
Rationale and Objectives
This study aimed to compare Breast Imaging Reporting and Data System (BI-RADS) assessment of lesions in two-view digital mammogram (DM) to two-view wide-angle digital breast tomosynthesis (DBT) without DM.
Materials and Methods
With Institutional Review Board approval and written informed consent, two-view DBTs were acquired from 134 subjects and the corresponding DMs were collected retrospectively. The study included 125 subjects with 61 malignant (size: 3.9–36.9 mm, median: 13.4 mm) and 81 benign lesions (size: 4.8–43.8 mm, median: 12.0 mm), and 9 normal subjects. The cases in the two modalities were read independently by six experienced Mammography Quality Standards Act radiologists in a fully crossed counterbalanced manner. The readers were blinded to the prevalence of malignant, benign, or normal cases and were asked to assess the lesions based on the BI-RADS lexicon. The ratings were analyzed by the receiver operating characteristic methodology.
Results
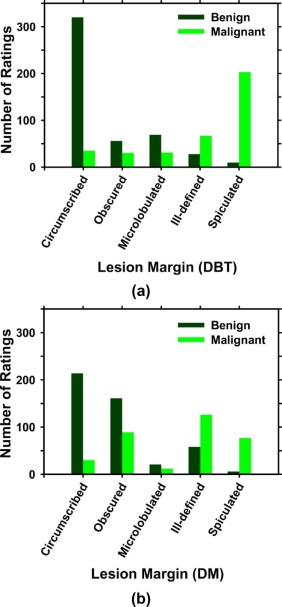
Lesion conspicuity was significantly higher ( P « .0001) and fewer lesion margins were considered obscured in DBT. The mean area under the receiver operating characteristic curve for the six readers increased significantly ( P = .0001) from 0.783 (range: 0.723–0.886) for DM to 0.911 (range: 0.884–0.936) for DBT. Of the 366 ratings for malignant lesions, 343 on DBT and 278 on DM were rated as BI-RADS 4a and above. Of the 486 ratings for benign lesions, 220 on DBT and 206 on DM were rated as BI-RADS 4a and above. On average, 17.8% (65 of 366) more malignant lesions and 2.9% (14 of 486) more benign lesions would be recommended for biopsy using DBT. The inter-radiologist variability was reduced significantly.
Conclusion
With DBT alone, the BI-RADS assessment of breast lesions and inter-radiologist reliability were significantly improved compared to DM.
Introduction
Digital breast tomosynthesis (DBT) is increasingly being used in breast imaging clinics. Three commercial DBT systems have been approved by the Food and Drug Administration for screening and diagnostic workup, and more systems are available outside the United States. The three systems have different designs of scan parameters ranging from 15° to 50°. The screening protocols for the systems also differ; one system was approved for a combination mode (combo mode) that includes two-view DBT in combination with two-view digital mammograms (DMs), the second system was approved for a craniocaudal (CC) view DM with a mediolateral oblique (MLO) view DBT, and the third system was approved for a stand-alone two-view DBT. A number of prospective or observational studies of clinical performance before and after implementation of DBT have been conducted to compare the combo mode with DM alone in screening settings. All these studies found significant improvement in cancer detection rate and a reduction in the overall recall rate or a reduction in the recall rate per cancer detected. Other investigators have conducted retrospective reader studies as reviewed in References ; most of these studies also revealed the potential of the combo mode, yielding higher cancer detection rate and lower recall rate compared to DM alone.
The vast majority of the studies to date evaluated DBT as an adjunct to DM using DBT systems with a scan angle of 15°. A few studies evaluated DBT systems with larger scan angles (40°–50°) , in which an MLO-view DBT replaced the MLO-view DM or both views of DM. The results from the studies using different modes other than the combo mode are more varied. The DM in the combo mode is also being replaced with a mammogram-like image synthesized from DBT to reduce dose, and the adequacy of such approach is being investigated. DBT is still an evolving technology, and its capability and limitations have not been fully explored, especially its performance for scan angles other than 15° and as a stand-alone modality. Continued development and studies of the impact of DBT acquisition geometry (scan angle, number of projections) and other factors on the performance of DBT are crucial to further improve its efficacy in both screening and diagnostic applications.
Get Radiology Tree app to read full this article<
Materials and Methods
Data Set
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Pathology of the Malignant or Benign Lesions Included in the Study
Lesion Type Pathology Number Benign Fibroadenoma 43 Fibrocystic change 8 Fat necrosis 2 Lymph node 2 Usual intraductal hyperplasia 4 Atypical ductal hyperplasia and atypical lobular hyperplasia 1 Pseudoangiomatous stromal hyperplasia 1 Cyst 11 Hematoma 2 Benign tissue 7 Malignant Invasive ductal carcinoma 31 \* Invasive lobular carcinoma 12 \* Invasive carcinoma with ductal and lobular features 14 \* Adenocarcinoma 1 Invasive tubular carcinoma 1 Mucosa-associated lymphoid tissue (MALT) lymphoma 2
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Observer Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
participated as readers. At the time of the study, the six radiologists had 6–37 years (median 20 years) of experience in mammography; they had not interpreted DBT in clinical settings but four had experience in reading human subject DBT (different from those in the current data set) for previous research projects.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
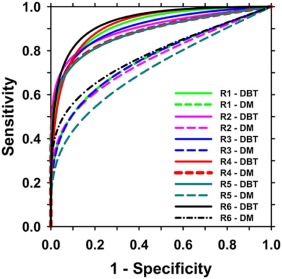
TABLE 2
Areas Under the ROC Curves for the Six Radiologists Reading the Two Modalities (DBT, DM) and Rating the Degree of Suspicion by BI-RADS Assessment Categories (1, 2, 3, 4a, 4b, 4c, 5)
Reader Area Under the ROC Curve DBT DM Difference (DBT − DM)P Value R1 0.916 0.769 0.147 .0018 R2 0.902 0.762 0.140 .0003 R3 0.906 0.770 0.137 .0011 R4 0.923 0.886 0.037 .2567 R5 0.884 0.723 0.160 .0003 R6 0.936 0.787 0.149 <.0001 Mean 0.911 0.783 0.129 Standard deviation 0.020 0.034 95% Confidence interval (0.069, 0.188)P value .0001
DBT, digital breast tomosynthesis; DM, digital mammogram; ROC, receiver operating characteristic.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
The BI-RADS Assessments by the Six Radiologists in the Two Modalities (DBT, DM) for Malignant or Benign Lesions Grouped Into Three Types (Architectural Distortion, Asymmetry, and Mass) Based on Their Appearance on DM
Ratings DBT DM Change (DBT − DM) Malignant Benign Malignant Benign Malignant Benign BI-RADS 3 and below Architectural distortion 1 0 22 1 −21 −1 Asymmetry 8 59 36 57 −28 +2 Mass 14 207 30 222 −16 −15 Total 23 266 88 280 −65 −14 BI-RADS 4a and above Architectural distortion 77 6 56 5 +21 +1 Asymmetry 94 31 66 33 +28 −2 Mass 172 183 156 168 +16 +15 Total 343 220 278 206 +65 +14
Classification Sensitivity Specificity Sensitivity Specificity Percentage Change Percentage Change 93.7% (343/366) 54.7% (266/486) 76.0% (278/366) 57.6% (280/486) +17.8% (65/366) −2.9% (14/486)
BI-RADS, Breast Imaging Reporting and Data System; DBT, digital breast tomosynthesis; DM, digital mammogram; ROC, receiver operating characteristic.
The number of lesions in each type can be found in Table 4 . The total number of ratings was 366 (61 × 6) for malignant lesions and 486 (81 × 6) for benign lesions. The sensitivity and specificity for the classification of malignancy are determined with a decision threshold of BI-RADS 4a and above. For malignant lesions, positive change to BI-RADS 4a and above is desirable. For benign lesions, positive change to BI-RADS 4a and above is undesirable.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
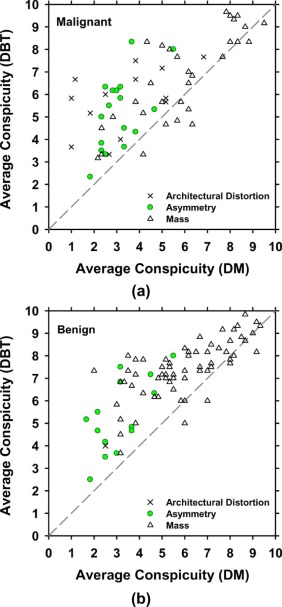
TABLE 4
Mean Conspicuity Ratings of the Three Types of Lesions: Architectural Distortion, Asymmetry, and Mass, Averaged Over the Six Radiologists in the Two Modalities
Malignant Mean Conspicuity Benign Mean Conspicuity_N_ DBT DM_P_ Value_N_ DBT DM_P_ Value Architectural distortion 13 5.8 3.3 .0002 1 4.0 2.5 — Asymmetry 17 5.2 3.1 .00001 15 5.4 3.3 .00001 Mass 31 6.7 5.9 .0011 65 7.4 5.9 «.0001 Total 61 6.1 4.6 «.0001 81 7.0 5.4 «.0001
DBT, digital breast tomosynthesis; DM, digital mammogram; N , number.
The conspicuities in DBT are significantly higher than those in DM for all types of lesions with P values from two-tailed paired t test much smaller than 0.05. Rating scale: 1–10, 10 = most conspicuous.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Skaane P., Bandos A.I., Gullien R., et. al.: Prospective trial comparing full-field digital mammography (FFDM) versus combined FFDM and tomosynthesis in a population-based screening programme using independent double reading with arbitration. Eur Radiol 2013; 23: pp. 2061-2071.
2. Skaane P., Bandos A.I., Gullien R., et. al.: Comparison of digital mammography alone and digital mammography plus tomosynthesis in a population-based screening program. Radiology 2013; 267: pp. 47-56.
3. Ciatto S., Houssami N., Bernardi D., et. al.: Integration of 3D digital mammography with tomosynthesis for population breast-cancer screening (STORM): a prospective comparison study. Lancet Oncol 2013; 14: pp. 583-589.
4. Rose S.L., Tidwell A.L., Bujnoch L.J., et. al.: Implementation of breast tomosynthesis in a routine screening practice: an observational study. Am J Roentgenol 2013; 200: pp. 1401-1408.
5. Friedewald S.M., Rafferty E.A., Rose S.L., et. al.: Breast cancer screening using tomosynthesis in combination with digital mammography. JAMA 2014; 311: pp. 2499-2507.
6. Greenberg J.S., Javitt M.C., Katzen J., et. al.: Clinical performance metrics of 3D digital breast tomosynthesis compared with 2D digital mammography for breast cancer screening in community practice. Am J Roentgenol 2014; 203: pp. 687-693.
7. Durand M.A., Haas B.M., Yao X.P., et. al.: Early clinical experience with digital breast tomosynthesis for screening mammography. Radiology 2015; 274: pp. 85-92.
8. Sharpe R.E., Venkataraman S., Phillips J., et. al.: Increased cancer detection rate and variations in the recall rate resulting from implementation of 3D digital breast tomosynthesis into a population-based screening program. Radiology 2016; 278: pp. 698-706.
9. Bernardi D., Macaskill P., Pellegrini M., et. al.: Breast cancer screening with tomosynthesis (3D mammography) with acquired or synthetic 2D mammography compared with 2D mammography alone (STORM-2): a population-based prospective study. Lancet Oncol 2016; 17: pp. 1105-1113.
10. Conant E.F., Beaber E.F., Sprague B.L., et. al.: Breast cancer screening using tomosynthesis in combination with digital mammography compared to digital mammography alone: a cohort study within the PROSPR consortium. Breast Cancer Res Treat 2016; 156: pp. 109-116.
11. Gilbert F.J., Tucker L., Young K.C.: Digital breast tomosynthesis (DBT): a review of the evidence for use as a screening tool. Clin Radiol 2016; 71: pp. 141-150.
12. Hodgson R., Heywang-Kobrunner S.H., Harvey S.C., et. al.: Systematic review of 3D mammography for breast cancer screening. Breast 2016; 27: pp. 52-61.
13. Andersson I., Ikeda D.M., Zackrisson S., et. al.: Breast tomosynthesis and digital mammography: a comparison of breast cancer visibility and BIRADS classification in a population of cancers with subtle mammographic findings. Eur Radiol 2008; 18: pp. 2817-2825.
14. Gennaro G., Toledano A., di Maggio C., et. al.: Digital breast tomosynthesis versus digital mammography: a clinical performance study. Eur Radiol 2010; 20: pp. 1545-1553.
15. Svahn T.M., Chakraborty D.P., Ikeda D., et. al.: Breast tomosynthesis and digital mammography: a comparison of diagnostic accuracy. Br J Radiol 2012; 85: pp. E1074-E1082.
16. Gennaro G., Hendrick R.E., Toledano A., et. al.: Combination of one-view digital breast tomosynthesis with one-view digital mammography versus standard two-view digital mammography: per lesion analysis. Eur Radiol 2013; 23: pp. 2087-2094.
17. Thibault F., Dromain C., Breucq C., et. al.: Digital breast tomosynthesis versus mammography and breast ultrasound: a multireader performance study. Eur Radiol 2013; 23: pp. 2441-2449.
18. Lang K., Andersson I., Rosso A., et. al.: Performance of one-view breast tomosynthesis as a stand-alone breast cancer screening modality: results from the Malmo breast tomosynthesis screening trial, a population-based study. Eur Radiol 2016; 26: pp. 184-190.
19. Dorfman D.D., Berbaum K.S., Metz C.E.: ROC rating analysis: generalization to the population of readers and cases with the jackknife method. Invest Radiol 1992; 27: pp. 723-731.
20. Metz C.E.: Some practical issues of experimental design and data analysis in radiological ROC studies. Invest Radiol 1989; 24: pp. 234-245.
21. Mariscotti G., Durando M., Houssami N., et. al.: Digital breast tomosynthesis as an adjunct to digital mammography for detecting and characterising invasive lobular cancers: a multi-reader study. Clin Radiol 2016; 71: pp. 889-895.
22. Thomassin-Naggara I., Perrot N., Dechoux S., et. al.: Added value of one-view breast tomosynthesis combined with digital mammography according to reader experience. Eur J Radiol 2015; 84: pp. 235-241.
23. Waldherr C., Cerny P., Altermatt H.J., et. al.: Value of one-view breast tomosynthesis versus two-view mammography in diagnostic workup of women with clinical signs and symptoms and in women recalled from screening. Am J Roentgenol 2013; 200: pp. 226-231.
24. Wallis M.G., Moa E., Zanca F., et. al.: Two-view and single-view tomosynthesis versus full-field digital mammography: high-resolution X-ray imaging observer study. Radiology 2012; 262: pp. 788-796.
25. Teertstra H.J., Loo C.E., van den Bosch M.A.A.J., et. al.: Breast tomosynthesis in clinical practice: initial results. Eur Radiol 2010; 20: pp. 16-24.
26. Gur D., Abrams G.S., Chough D.M., et. al.: Digital breast tomosynthesis: observer performance study. Am J Roentgenol 2009; 193: pp. 586-591.
27. Poplack S.P., Tosteson T.D., Kogel C.A., et. al.: Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screening mammography. Am J Roentgenol 2007; 189: pp. 616-623.
28. Spangler M.L., Zuley M.L., Sumkin J.H., et. al.: Detection and classification of calcifications on digital breast tomosynthesis and 2D digital mammography: a comparison. Am J Roentgenol 2011; 196: pp. 320-324.
29. Kopans D., Gavenonis S., Halpern E., et. al.: Calcifications in the breast and digital breast tomosynthesis. Breast J 2011; 17: pp. 638-644.
30. Tagliafico A., Mariscotti G., Durando M., et. al.: Characterisation of microcalcification clusters on 2D digital mammography (FFDM) and digital breast tomosynthesis (DBT): does DBT underestimate microcalcification clusters? Results of a multicentre study. Eur Radiol 2015; 25: pp. 9-14.
31. Clauser P., Nagl G., Helbich T.H., et. al.: Diagnostic performance of digital breast tomosynthesis with a wide scan angle compared to full-field digital mammography for the detection and characterization of microcalcifications. Eur J Radiol 2016; 86: pp. 2161-2168.