlargement of the airspace. Although the upper lobes are usually the first affected, there is considerable variability in the location and degree of emphysema. Emphysematous changes lead to a decrease in lung ventilation as air becomes entrapped within afflicted lung regions and are the cause of dyspnea, exercise impairment, and a reduced quality of life . In 2005, emphysema was deemed primarily responsible for the deaths of >14,000 Americans , and it is estimated that >2 million people in the United States alone are currently affected by this disease . Lung volume reduction surgery with surgical removal of the nonfunctioning, hyperinflated areas has been shown to be effective in patients whose emphysema predominantly involved the upper lobes; however, the procedure is highly invasive and is associated with high morbidity (20%–30%) and mortality (7.6%) rates within 90 days after surgery .
New, less invasive bronchoscopic approaches to treat COPD have been tested in the past decade and are currently under investigation . These new procedures involve a variety of different devices (eg, bronchial blockers, bronchial sealants, one-way bronchial valves [BVs]), but their basic concept is the reduction of ventilation to the areas with the most severe emphysema, which, if atelectasis occurs, is conceptually similar to the volume loss created by lung volume reduction surgery but with a much less invasive procedure. The IBV Valve (Spiration, Inc, Redmond, WA), which is currently undergoing phase III clinical trials in the United States, is one such device for the minimally invasive treatment of patients with severe emphysema. This small one-way BV can be placed during a single bronchoscopic procedure in selected bronchi. The BV can induce atelectasis , but investigations using quantitative computed tomography have shown that the most common mechanism associated with significant improvement in quality of life was a redirection of airflow to nontreated regions of the lung . Currently, multiple valves are placed bilaterally in upper lobe bronchi in patients with upper lobe–predominant emphysema . Although the upper lobes are commonly the first area to be affected, there is considerable variability in the location and degree of emphysema. The development of a clinical imaging modality that can generate high-resolution, three-dimensional functional maps of the lung without the use of ionizing radiation could provide a more targeted approach to valve placement, which could improve effectiveness.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Barnes P.J.: Chronic obstructive pulmonary disease. N Engl J Med 2000; 343: pp. 269-280.
2. Kung H.C., Hoyert D.L., Xu J., et. al.: Deaths: final data for 2005. Natl Vital Stat Rep 2008; 56: pp. 1-120.
3. Venuta F., Rendina E.A., De Giacomo T., et. al.: Bronchoscopic procedures for emphysema treatment. Eur J Cardiothorac Surg 2006; 29: pp. 281-287.
4. Coxson H.O., Nasute Fauerbach P.V., Storness-Bliss C., et. al.: Computed tomography assessment of lung volume changes after bronchial valve treatment. Eur Respir J 2008; 32: pp. 1443-1450.
5. Fishman A., Martinez F., Naunheim K., et. al.: A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med 2003; 348: pp. 2059-2073.
6. Naunheim K.S., Wood D.E., Krasna M.J., et. al.: Predictors of operative mortality and cardiopulmonary morbidity in the National Emphysema Treatment Trial. J Thorac Cardiovasc Surg 2006; 131: pp. 43-53.
7. Maxfield R.A.: New and emerging minimally invasive techniques for lung volume reduction. Chest 2004; 125: pp. 777-783.
8. Springmeyer S.C., Bolliger C.T., Waddell T.K., et. al., IBV Valve Pilot Trials Research Teams: Treatment of heterogeneous emphysema using the Spiration IBV valves. Thorac Surg Clin 2009; 19: pp. 247-253.
9. Sterman D.H., Mehta A.C., Wood D.E., et. al.: A multicenter pilot study of a bronchial valve for the treatment of severe emphysema. Respiration 2010; 79: pp. 222-233.
10. Mata J.F., Altes T.A., Cai J., et. al.: Evaluation of emphysema severity and progression in a rabbit model: comparison of hyperpolarized 3He and 129Xe diffusion MRI with lung morphometry. J Appl Physiol 2007; 102: pp. 1273-1280.
11. Salerno M., de Lange E.E., Altes T.A., et. al.: Emphysema: hyperpolarized helium 3 diffusion MR imaging of the lungs compared with spirometric indexes—initial experience. Radiology 2002; 222: pp. 252-260.
12. Mata J.: Hyperpolarized Gas MRI to Evaluate Emphysema—A New Biomarker with High Sensitivity.2008.VDM VerlagBerlin, Germany
13. Wood D.E., McKenna R.J., Yusen R.D., et. al.: A multicenter trial of an intrabronchial valve for treatment of severe emphysema. J Thorac Cardiovasc Surg 2007; 133: pp. 65-73.
14. Middleton H., Black R.D., Saam B., et. al.: MR imaging with hyperpolarized 3He gas. Magn Reson Med 1995; 33: pp. 271-275.
15. Black R.D., Middleton H.L., Cates G.D., et. al.: In vivo He-3 MR images of guinea pig lungs. Radiology 1996; 199: pp. 867-870.
16. Herpel L.B., Kanner R.E., Lee S.M., et. al.: Variability of spirometry in chronic obstructive pulmonary disease: results from two clinical trials. Am J Respir Crit Care Med 2006; 173: pp. 1106-1113.
17. Takasugi J.E., Godwin J.D.: Radiology of chronic obstructive pulmonary disease. Radiol Clin North Am 1998; 36: pp. 29-55.
18. Mata J.F., Altes T.A., Ruppert K., et. al.: Assessment of in vitro vs. in vivo lung structure using hyperpolarized helium-3 diffusion magnetic resonance imaging. Magn Reson Imaging 2009; 27: pp. 845-851.
19. Gierada D.S., Woods J.C., Bierhals A.J., et. al.: Effects of diffusion time on short-range hyperpolarized (3)He diffusivity measurements in emphysema. J Magn Reson Imaging 2009; 30: pp. 801-808.
20. Kilian W., Seifert F., Rinneberg H.: Dynamic NMR spectroscopy of hyperpolarized (129)Xe in human brain analyzed by an uptake model. Magn Reson Med 2004; 51: pp. 843-847.
21. Ruppert K., Brookeman J.R., Hagspiel K.D., et. al.: NMR of hyperpolarized (129)Xe in the canine chest: spectral dynamics during a breath-hold. NMR Biomed 2000; 13: pp. 220-228.
22. Kauczor H.U., Chen X.J., van Beek E.J., et. al.: Pulmonary ventilation imaged by magnetic resonance: at the doorstep of clinical application. Eur Respir J 2001; 17: pp. 1008-1023.