
Rationale and Objectives
Pulmonary involvement in inflammatory bowel disease may reflect the common embryonic origin of the gastrointestinal tract and the bronchial tree. No studies have compared pulmonary high-resolution computed tomography (HRCT) findings between ulcerative colitis (UC) and Crohn disease (CD). This study aimed to assess the relationship between pulmonary HRCT findings and inflammatory bowel disease activity and to compare HRCT findings between UC and CD.
Materials and Methods
We retrospectively identified 601 consecutive patients (350 with UC and 251 with CD) who had undergone chest HRCT examinations at our institutions between April 2004 and April 2016. Parenchymal abnormalities, enlarged lymph nodes, and pleural effusion were evaluated on HRCT.
Results
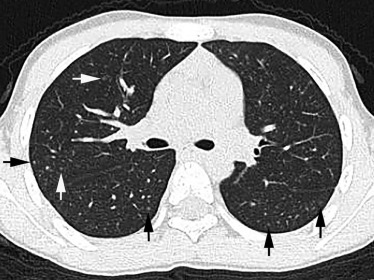
One hundred sixty-seven patients (94 men, 73 women; aged 12–86 years, mean: 47.2 years) with UC and 93 patients (61 men, 32 women; aged 12–71 years, mean: 37.9 years) with CD had abnormal findings on chest HRCT. The HRCT findings of UC and CD mainly consisted of centrilobular nodules (in 49.1% and 45.2% of cases, respectively) and bronchial wall thickening (in 31.7% and 54.8%, respectively). There was no relationship between HRCT findings and disease activity. Bronchial wall thickening was significantly more frequent in patients with CD than in those with UC ( P < .001).
Conclusion
The main chest HRCT findings in UC and CD are centrilobular nodules and bronchial wall thickening. There are differences in HRCT findings between UC and CD.
Introduction
The inflammatory bowel diseases (IBDs) (Crohn disease [CD] and ulcerative colitis [UC]) are widely recognized disorders of the gastrointestinal tract that may have a variety of extraintestinal manifestations. These manifestations include pyoderma gangrenosum, erythema nodosum, arthritis, uveitis, and various types of pulmonary disease . Colonic and respiratory epithelia share an embryonic origin from the primitive foregut. Unexplained bronchopulmonary disease was first reported in six patients with IBD in 1976 . Pulmonary involvement in IBD has since been recognized with increasing frequency in the literature.
There have been several reports of pulmonary computed tomography (CT) findings in patients with IBD. However, only nine English-language studies have used high-resolution CT (HRCT) to evaluate these findings. Tunc et al. investigated associations between chest HRCT findings and IBD activity in 52 patients with IBD . They found that 50% of patients with UC and 60% of patients with CD had abnormal chest HRCT findings and that these abnormalities were not significantly different between UC and CD. Yilmaz et al. reported that IBD activity was not correlated with chest HRCT findings in 39 patients .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Examinations
Get Radiology Tree app to read full this article<
CT Image Interpretation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Patients’ Characteristics
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics
Characteristics Ulcerative Colitis ( n = 167) Crohn Disease ( n = 93) M, F 94, 73 61, 32 Age (y) Range 12-86 13-71 Mean 47.2 37.9 Smoking Current/Exs/Never/unknown 1/11/146/9 1/9/83/0 Clinical activity Mild 64 (38.3) 25 (26.9) Moderate 94 (56.3) 65 (69.9) Severe 9 (5.4) 3 (3.2) Clinical symptoms Abdominal pain 133 (79.6) 70 (75.3) Diarrhea 77 (46.1) 49 (52.7) Weight loss 65 (38.9) 39 (41.9) Fever 91 (54.5) 40 (43.0) Cough 17 (10.2) 8 (8.6) Sputum 0 0 0 0 Breathlessness 5 (3.0) 3 (3.2)
Note: Data in parentheses are percentages.
Exs- ex-smoker.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Thoracic CT Findings in Patients with Ulcerative Colitis
Findings Activity Mild ( n = 64) Moderate ( n = 94) Severe ( n = 9)P Value Ground-glass opacity 10 (15.6) 14 (14.9) 0 (0) NS Consolidation 1 (1.6) 0 (0) 0 (0) NS Bronchial wall thickening 16 (25.0) 33 (35.1) 4 (44.4) NS Centrilobular nodules 35 (54.7) 42 (44.7) 5 (55.6) NS Crazy-paving appearance 0 (0) 0 (0) 0 (0) NS Nodules 6 (9.4) 11 (11.7) 0 (0) NS Bronchiectasis 0 (0) 4 (4.3) 0 (0) NS Interlobular septal thickening 0 (0) 4 (4.3) 0 (0) NS Cysts 2 (3.1) 0 (0) 0 (0) NS Lymph node enlargement 0 (0) 0 (0) 0 (0) NS Pleural effusion 1 (1.6) 2 (2.1) 1 (11.1) NS CT diagnostic pattern NSIP 0 (0) 3 (3.2) 0 (0) NS OP 1 (1.6) 8 (8.5) 0 (0) NS UIP 0 (0) 1 (1.1) 0 (0) NS Indeterminate 2 (3.1) 2 (2.1) 0 (0) NS
Data in parentheses are percentages.
CT, computed tomography; NS, not significant; NSIP, nonspecific interstitial pneumonia; OP, organizing pneumonia; UIP, usual interstitial pneumonia.
TABLE 3
Thoracic CT Findings in Patients with Crohn Disease
Findings Activity Mild ( n = 25) Moderate ( n = 65) Severe ( n = 3)P Value Ground-glass opacity 0 (0) 8 (12.3) 0 (0) NS Consolidation 1 (4.0) 1 (1.5) 0 (0) NS Bronchial wall thickening 14 (56.0) 35 (53.8) 2 (66.7) NS Centrilobular nodules 15 (60.0) 25 (38.5) 2 (66.7) NS Crazy-paving appearance 0 (0) 0 (0) 0 (0) NS Nodules 1 (4.0) 3 (4.6) 0 (0) NS Bronchiectasis 0 (0) 1 (1.5) 0 (0) NS Interlobular septal thickening 0 (0) 0 (0) 1 (33.3) NS Cysts 0 (0) 1 (1.5) 0 (0) NS Lymph node enlargement 1 (4.0) 1 (1.5) 0 (0) NS Pleural effusion 0 (0) 1 (1.5) 0 (0) NS CT diagnostic pattern NSIP 1 (4.0) 1 (1.5) 0 (0) NS OP 0 (0) 4 (6.2) 0 (0) NS UIP 0 (0) 0 (0) 0 (0) NS Indeterminate 0 (0) 3 (4.6) 0 (0) NS
Data in parentheses are percentages.
CT, computed tomography; NS, not significant; NSIP, nonspecific interstitial pneumonia; OP, organizing pneumonia; UIP, usual interstitial pneumonia.
Get Radiology Tree app to read full this article<
CT Patterns
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Thoracic CT Findings for Each Type of Disease
Findings Ulcerative Colitis ( n = 167) Crohn Disease ( n = 93)P Value Ground-glass opacity 24 (14.4) 8 (8.6) NS Consolidation 1 (0.6) 2 (2.1) NS Bronchial wall thickening 53 (31.7) 51 (54.8) <.001 Centrilobular nodules 82 (49.1) 42 (45.2) NS Crazy-paving appearance 0 (0) 0 (0) NS Nodules 17 (10.2) 4 (4.3) NS Bronchiectasis 4 (2.4) 1 (1.1) NS Interlobular septal thickening 4 (2.4) 1 (1.1) NS Cysts 2 (1.2) 1 (1.1) NS Lymph node enlargement 0 (0) 2 (2.2) NS Pleural effusion 4 (2.4) 1 (1.1) NS CT diagnostic pattern NSIP 3 (1.8) 2 (2.2) NS OP 9 (5.4) 4 (4.3) NS UIP 1 (0.6) 0 (0) NS Indeterminate 4 (2.4) 3 (3.2) NS
Data in parentheses are percentages.
CT, computed tomography; NS, not significant; NSIP, nonspecific interstitial pneumonia; OP, organizing pneumonia; UIP, usual interstitial pneumonia.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Disease Distribution
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Follow-up Study
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Levine J.B., Lekawski-Trubish D.: Extraintestinal considerations in inflammatory bowel disease. Gastroenterol Clin North Am 1995; 24: pp. 633-646.
2. Kraft S.C., Earle R.H., Roesler M., et. al.: Unexplained bronchopulmonary disease with inflammatory bowel disease. Arch Intern Med 1976; 136: pp. 454-459.
3. Tunc B., Filik L., Bilgic F., et. al.: Pulmonary function tests, high-resolution computed tomography findings and inflammatory bowel disease. Acta Gastroenterol Belg 2006; 69: pp. 255-260.
4. Yilmaz A., Yilmaz Demirci N., Hosgun D., et. al.: Pulmonary involvement in inflammatory bowel disease. World J Gastroenterol 2010; 16: pp. 4952-4957.
5. Raghu G., Collard H.R., Egan J.J., et. al.: An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am J Respir Crit Care Med 2011; 183: pp. 788-824.
6. Travis W.D., Costabel U., Hansell D.M., et. al.: An official American Thoracic Society/European Respiratory Society statement: update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med 2013; 188: pp. 733-748.
7. Hansell D.M., Bankier A.A., MacMahon H., et. al.: Fleischner Society: glossary of terms for thoracic imaging. Radiology 2008; 246: pp. 697-722.
8. Songur N., Songur Y., Tuzun M., et. al.: Pulmonary function tests and high-resolution CT in the detection of pulmonary involvement in inflammatory bowel disease. J Clin Gastroenterol 2003; 37: pp. 292-298.
9. Tzanakis N., Samiou U.M., Bouros D., et. al.: Small airways function in patients with inflammatory bowel disease. Am J Respir Crit Care Med 1998; 157: pp. 382-386.
10. Tokuda H., Harigai M., Kameda H., et. al.: Consensus statement for medical practice: biological agents and lung disease [Abridged English translation by the Japanese Respiratory Society]. Respir Investig 2017; 55: pp. 229-251.
11. Fidder H., Schnitzler F., Ferrante M., et. al.: Long-term safety of inflizimab for the treatment of inflammatory bowel disease: a single center cohort study. Gut 2009; 58: pp. 501-508.
12. Keane J.: Tumor necrosis factor blockers and reactivation of latent tuberculosis. Clin Infect Dis 2004; 39: pp. 300-302.
13. Garcia-Vidal C., Rodriguez-Fernandez S., Teijon S., et. al.: Risk factors for opportunistic infection in infliximab-treated patients: the importance of screening in prevention. Eur J Clin Microbiol Infect Dis 2009; 28: pp. 3310-3317.
14. Jones J.L., Loftus E.V.: Lymphoma risk in inflammatory bowel disease: is it the disease or its treatment?. Inflamm Bowel Dis 2007; 13: pp. 1299-1307.
15. Camus P., Piard F., Ashcroft T., et. al.: The lung in inflammatory bowel disease. Medicine (Baltimore) 1993; 72: pp. 151-183.
16. Shneerson J.M.: Steroid-responsive alveolitis associated with ulcerative colitis. Chest 1992; 101: pp. 585-586.
17. Mahadeva R., Walsh G., Flower C.D., et. al.: Clinical and radiological characteristics of lung disease in inflammatory bowel disease. Eur Respir J 2000; 15: pp. 41-48.
18. Wilcox P., Miller R., Miller G., et. al.: Airway involvement in ulcerative colitis. Chest 1987; 92: pp. 18-22.
19. Forrest J.A., Sherman D.J.: Pulmonary vasculitis and ulcerative colitis. Am J Dig Dis 1975; 20: pp. 482-486.
20. Swinburn C.R., Jackson G.J., Cobden I., et. al.: Bronchiolitis obliterans organizing pneumonia in a patient with ulcerative colitis. Thorax 1988; 43: pp. 735-736.
21. Dodd J.D., de Jong P.A., Levy R.D., et. al.: Conventional high-resolution CT versus contiguous multidetector CT in the detection of bronchiolitis obliterans syndrome in lung transplant recipients. J Thorac Imaging 2008; 23: pp. 235-243.
22. Garg K., Lynch D.A., Newell J.D.: Inflammatory airways disease in ulcerative colitis: CT and high-resolution CT features. J Thorac Imaging 1993; 8: pp. 159-163.
23. Spira A., Grossman R., Balter M.: Large airway disease associated with inflammatory bowel disease. Chest 1998; 113: pp. 1723-1726.
24. Okada F., Ando Y., Yoshitake S., et. al.: Clinical/pathologic correlation in 553 patients with primary centrilobular findings on high-resolution scan of the thorax. Chest 2007; 132: pp. 1939-1948.
25. Casey M.B., Tazelaar H.D., Myers J.L., et. al.: Noninfectious lung pathology in patients with Crohn’s disease. Am J Surg Pathol 2003; 27: pp. 213-219.
26. Okada F., Ando Y., Wakisaka M., et. al.: Chlamydia pneumoniae pneumonia and Mycoplasma pneumoniae pneumonia: comparison of clinical findings and CT findings. J Comput Assist Tomogr 2005; 29: pp. 626-632.
27. Okada F., Ando Y., Tanoue S., et. al.: Radiological findings in acute Haemophilus influenzae pulmonary infection. Br J Radiol 2012; 85: pp. 121-126.
28. Okada F., Ando Y., Nakayama T., et. al.: Pulmonary thin-section CT findings in acute Moraxella catarrhalis pulmonary infection. Br J Radiol 2011; 84: pp. 1109-1114.
29. Morikawa K., Okada F., Ando Y., et. al.: Meticillin-resistant Staphylococcus aureus and meticillin-susceptible S. aureus pneumonia: comparison of clinical and thin-section CT findings. Br J Radiol 2012; 85: pp. e168-e175.
30. Okada F., Ando Y., Matsushita S., et. al.: Thin-section computed tomography findings of patients with acute Streptococcus pneumoniae pneumonia with and without concurrent infection. Br J Radiol 2012; 85: pp. e357-e364.
31. Okada F., Ando Y., Honda K., et. al.: Clinical and pulmonary thin-section CT findings in acute Klebsiella pneumoniae pneumonia. Eur Radiol 2009; 19: pp. 809-815.
32. Okada F., Ando Y., Honda K., et. al.: Acute Klebsiella pneumoniae pneumonia alone and with concurrent infection: comparison of clinical and thin-section CT findings. Br J Radiol 2010; 83: pp. 854-860.
33. Okada F., Ono A., Ando Y., et. al.: High-resolution CT findings in Streptococcus milleri pulmonary infection. Clin Radiol 2013; 68: pp. e331-e337.
34. Sommer H., Schmidt M., Gruber K.D.: Pulmonary functional disorders in ulcerative colitis and Crohn’s disease. Dtsch Med Wochenschr 1986; 111: pp. 812-815.